










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.110 no.5 Madrid may. 2018
https://dx.doi.org/10.17235/reed.2018.5444/2017
CASE REPORTS
Aerophagia due to abdomino-phrenic dyssynergia in a 2-year-old child
1Servicios de Gastroenterología, Hepatología y Nutrición. Hospital Sant Joan de Déu. Barcelona, Spain
2Servicios de Fisioterapia. Hospital Sant Joan de Déu. Barcelona, Spain
CASE REPORT
A 2-year-old child presented to the Emergency Room (ER) due to progressive, abdominal distension that worsened during the night of a one week duration. The patient also presented isolated vomiting, normal stools and irritability in the absence of fever.
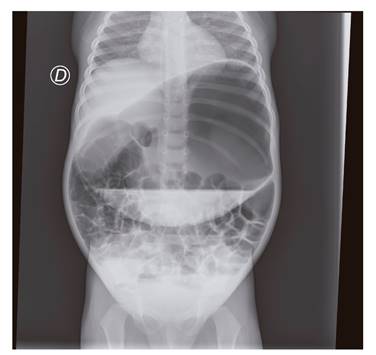
An abdominal x-ray film identified abundant intra-abdominal air (Fig. 1) with no other abnormal findings. The patient was examined by the Surgery Department and acute abdomen was ruled out. Following a spontaneous clinical improvement, the patient was discharged from hospital. Fifteen days later, the patient returned due to persistent abdominal distension that worsened throughout the day, in association with intermittent vomiting and greenish, foul-smelling stools over the previous ten days. The stool culture was negative and the patient was admitted for assessment.
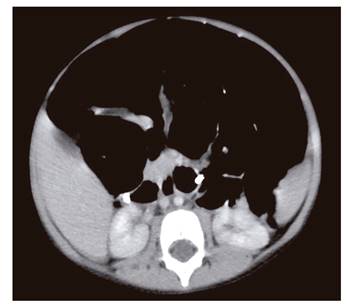
A new radiographic imaging test on admission revealed significant gastric distension. Laboratory tests that included cell count, liver and kidney function were normal and the anti-transglutaminase antibodies were negative. The child was again assessed by the Surgery Department and gastric volvulus was suspected. A nasogastric tube (NGT) was placed and a liquid diet was maintained. The intestinal transit was normal. A transpyloric tube was placed and feeding was started with a basic formula. This was well tolerated although obvious distension persisted. Accordingly, an open NGT was left in place with intermittent aspiration. However, abdominal distension remained progressive throughout the day. An abdominal computed tomography (CT) scan found no evidence of a malrotation (Fig. 2) but a significant generalized distension from the stomach to the large bowel was identified. A total of 2.5 liters of gas per 24 hours were recovered from the NGT.
The patient remained symptomatic and a macronutrient intolerance was excluded. An endoscopic examination found no abnormal changes that could account for the symptoms and clinical presentation. The diet was changed to a milk-based polymeric formula but there was no clinical change. Blenderized food was initiated with an adequate tolerance and no clinical worsening. Therefore, the transpyloric tube was removed. An open NGT was kept in place without aspiration and an oral diet of an adequate texture was introduced. An empiric therapeutic test was performed using metronidazole for suspected bacterial overgrowth 1 and erythromycin for gastrointestinal tract motility 2, which resulted in no clinical improvement.
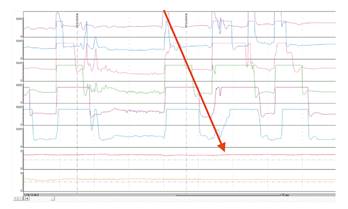
After ruling out a malrotation, bowel obstruction and cows' milk protein intolerance, aerophagia was suspected, as the patient repeatedly swallowed small amounts of air in an almost imperceptible manner. A pH-impedancemetry was performed and the results were consistent with daytime aerophagia (Fig. 3) within the pathological range of five air swallows (> 15,000 Ohm) per minute. Based on the description of abdomino-phrenic dyssynergia in adults 3, treatment was started with respiratory physical therapy (manual abdominal exercises) in order to induce intra-abdominal pressure changes to enhance peristalsis and modify breathing patterns. Simeticone was also added and the symptoms gradually improved, with a good tolerance of an age-appropriate normal diet.
Pathologic aerophagia is an uncommon pediatric disorder that almost exclusively affects children with an underlying neurologic condition. It may lead to multiple diagnostic tests and unnecessary aggressive therapies 2. A recent case report associated aerophagia with a novel concept of abdomino-phrenic dyssynergia 4.
BIBLIOGRAFÍA
1. Sieczkowska A, Landowski P, Kaminska B, et al. Small bowel bacterial overgrowth in children. J Pediatr Gastroenterol Nutr 2016;62:196-207. DOI: 10.1097/MPG.0000000000000920 [ Links ]
2. Rashid ANS, Taminiau JA, Benninga MA, et al. Definitions and outcome measures in pediatric functional upper gastrointestinal tract disorders: a systematic review. J Pediatr Gastroenterol Nutr 2016;62:581-7. [ Links ]
3. Villoria A, Azpiroz F, Burri E, et al. Abdomino-phrenic dyssynergia in patients with abdominal bloating and distension. Am J Gastroenterol 2011;106:815-9. [ Links ]
4. Dike CR, Bishop W, Pitcher G. Aerophagia and abdomino-phrenic dyssynergia in a 3-year-old. J Pediatr Gastroenterol Nutr 2017;65:e76-7. [ Links ]
Received: January 10, 2017; Accepted: February 07, 2018
