










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 no.12 Madrid dic. 2017
https://dx.doi.org/10.17235/reed.2017.5246/2017
LETTERS TO THE EDITOR
A rare cause of upper gastrointestinal bleeding in a patient with end stage renal disease: gastric amyloidosis
Key words: Gastric amyloidosis. End stage renal disease. Upper gastrointestinal system bleeding.
Dear Editor,
This letter has two purposes, firstly to evaluate the correlation between our endoscopic findings of gastric amyloidosis with the previous report by Vargas et al. (1). Secondly, to draw attention to the fact that amyloidosis may occur in upper gastrointestinal bleeding (UGIB) in patients with end-stage renal disease (ESRD).
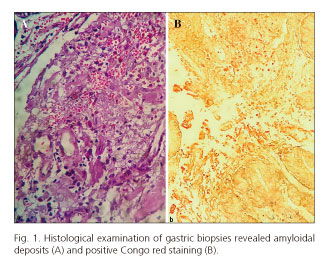
A 55 year old man who had ESRD at 15 years old was presented to our hospital with hematemesis and melena. There was no evidence of rheumatological, hematological or other systemic disease. Hypotension, melena, decreased hemoglobin levels and high creatinine levels were detected. Fluid resuscitation, a blood transfusion and intravenous pantoprazole were initiated. An upper gastrointestinal endoscopy showed an irregular, malignant-appearing ulcer of 25 x 30 mm in size with an adherent blood clot in the antrum incisura angularis. Erythematous, polypoid, fragile lesions and mucosal thickening were seen at the edge of the ulcer. Gastric malignancy was suspected during the differential diagnosis. A new endoscopy was performed two days later and biopsy samples were obtained. Histological examination revealed amyloidal deposits (Fig. 1A) and positive Congo red staining (Fig. 1B). The patient was discharged after 7 days in the hospital.
This is the first reported case of ESRD and gastric amyloidosis presenting with UGIB. UGIB is a frequent complication of ESRD. The most common causes of bleeding are peptic ulcer disease, severe ulcerative esophagitis, duodenitis and angiodysplasia (2). Gastrointestinal involvement is uncommon in patients with amyloidosis and the reported risk is only about 3% (3). In this case, location and endoscopic features of gastric amyloid deposits were in accordance with the findings of Vargas et al. (1). Gastric amyloidosis should be kept in mind in patients with UGIB and ESRD.
Ufuk Kutluana
Division of Gastroenterology and Internal Medicine.
Denizli State Hospital. Denizli, Turkey
References
1. Vargas AA, Carnerero EL, Mercedes NR, et al. Correlation between location of amyloid deposits and endoscopic and clinical manifestations in symptomatic gastrointestinal amyloidosis. Rev Esp Enferm Dig 2015;107(1):49-51. [ Links ]
2. Boyle JM, Johnston B. Acute upper gastrointestinal hemorrhage in patients with chronic renal diseases. Am J Med 1983;75:409-12. DOI: 10.1016/0002-9343(83)90341-8. [ Links ]
3. Cowan AJ, Skinner M, Seldin DC, et al. Amyloidosis of the gastrointestinal tract: a 13-year, single-center, referral experience. Haematologica 2013;98(1):141-6. DOI: 10.3324/haematol.2012.068155. [ Links ]
