










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.110 n.3 Madrid Mar. 2018
https://dx.doi.org/10.17235/reed.2018.5367/2017
LETTERS TO THE EDITOR
The morphological and functional diagnosis of a rare entity: lipomatous pseudohypertrophy of the páncreas
1Servicio de Radiodiagnóstico. Hospital Clínico Santiago de Compostela. Santiago de Compostela, A Coruña, España
Key words: Magnetic resonance; Cholangiopancreatic; Secretin; Pancreas; Lipomatous pseudohypertrophy
Dear Editor,
Lipomatous pseudohypertrophy of the pancreas (PLP) is a rare entity with an uncertain etiology that occurs due to a focal or diffuse replacement of the pancreatic parenchyma by mature adipose tissue 1) (2.
The clinical manifestation is non-specific and abdominal pain and/or steatorrhea are the most frequent symptoms. Nevertheless, there a few characteristics that lead to a diagnosis. These include: a) an increase in size and weight of the pancreas due to replacement by adipose tissue; b) a practically complete absence of the exocrine function of the pancreas; and 3) the preservation of the ductal system and the islets of Langerhans. These findings can be confirmed by imaging techniques 1) (2.
Case report
We present the case of a 72-year-old woman with a colicky abdominal pain in the right hypochondria of a duration of several months and a weight loss of 10 kg. Echoendoscopy identified a heterogeneous pancreatic parenchyma with areas of a lobular pattern and hyperechoic stripes and a normal Wirsung. The abdominal-pelvic computed tomography (CT) showed an increase in the size of the pancreas with an almost complete replacement of the parenchyma by adipose tissue (Fig. 1A). After the administration of secretin, a cholangiopancreatic MRI showed a fatty infiltration and a normal pancreatic duct with an adequate distension. The secretin confirmed a correct distension of the Wirsung duct, which had returned to its normal caliber, and a reduced exocrine function as there was only a small amount of duodenal filling (Fig. 1B-D).
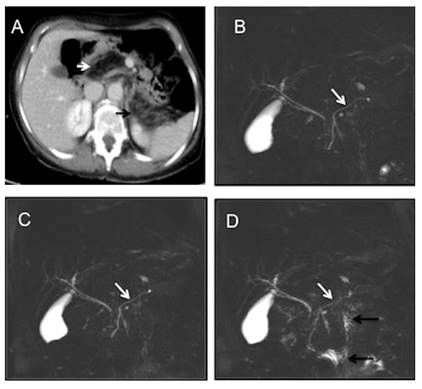
Fig. 1 A. CT. Axial MIP reconstruction: fatty replacement of the pancreatic parenchyma (white arrow: pancreas head-neck; black arrow: pancreas tail). B-D. Cholangiopancreatic MR coronal images. B. Basal image that identifies a normal pancreatic conduct (white arrow). C. One minute after secretin injection, the pancreatic conduct (white arrow) is at its widest point of dilatation. D. Late image (ten minutes) shows a reduction in the pancreatic duct caliber (white arrow) in relation to C and a small amount of signal intensity in the small bowel due to a poor exocrine function (black arrows).
Discussion
Among the available imaging techniques, a cholangiopancreatic MRI with secretin is the technique of choice due to its ability to provide morphological information and also functional data of the ductal system. This technique is also able to assess the exocrine function in a semi-quantitative manner 3) (4) (5.
A few differential diagnoses should be considered, as this condition can be confused with a lipoma or liposarcoma when presenting in a focal manner. However, when there is a diffuse involvement of the pancreas, it should be differentiated from chronic pancreatitis, cystic fibrosis and pancreatic lipomatosis. The possibility of diagnosing PLP by a non-invasive imaging technique, allows a conservative management of this condition.
Bibliografía
1. Altinel D, Basturk O, Sarmiento JM, et al. Lipomatous pseudohypertrophy of the pancreas: A clinicopathologically distinct entity. Pancreas 2010;39:392-7. DOI: 10.1097/MPA.0b013e3181bd2923 [ Links ]
2. Beresford OD, Owen TK. Lipomatous pseudohypertrophy of the pancreas. J Clin Path 1957;10:63-6. DOI: 10.1136/jcp.10.1.63 [ Links ]
3. Sandrasegaran K, Lin C, Akisik FM, et al. State-of-the-art pancreatic MRI. AJR 2010;195:42-53. DOI: 10.2214/AJR.10.4421 [ Links ]
4. Akisik MF, Sandrasegaran K, Aisen AA, et al. Dynamic secretin-enhanced MR cholangiopancreatography. RadioGraphics 2006;26:665-77. DOI: 10.1148/rg.263055077 [ Links ]
5. Sanyal R, Stevens T, Novak E, et al. Secretin-enhanced MRCP: Review of technique and application with proposal for quantification of exocrine function. AJR 2012;198:124-32. DOI: 10.2214/AJR.10.5713 [ Links ]
