










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 no.11 Madrid nov. 2017
https://dx.doi.org/10.17235/reed.2017.4983/2017
PICTURES IN DIGESTIVE PATHOLOGY
An intrahepatic cavoportal collateral pathway due to a liver hydatid cyst obstructing the inferior vena cava
Shunt intrahepático portocava en paciente con quiste hidatídico que comprime vena cava inferior
Alba Manuel-Vázquez1, José Manuel Ramia-Ángel1, Luis Gijón2 and Roberto de-la-Plaza-Llamas1
Services of 1General and Digestive Surgery, and 2Radiodiagnosis. Hospital Universitario de Guadalajara. Guadalajara, Spain
We present the case of a 47-year-old female with a previous consumption of hashish and cocaine and HIV infection with an undetectable viral load.
She presented with fever, right upper quadrant pain and a three finger hepatomegaly. The analytical results showed 12,800 cells/l, alkaline phosphatase at 251 IU/l, GGT of 178 IU/l and CRP at 156 mg/l.
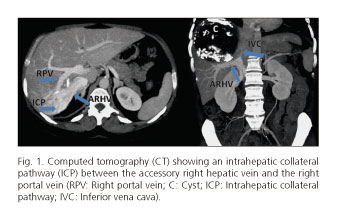
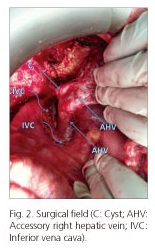
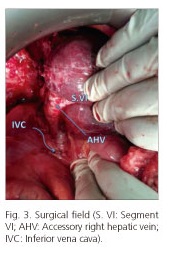
The abdominal computed tomography (CT) showed a hydatid cyst of 11.5 cm occupying segments VII-VIII that communicated with the biliary tree and compressed 10 cm of the inferior vena cava (IVC) (Fig. 1). In addition, an intrahepatic collateral pathway (ICP) of 3 cm between the accessory right hepatic vein and the right portal vein was observed (Figs. 2 and 3). The Echinococcus serology was positive (1/1,280).
A percutaneous drainage was performed and Streptococcus oralis grew in the culture.
The endoscopic retrograde cholangiopancreatography (ERCP) showed cystobiliary communication, cyst material in the biliary tree and a papillary stenosis. The bile duct was cleaned and the papilla dilated. A subtotal cystectomy was performed leaving a small patch of the cyst attached to the IVC. The patient was discharged on postoperative day 4 without complications.
Discussion
When there is a chronic obstruction of the IVC, this leads to collateral formation between the IVC and a tributary vein of the portal system (1).
These shunts can be extrahepatic or, more infrequently, intrahepatic (1,2). In our case, we did not know if this ICP was congenital and had grown as a consequence of the compression in the IVC, or if it developed de novo.
The liver sometimes has accessory right hepatic veins called middle right or inferior right vein. They are present in 15%-47% of cases and only 3-12% have a wider caliber than the right hepatic vein (3).
References
1. Tsitouridis I, Sotiriadis C, Michaelides M, et al. Intrahepatic portosystemic venous shunt: Radiological evaluation. Diagn Interv Radiol 2009;15:182-7. [ Links ]
2. Kapur S, Paik E, Rezaei A, et al. Where there is blood, there is the way: Unusual collateral vessels in superior and inferior vena cava obstruction. Radiographics 2010;30:67-78. DOI: 10.1148/rg.301095724. [ Links ]
3. Hanaoka J, Shimada M, Uchiyama H, et al. A simple formula to calculate the liver drainage volume of the accessory right hepatic vein using its diameter alone. Surgery 2009;146:264-8. DOI: 10.1016/j.surg.2009.06.004. [ Links ]
