










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Spontaneous hepatic rupture was first described in 1844 by Abercrombie J. 1 and nowadays remains a rare condition associated with a high mortality rate and without standardized treatment 2. The condition results from a breach in the hepatic parenchyma that occurs without an external cause. It is an acute surgical emergency and often presents with non-specific signs and symptoms that require an early diagnosis and multidisciplinary management 3. Dietary supplements and anabolic androgenic steroids (AAS) are commonly used by bodybuilders to enhance physique and improve performance levels. This has resulted in an increasingly common source of drug-induced liver injury 4. We report the case of a spontaneous hepatic rupture and life-threatening hemorrhage in a young bodybuilder with a history of clenbuterol and ephedrine alkaloids use.
CASE REPORT
A 32-year-old man presented to the Emergency Department with sudden mid-epigastric pain and vomiting in absence of any recent history of trauma. The patient was a metalworker and competitive bodybuilder. He was on a hyperproteic diet and reported the use of a combination of clenbuterol and ephedrine alkaloids that were purchased on the internet. Physical examination identified mid-epigastric tenderness and tender hepatomegaly. Blood tests showed bilirubin levels of 0.8 mg/dl, ALT of 477 U/l and AST of 437 U/l. Hematocrit was of 41.2% and hemoglobin of 13.1 g/dl. From a clinical perspective, the patient was hemodynamically stable and well oriented. Three hours later he developed tachycardia, hypotension and became oliguric. The hemoglobin level dropped to 9.8 g/dl. Hemorrhagic shock was suspected and a contrast-enhanced abdomino-pelvic computed tomography (CT) was performed. CT scan showed perihepatic, perisplenic and pelvic free fluid, a fracture of the right liver capsule and multiple heterogeneous appearing masses in the right hepatic hemiliver, the largest of which measured 87 mm in diameter (Fig. 1). The patient was resuscitated and stabilized in the Emergency Department and transferred to the third-level hepatobiliary and pancreatic surgery unit. Two consecutive transarterial embolizations of the posterior and anterior branches of the right hepatic artery were attempted and three units of packed red blood cells were transfused. The patient was subsequently hemodynamically stable.

Fig. 1 CT scan showing perihepatic free fluid, a fracture of the right liver capsule and multiple heterogeneous-appearing masses in the right hepatic hemiliver, the largest of which measured 87 mm in diameter.
Twelve hours later a cardiovascular collapse occurred. Aggressive resuscitation measures were put in place and the patient was rushed to the operating room for an emergency median laparotomy.
Three liters of blood were removed from the abdominal cavity. A deep laceration of segments VII and VIII of the liver was identified as the source of the hemorrhage (Fig. 2). The remnant right-sided hepatic parenchyma appeared ischemic, likely due to the previous embolization. Several round lesions were macroscopically visible on the surface of the liver with a typical aspect of adenomata. The gallbladder was necrotic. Intraoperative ultrasound showed good perfusion to the left hemiliver and a decision was made to proceed with a right hemihepatectomy. The surgery was uneventful and the postoperative (PO) course was characterized by a slow normalization of the liver function tests. An abdominal ultrasound performed on the 10th PO day showed initial signs of regeneration and good perfusion to the remnant liver. The patient was discharged from the ward on the 11th PO day and remained well during a recent follow-up visit.

Fig. 2 Surgical image. A deep laceration of the right hepatic hemiliver was identified as the source of the hemorrhage.
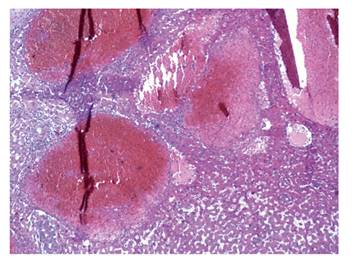
The pathology report described a necrotic adenoma of the liver and a Glisson's capsule tear adjacent to an extended area of hemorrhagic infarction. The background liver also showed diffuse signs of peliosis hepatis (Fig. 3). An out-patient CT scan on the 42nd PO day revealed compensatory hypertrophy of the remnant liver and an enlargement of sub-diaphragmatic lymph nodes, most likely of a reactive nature.
DISCUSSION
A recent review by Srinivasa et al. described spontaneous hepatic hemorrhage as most commonly caused by hepatocellular carcinoma (HCC) with 10% of HCC cases presenting with bleeding. Other causes are benign and malignant hepatic tumors of different natures, peliosis hepatis, amyloid, systemic lupus erythematosus, polyarteritis nodosa, HELLP syndrome and acute fatty liver of pregnancy 3.
The presenting signs and symptoms of liver bleeding are often subtle and non-specific; the most common are abdominal pain, malaise and vomiting. Initial workup should include an assessment of liver function, coagulation status and tumor markers. A CT scan remains the gold standard diagnostic procedure and the finding of active contrast extravasation confirms the diagnosis. Durable hemostasis is the primary aim of treatment and is usually achieved by conservative therapy or transarterial bland embolization, even though 20% of the patients will require surgical intervention. The latter includes perihepatic packing, suture plication, hepatic artery ligation or acute hepatic resection. Definitive treatment and prognosis vary depending on the underlying liver pathology 3.
The present case was a competitive bodybuilder who reported the use of a combination of clenbuterol and ephedrine, which he had purchased online. We were not able either to exclude or investigate the concomitant use of AAS, a common trend among elite athletes and body image fanatics.
Clenbuterol is a 2-agonist that is available in Europe and Latin America as a bronchodilator for human use. Studies have demonstrated that it enhances lipolysis, glycolytic capacity and minimizes protein degradation. In addition, the unique 3-adrenergic effects induce muscle hypertrophy and increased muscle strength. The effects of clenbuterol and its easy access via the internet have led to a trend of abuse among bodybuilders and fitness enthusiasts and a subsequent ban by the World Anti-Doping Agency and the International Olympic Committee. Clinical adverse events related to clenbuterol misuse are primarily cardiovascular, including myocardial injury and infarction 5.
Ephedra alkaloids are naturally occurring substances derived from the Chinese herb Ma Huang (Ephedra sinica), which is used to treat asthma, nasal congestion and fever in traditional Chinese medicine. In Western countries, these substances have been widely consumed to stimulate weight loss, increase energy levels and counteract fatigue. Due to the potent sympathomimetic effects, most adverse effects of ephedra alkaloids are cardiovascular or neurological (e.g., tremors, hypertension, myocardial infarction, seizures, stroke and psychosis) and 4% of reports have mentioned overt hepatitis 6. In April 2004, the U.S. Food and Drug Administration (FDA) banned the sale of dietary supplements containing ephedra due to the potential health risks.
Hepatotoxicity of several common herbs and dietary supplements has been widely reported, varying from asymptomatic elevation in liver enzymes levels to fulminant hepatic failure (FHF). In a retrospective case series by Estes et al., 50% of patients referred to the liver transplantation service for FHF were recent or active users of potentially hepatotoxic supplements or herbs. The four major agents with hepatotoxic potential were LipoKinetix, Kava, Chaparral and Ma Huang 7.
An Internet search of "clenbuterol and ephedrine" will result in a number of websites and forums for bodybuilders and athletes discussing the use, dosage, cycling methods, bans and possible side effects of this stimulant combination. Of interest, clenbuterol is often used together with ECA stacks, an acronym for ephedrine, caffeine and aspirin.
Peliosis hepatis (PH) was identified in the analyzed liver specimen. PH is a very rare disease which tends to remain at a sub-clinical level and is usually diagnosed incidentally during liver imaging or pathological examinations. Histologically, PH is characterized by the gross appearance of multiple cyst-like, blood-filled cavities within parenchymatous organs. At the macroscopic level in the liver, the peliotic lesions give the cut sections a "Swiss cheese" appearance and fall into the differential diagnosis with Budd-Chiari syndrome 8. Although the pathogenesis remains uncertain, Pan et al. identified three main causative categories: autoimmune, infectious and drug related 9. When these lesions rupture and cause a potentially fatal hemoperitoneum, treatment is usually surgical, including transarterial embolization, hepatic resection and liver transplant 2. The present case did not report any past medical condition that may be associated with the finding of PH, except for the chronic use of clenbuterol and ephedrine and the possible use of AAS.
CONCLUSION
The present case is the first description of a spontaneous hepatic rupture that occurred in a bodybuilder with a history of clenbuterol and ephedrine alkaloids use. This case highlights the challenge of early diagnosis of a liver complication that leads to a massive hemoperitoneum in a healthy appearing young male without a previous history of liver disease. Although the association between AAS, food supplements use and a number of pathological changes of liver structure and function is well recognized 10, drugs and food supplements used to enhance physical performance and body image are still not taken into account when evaluating risk factors for liver diseases. Due to the rarity of the condition and the high mortality rate, the patient was referred to a specialized hepatobiliary surgical unit and the treatment was guided on the basis of the available literature on similar conditions.
A variety of substances are misused by body image fanatics resulting in an enormous potential for life-threatening complications. Furthermore, inaccurate information and the online trade of drugs contribute to their widespread and illicit use.
Patients with the physique of bodybuilders and a history of substance abuse that present with an acute abdomen may have underlying liver disease. When these cases develop hemorrhagic shock, a ruptured hepatic adenoma or peliosis hepatis should be considered in the diagnosis.
