










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Submucosal tumors (SMTs) refer to a protuberant lesion covered with intact mucosa. The majority of SMTs found in the stomach are small and asymptomatic. Half of gastric SMTs are considered to be gastrointestinal stromal tumors (GIST) with malignant potential, especially large lesions 1. Periodical surveillance by esophagogastroduodenoscopy (EGD) and endoscopic ultrasonography (EUS) is performed for SMTs of < 2 cm. However, this raises issues with regard to the compliance and stress levels of the patient, cost-effectiveness and the risk associated with repeated endoscopic procedures and a delayed diagnosis of malignancy 1) (2. Therefore, it is necessary to remove SMTs and endoscopic resection is an alternative method 3) (4. Endoscopic full-thickness resection (EFTR) has proved to be a safe and effective endoscopic method for the treatment of gastric fundus SMTs that originate from the muscularis propria (MP) layer, with a high rate of complete resection 5) (6) (7) (8) (9) (10. Submucosal tunneling endoscopic resection (STER) is a novel endoscopic technique and has been shown to be safe and effective for the treatment of gastric SMTs 11) (12) (13) (14. However, there is little data that compares STER and EFTR for the treatment of SMTs in the gastric fundus. In this retrospective study, we aimed to compare both endoscopic techniques for the treatment of gastric fundus SMTs.
MATERIALS AND METHODS
Patients
This was a single center, retrospective study conducted in China. The study was approved by the ethics committee of the Second Xiangya Hospital of the Central South University. All participants signed an informed consent for this retrospective study. The inclusion criteria were as follows: a) presence of gastric fundus SMTs originating from the MP layer confirmed by upper endoscopy (EGD), endoscopic ultrasound (EUS) and/or computerized tomography (CT); b) EUS with no high-risk features of malignancy such as an irregular border, internal heterogeneity and heterogeneous enhancement; c) no signs of metastasis or invasion outside the gastrointestinal tract during CT examination; d) a tumor size of 2-3.5 cm or SMTs < 2 cm with strong grounds for resection according to the patients' wishes; and e) consent to undergo an STER or EFTR procedure at our hospital. Cases that could not tolerate anesthesia and those with severe cardiopulmonary disease or blood coagulation disorders (international normalized ratio > 2.0, platelet count < 100,000/mm3) were excluded from the study. Forty-three consecutive patients were enrolled into the study between April 2011 and May 2016. Cases only underwent EFTR from April 2011 to June 2012, as STER was not performed for SMTs. After this period, some cases underwent STER while others underwent EFTR according to the patient's preference, after being informed of the merits and disadvantages of each technique. Demographic data (age, gender), tumor size, procedure-related parameters, complications, hospital stay, cost and follow-up data were retrospectively collected and recorded for all cases.
Equipment for STER and EFTR
Both STER and EFTR were performed under general anesthesia via tracheal intubation. A carbon dioxide insufflator (UCR; Olympus) was used in all procedures. Other equipment and accessories included a high-frequency generator (ENDO CUT(r) Q 3-2-3, VIO 200D, ERBE, Tübingen, Germany), an argon plasma coagulation unit (APC300; ERBE), a hybrid knife (ERBE), a dual knife (KD-650Q; Olympus), an insulation-tip knife (KD611L, IT2; Olympus), an injection needle (NM-4L-1; Olympus) and hemostatic clips (HX-600-90; Olympus).
STER procedure
STER was performed as previously reported 14. Briefly, the procedure was as follows: a) identification of the SMT; b) submucosal injection at about 3-5 cm proximal to the SMT; c) a longitudinal mucosal incision was made to create the tunnel entry; d) a submucosal tunnel was made between the submucosal and the MP layers; e) dissection of the tumor with an insulation-tip knife, a hybrid knife or a dual knife; and f) closure of the mucosal entry with metallic clips 11. Figure 1 depicts the STER procedure.
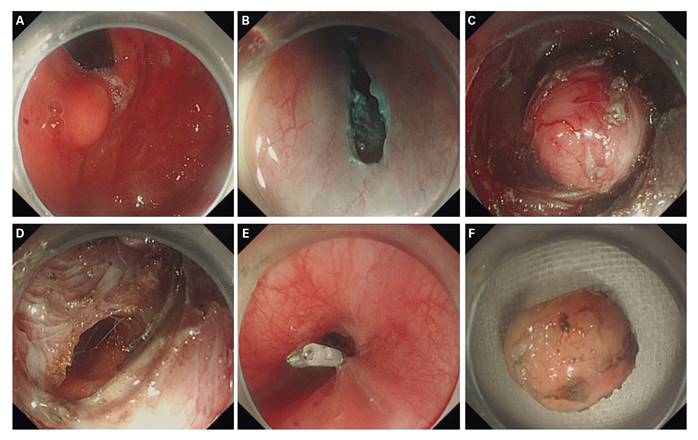
Fig. 1 Case illustration of the submucosal tunneling endoscopic resection. A. Endoscopy showed a submucosal tumor in the gastric fundus. B. Longitudinal mucosal incision to make a tunnel entry. C. Submucosal tumor in the submucosal tunnel. D. Wound surface after removal of the tumor. E. The tunnel entry was closed with several clips. F. Resected tumor.
EFTR procedure
EFTR was performed as previously reported 5: a) submucosal injection and precutting of the mucosal and submucosal layer around the lesion; b) circumferential incision as deep as the MP layer around the lesion using the endoscopic submucosal dissection (ESD) technique; c) incision into the serosal layer around the lesion; d) full-thickness resection of the tumor, including the serosal layer, without laparoscopic assistance; and e) closure of the gastric-wall defect with metallic clips 5. A gastric tube was placed after the procedure. Figure 2 depicts the EFTR procedure.

Fig. 2 Case illustration of an endoscopic full-thickness resection. A. Protruding submucosal tumor in the gastric fundus. B. A circumferential incision was made as deep as the muscularis propria layer around the lesion. C. An incision was made into the serosal layer around the lesion to create an active perforation. D. Wound surface after removal of the tumor. E. The gastric wall defect was closed with several clips. F. Resected tumor.
Postoperative management
All the patients were asked to maintain a semi-reclined position for three days. Intravenous proton pump inhibitor (PPI) and antibiotics were administered for three days and then oral PPI for four weeks.
With regard to patients that underwent STER, they were kept nil per os (NPO) for 48 h, on a liquid diet for three days and returned gradually to a normal diet within two weeks. With regard to cases who underwent EFTR, they were kept NPO for at least 72 h, on a liquid diet for five days and returned gradually to a normal diet within two weeks.
Clinical symptoms were monitored postoperatively, including fever, chest/abdominal pain, vital sign, chest/abdominal sign, melena, hematemesis, etc.
Laboratory tests, including blood routine as well as imageological examination such as thoracoabdominal radiography, contrast roentgenography and ultrasound, were performed postoperatively. A CT scan was performed for patients with a suspicion of leakage or chest/abdominal infection, etc.
Definition and assessment
En bloc resection: the intact fibrous capsule of the resected tumor and the absence of any remnant of tumor by endoscopy.
Suture time: the time point from insertion of the first clip to a complete closure of the defect.
Complications: incidences that occurred intraoperatively or postoperatively such as pain/discomfort, fever, bleeding, perforation, leakage, infection and emphysema, etc. A severe complication was defined as an incident that required a blood transfusion, endoscopic or surgical intervention and resulted in an extended length of hospital stay and a greater hospital cost.
Postoperative hospital stay: from the day of the operation to the day of discharge, the duration of the preoperative evaluation was not included.
Pathological evaluation: the specimens were fixed, embedded with paraffin and sectioned. Hematoxylin and eosin and immunohistochemical staining (SMA, Ki67, CD34, CD117, S-100, desmin, Dog-1, etc.) were carried out to determine the characteristic of the SMTs.
Follow-up
When patients were discharged from hospital, a notification was sent in order to inform the patient of the follow-up surveillance. In addition, nurses from our department would call patients to remind them of the upcoming examination appointment. Surveillance EGD was performed at one, three, six, and 12 months, and annually thereafter, in order to observe wound healing and to check for any residual tumor. An additional EUS was recommended in the case of any suspicious residue or recurrence.
Statistical analysis
The SPSS 21.0 software was used for data analysis. Continuous variables were presented as a mean ± standard deviation and analyzed using the Student's t test. Qualitative data were presented as frequencies and calculated using the Chi-squared test or Fisher's exact test. A two-tailed p value < 0.05 was considered as statistically significant.
RESULTS
Clinical characteristics and therapeutic outcomes
Forty-three patients were enrolled into the study from April 2011 to May 2016, the mean age was 51.7 years (range 26-65 years) and the male/female ratio was 18/25. All 43 SMTs were located at the gastric fundus, the mean operation time was 67.6 minutes (range 25-160 minutes) and the mean diameter was 16.6 mm (range 5-40 mm). Around a quarter of patients in both groups had a tumor of < 2 cm. Endoscopic resection was performed based on a strong desire for removal by the patient. With regard to a pathological diagnosis, 36 SMTs were GIST (15 were very low risk and 21 were low risk on the basis of the National Comprehensive Cancer Network guidelines 15)), six were leiomyoma and one was a schwannoma.
Fifteen of 43 cases underwent STER and the remaining 28 cases underwent EFTR. There were no significant differences between the two groups in terms of gender, age, concomitant diseases, operation time, tumor size and cost (p > 0.05) (Table 1). However, patients in the STER group had a shorter suture time, a smaller number of clips were required for closure and postoperative hospital stay was shorter (p < 0.05) (Table 1). En bloc resection was achieved in 93.3% (14/15) of the patients in the STER group and 96.4% (27/28) of the patients in the EFTR group, and the difference was not statistically significant (p > 0.05) (Table 1).
Complications and follow-up results
A mucosa perforation was found intraoperatively in one case (6.7%) in the STER group, which was closed with two clips without subsequent leakage. Four cases (14.3%) in the EFTR group experienced complications, one patient had delayed bleeding and three patients had abdominal pain/discomfort and a fever < 38.5 °C. The case with delayed bleeding had a persistent hemoglobin disorder and abdominal pain but no hematemesis or melena. EGD did not identify bleeding in the stomach or leakage. A laparoscopy was performed in order to identify the bleed, which was on the serosal surface of the surgical site and was successfully managed by suturing. With regard to the three cases with abdominal pain/discomfort and a fever < 38.5 °C, none of them had an abdominal cavity effusion on abdominal ultrasound and their symptoms subsided one to three days after EFTR with PPI and antibiotics. There was no significant difference between the two groups with regard to complications (p > 0.05) (Table 1). No recurrence was noted in the STER and EFTR groups during a mean follow-up of 12.1 and 22.8 months, respectively.

DISCUSSION
The present study demonstrated that the efficacy of STER and EFTR for the treatment of gastric fundus SMTs was comparable. However, STER offers advantages over EFTR such as a shorter suture time, a smaller number of clips required for closure and a shorter postoperative hospital stay. To the best of our knowledge, this is the first study comparing the safety and efficacy of STER and EFTR for gastric fundus SMTs.
Even though most of the SMTs found in the stomach are small and asymptomatic, the majority of the gastric fundus SMTs are GISTs which have malignant potential, especially if they are large 1. The primary aim of endoscopic removal in our study was to perform STER or EFTR for SMTs of 2-3.5 cm in size (tumors size was preoperatively measured by EUS or CT). Endoscopic resection was also performed for patients who have a strong desire for removal of SMTs < 2 cm, usually due to the stress of repeated endoscopic procedures and the risk of malignancy. It is worth mentioning that periodical surveillance still remains one of the recommended strategies for gastric SMTs < 2 cm.Endoscopic resection has been widely accepted as an alternative method for gastric SMTs originating from the MP layer and endoscopic options include ESD, endoscopic submucosal excavation (ESE), EFTR and STER 3) (4. ESD was used to treat gastric SMTs originating from the superficial MP layer. However, when the tumor originates from the deep MP layer or has a tight connection with the underlying MP layer or serosal layer, the complete resection rate decreases and the complication rate increases 4) (16) (17. Although ESE could improve the complete resection rate for gastric SMTs from the deep MP layer, it has some limitations for lesions with a tight connection with the serosal layer or with an extraluminal growth 4) (18.
EFTR was first reported by Suzuki and Ikeda 19 for the treatment of two rectal carcinoids and one duodenal carcinoid using a snaring technique. Ikeda et al. 20 also reported the use of the EFTR technique in a porcine model. Zhou et al. 5 first introduced this technique into the clinical practice in 2011. Twenty-six gastric SMTs originating from the MP layer were successfully removed by EFTR with a mean operation time of 105 minutes, an en bloc resection rate of 100% and a mean tumor size of 2.8 cm. No severe complications such as gastrointestinal bleeding, peritonitis, or abdominal abscess were found. Since then, additional clinical studies have confirmed its safety and efficacy for the treatment of gastric SMTs, including those located at the gastric fundus 6) (7) (8) (9) (10) (21. In the present study, 28 gastric fundus SMTs were removed by EFTR with an en bloc resection rate of 96.4%. Only 13.4% cases suffered complications and all were successfully managed, which is consistent with previous studies 6) (7) (8) (9) (10) (21.
One major concern with the EFTR technique is air/fluid leakage, specifically the passage of air or fluid through the gastric wall defect into the abdominal cavity. In addition, sufficient closure of the defect after a full-thickness resection is also very important 16. Incomplete closure of the gastric wall defect may lead to serious morbidity such as peritonitis, fever, abdominal and/or pelvic effusion, etc. Several endoscopic techniques have been reported for closure of the defect such as clips, endoloop and clips, over-the-scope-clips and endoscopic suturing devices. While most of these techniques require specialized equipment and demand a skillful handling, closure with clips is still widely accepted 6) (7) (8) (9) (16) (22) (23. In the present study, the defects of the 28 EFTR cases were all successfully closed with clips. Only three of them had suspicious air/fluid leakage symptoms which were successfully managed with conservative treatment. In our experience, several tips may help to promote defect closure as well as minimize subsequent complications. Firstly, it is important to prevent the gastric fluid from flowing into the abdominal cavity. The patients' position should be changed before performing a resection in order to obtain a satisfactory view of the tumor. Meanwhile, the operative field should be cleaned and clearly exposed by the removal of remnant fluid and gas in the stomach lumen in order for the incision to reach the serosal layer. Secondly, a sufficient closure of the defect needs to be obtained. When the defect is smaller than the width of the open clip, it should be closed in a "side-to-center" manner. When the defect is slightly larger than the width of the open clip, the defect should be closed using clips after a reduction of the diameter by air suction. Larger lesions can be managed by an omental-patch method, i.e., the defect is closed by clipping the gastric wall together with the omentum that was intentionally sucked into the gastric cavity 24) (25. Thirdly, a thorough postoperative management is required, such as maintaining a semi-reclined position postoperatively, using intravenous antibiotics and PPIs. Gastrointestinal decompression can also help to prevent peritoneal infection or reduce its effects. Lastly, contrast roentgenography should be performed to check for any leakage before eating food.
STER was initially used as a therapeutic technique for the treatment of esophageal and cardia SMTs 11) (26 in which a submucosal tunnel between the submucosal and MP layer is created to expose and dissect the SMT. Several retrospective studies have demonstrated its feasibility and efficacy for gastric fundus SMTs 12) (13. Lu et al. 12 applied this technique in 18 patients with gastric fundus SMTs with a total of 19 tumors (13 GISTs, six leiomyomas), and the mean tumor size was 21 mm (range 8-50 mm). All tumors were successfully removed and en bloc resection was achieved in all cases. Only two patients experienced complications that were resolved conservatively. Li et al. 13 reported 32 cases of gastric SMTs managed by STER without severe complications. An en bloc resection was achieved in all three cases with gastric fundus SMTs. In the present study, we successfully treated 15 cases of gastric fundus SMTs using the STER technique, and the en bloc resection rate was 93.3%. Besides, only one case suffered a complication that was alleviated by conservative treatment. This indicates that STER could be considered as a feasible therapeutic approach for gastric fundus SMTs, which is consistent with previous studies.
The main advantage of the STER technique is to maintain the integrity of the gastrointestinal mucosa and to promote wound healing in order to reduce the duration of NPO and avoid gastrointestinal decompression 27) (28. A 3-5 cm long submucosal tunnel functions as a good "leak-proof structure" and could reduce the potential risk of gastrointestinal tract leakage (air and/or fluid) and prevent secondary infection. Wang et al. 29 demonstrated that STER has advantages over ESD in terms of promoting a rapid wound healing and reducing the operating time and hospital stay without compromising the success rate or increasing complications. With regard to SMTs > 10 mm, STER is the preferable choice compared with ESE with regard to the prevention of air leakage symptoms 30. However, little is known about how the STER and EFTR procedures compare for the treatment of gastric fundus SMTs. In the present study, we found that the efficacy of STER and EFTR for the treatment of gastric fundus SMTs was comparable. However, STER has a shorter suture time and a smaller number of clips are required for closure, which implies that it could be easier to close the gastric wall defect using the STER technique. The reason may be the larger tension of the suture surface during the EFTR procedure as the MP and serosal layer immediately underlying the wound is lacking. In addition, our results showed per-protocol can be achieved using the STER technique that shortened NPO time in order to reduce postoperative stay, and no significant differences were observed with regard to the complication rate. Even though no statistical differences were found in our small sample size study, the complication rate for STER was lower. Three of 28 cases in the EFTR group experienced abdominal pain/discomfort and a fever < 38.5 °C. No cases within the STER group experienced this type of complication, which may be due to local infection caused by gas and liquid infiltration during EFTR.
The present study has several limitations. Firstly, this was a single center, retrospective study. Secondly, the sample size was relatively small, with only 43 cases enrolled. Thus, a large-scale validation study is required. Thirdly, although STER would theoretically promote wound healing compared to EFTR, frequent endoscopic surveillance was not performed during the first three months after treatment. Thus, it was not possible to provide the accurate wound healing time. Finally, all patients with SMTs underwent EFTR from April 2011 to June 2012 as STER was not performed before June 2012 in our center. Therefore, there may be a potential selective bias in that more patients were enrolled into the EFTR group.
In conclusion, our study shows that the efficacy of STER and EFTR for the treatment of gastric fundus SMTs was comparable. However, STER offers advantages over EFTR in terms of a shorter suture time, a smaller number of clips required for closure and a shorter postoperative hospital stay. Randomized, large-scale studies are warranted for a more definitive conclusion.
