










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 n.10 Madrid Oct. 2017
https://dx.doi.org/10.17235/reed.2017.4893/2017
PICTURES IN DIGESTIVE PATHOLOGY
Hemosuccus pancreaticus secondary to pseudoaneurysm of the splenic artery
Hemosuccus pancreáticus secundario a pseudoaneurisma de la arteria esplénica
Mariano José Parada-Blázquez1 and Andrea Núñez-Ortiz2
Departments of 1Radiology and 2Gastroenterology. Hospital Universitario Virgen del Rocío. Sevilla, Spain
A 41 year old male and current smoker was evaluated using standard tests (blood analysis, X-ray, abdominal ultrasound, endoscopy) due to a prior history of severe epigastric abdominal pain that often required medical assistance.
He was admitted to the Emergency Department with discomfort, vomiting and rectal bleeding with acute anemia (from 165 g/dl to 65 g/dl). Neither gastroscopy nor colonoscopy identified any potential cause of the bleeding. The computed tomography (CT) showed a 70 x 31 mm pseudoaneurysm of the splenic artery with no evidence of other causes (i.e. pancreatitis) (Fig. 1). Thus, an arteriography was performed (Fig. 2) to embolize and generate pseudoaneurysm exclusion.

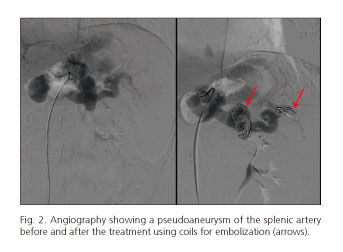
The gastrointestinal bleeding was attributed to a hemosuccus pancreaticus secondary to the pseudoaneurysm of the splenic artery, which could be related to a non-adverted episode of acute pancreatitis.
Discussion
Pseudoaneurysm of the splenic artery is usually secondary to splenic trauma, fungal infections and chronic or acute pancreatitis (1). It differs from aneurysms due to the absence of a complete arterial wall. Usually pain or gastrointestinal bleeding is the presenting symptoms due to the erosion to a viscera or pancreatic ductus. Typically, CT scan shows an evagination of the splenic artery (including ramifications) that is filled with contrast surrounded by a hematoma.
Due to the risk of a rupture, the treatment is mandatory irrespective of the size or symptoms. The coil embolization (both distal and proximal through the neck of the pseudoaneurysm) and the placement of a stent are the standard therapy for pseudoaneurysms (2,3).
References
1. Mandaliya R, Krevsky B, Sankineni A, et al. Hemosuccus pancreaticus: A mysterious cause of gastrointestinal bleeding. Gastroenterology Research 2014;7(1):32-7. DOI: 10.14740/gr596w. [ Links ]
2. Loffroy R, Favelier S, Pottecher P, et al. Endovascular management of visceral artery aneurysms: When to watch, when to intervene? World Journal of Radiology 2015;287(7):143-8. DOI: 10.4329/wjr.v7.i7.143. [ Links ]
3. Duan XH, Ren JZ, Zhou GF, et al. Clinical features and endovascular treatment of visceral artery pseudoaneurysms. Ann Vasc Surg 2015;29(3):482-90. DOI: 10.1016/j.avsg.2014.11.008. [ Links ]
