










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Upper gastrointestinal bleeding (UGIB) in infants and children is a common problem and accounts for 20% of referrals to pediatric gastroenterologists 1. Non variceal UGIB in children is more rare than in adult patients and can be caused by gastritis, peptic ulcers, angiodysplasic lesions, Dieulafoy lesions, congenital or acquired coagulopathies, polyps, pancreatitis with pseudocyst and hemorrhage or aortoenteric fistula. Even though the number of UGIB cases is significantly lower in children compared to adult patients, this is a potentially life-threatening emergency that is a common cause of hospitalization. Peptic ulcer disease in children is reported worldwide, although it is relatively rare in adults 2.
Helicobacter pylori infection is a common cause of ulcers in pediatric patients. Other risk factors include the use of non-steroidal anti-inflammatory agents, steroids, immunosuppressive drugs and stressful events 3. Interventional endoscopy has replaced surgery as the primary technique for bleeding peptic ulcers. However, the rate of rebleeding is still high after endoscopic hemostasis 4,5.
High dose proton pump inhibitors (PPI) infusion and second look endoscopy are strategies to prevent peptic ulcer rebleeding after endotherapy that have been tested in adult patients 6. Second look endoscopy performed within 24 hours after therapeutic endoscopy appears to reduce the risk of rebleeding in the absence of high dose PPI infusion in adult patients, although study designs and results vary 7,8. Meanwhile, prospective randomized studies in adult patients have demonstrated that high-dose omeprazole infusion after endoscopic hemostasis stabilizes the clot over the bleeding artery and successfully prevents peptic ulcer rebleeding 9,10. Studies in adult patients are used as primary guides for the evaluation of pediatric practice. There are no randomized studies with regard to the efficacy of pharmacologic therapy with high dose PPIs infusion compared to second look endoscopy for the prevention of peptic ulcer rebleeding in children. Esomeprazole is currently the only PPI drug approved for use in young children in Romania.
The aim of this prospective randomized trial was to compare the two strategies of scheduled second look endoscopy plus bolus esomeprazole with an additional high dose continuous esomeprazole infusion for the prevention of peptic ulcer rebleeding after endoscopic hemostasis in children. The main outcome was to assess the rebleeding rate within 30 days after initial hemostasis.
MATERIAL AND METHODS
A prospective randomized study was performed over a period of four years and eight months, between January 2012 and August 2016. The study was conducted at an Emergency Hospital for Children that is a reference center for all cases from surrounding counties. This hospital has highly specialized staff working in Pediatric Gastroenterology and Hepatology, Pediatric Surgery and Pediatric Digestive Endoscopy with appropriately trained pediatric endoscopists. All legal guardians/parents of patients enrolled in the study signed an informed consent prior to inclusion. Institutional ethical approval was obtained for this study. The work was conducted in compliance with the Local Institutional Review Board for Human Subjects Research Committee requirements.
All children who presented with acute UGIB underwent endoscopy within 24 hours after admission. The study included patients aged between two and 18 years who had undergone successful endoscopic hemostasis for bleeding peptic ulcers. Children with bleeding peptic ulcers with endoscopic stigmata of active bleeding, nonbleeding visible vessels or adherent clots were recruited (type Ia, Ib, IIa and IIb lesions according to the Forrest Classification System) 11. Children were excluded if the bleeding could not be controlled during the first endoscopy, there was no informed consent, cases with a known allergy to PPI or bleeding from non-ulcer lesions, subjects with an American Society of Anesthesiologists (ASA) grade 5 or 6, as well as those weighing less than 10 kilograms (kg). The children enrolled in this study heavier than 10 kg fit the criteria for therapeutic endoscopy with a 9.2 millimeter (mm) outer diameter videogastroscope with a 2.8 mm working channel that allows the performance of endoscopic hemostasis according to recent pediatric published guidelines 12. An Olympus(r) Exera II CV180 Gastrointestinal Videoscope System (Olympus Co. Ltd., Tokyo, Japan) was used using a GIF-Q165 videogastroscope with an outer diameter of 9.2 mm and working channel of 2.8 mm. The first endoscopic intervention was standardized for every child enrolled with a bleeding peptic ulcer, as an initial injection of 1:10000 epinephrine around the ulcer to achieve a tamponade effect, followed by the application of hemoclips (EZ clips, Olympus Co. Ltd, Tokyo, Japan). The same method of endotherapy was used during the second look endoscopy if bleeding stigmata persisted.
Pediatric endoscopists obtained written informed consent from the legal guardians and also from the children aged more than eight years of age with appropriate neuro-cognitive development, after successful initial endoscopic hemostasis for bleeding ulcers. The children were consecutively randomized to undergo either a scheduled second look endoscopy with appropriate therapy in the case of bleeding stigmata within 12-24 hours of the initial endoscopy (first group), or to receive a high dose continuous esomeprazole infusion after a successful primary endoscopic hemostasis (the second group). The children were randomized by a hospital based intranet computer system. Children assigned to the first group received an intravenous bolus of 0.5 mg/kg (maximum 40 mg) esomeprazole every 12 hours after the initial endoscopy for 72 hours. The omeprazole infusion dose is well established for adult patients: 80 mg intravenous bolus followed by 8 mg/hour continuous infusion for 72 hours (6). With regard to the second group, the pediatric dose for esomeprazole infusion was derived from existing indications for adults as follows: 1 mg/kg intravenous bolus followed by 0.1 mg/kg/hour continuous infusion for 72 hours. With regard to children who weighed at least 40 kg and were older than 12 years of age, the standard adult dose was applied. Both groups of patients received oral esomeprazole at 1 mg/kg daily, once per day (maximum 40 mg), after the 72 hour period of intravenous esomeprazole for the following 30 days. Children were closely monitored by hourly measurement of blood pressure, pulse, respiratory rate and diuresis for the first 72 hours. This was followed by close observation of the symptoms of rebleeding such as signs of hypovolemia (raised heart rate over 20 beats per minute [bpm] above the age-appropriate median), hematemesis, melena or a drop in hemoglobin of more than 2 g/dl. The clinical course and outcome of all children enrolled in this study were recorded from admission and after discharge from hospital, until 30 days from the first endoscopy. After discharge, the children were followed up by clinical and biological monitoring visits twice a week as outpatients, for a period of 30 days.
The statistical analysis was performed using the SPSS17 software. Means and standard deviations were calculated for numerical variables with a normal distribution, whereas medians and ranges were calculated for variables with a non-normal distribution. Qualitative variables were expressed as numbers and percentages. The Chi-squared test (with Yates' correction for continuity) was used to compare proportions expressed as percentages. The Kaplan-Meier curve was used to represent the probability of recurrent bleeding within 30 days of the initial hemorrhage and the two groups were compared using the log rank test. A p-value < 0.05 was considered as significant for each statistical test.
RESULTS
Two hundred and thirty-eight children were admitted with acute UGIB to the Emergency Children Hospital where the study was conducted from January 2012 to August 2016. A total of 144 children were diagnosed with bleeding gastric or duodenal ulcers and 127 were successfully treated with primary endoscopic therapy (88.1%). Seventeen children underwent emergency surgery following a failed primary endoscopic hemostasis. After endoscopic hemostasis, 63 children were randomized to undergo a second look endoscopy within 12-24 hours after initial endoscopy (the first group), and 64 were randomized to receive a high dose continuous esomeprazole infusion for 72 hours without endoscopic reassessment, unless in the case of an emergency rebleeding (the second group). Figure 1 shows a schematic diagram of the recruitment of subjects in the study.

There was no statistically significant difference between the two groups in terms of baseline demographic data including age, gender and ASA grade. There was also no statistically significant difference in the proportion of children who were admitted due to shock, the use of nonsteroidal anti-inflammatory drugs (NSAID) or oral steroids, hemoglobin level upon admission and the prevalence of Helicobacter pylori infection. None of the children recruited were receiving antiplatelet/anticoagulant therapy. In relation to ulcer characteristics, there was no significant difference between the groups with regard to the distribution of gastric or duodenal ulcers. The mean ulcer size was 1 cm in the PPI infusion group and 0.8 cm in the scheduled second look endoscopy group. In addition, there was no statistical difference in the distribution of endoscopic stigmata of recent ulcer bleeding according to a Forrest classification between the two groups. Table 1 shows the demographic data of the children and ulcer characteristics of the two study groups.
Table 1 Demographic data of the cohort and ulcer characteristics of the two study groups
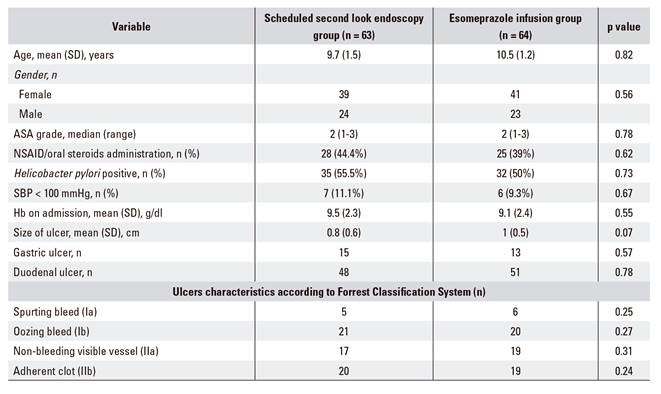
ASA: American Society of Anesthesiologists; Hb: hemoglobin; NSAID: nonsteriodal anti-inflamatory drug; SBP: systolic blood pressure.
None of the children in the second look endoscopy group developed rebleeding before the second scheduled endoscopy. During the second look endoscopy, the majority of children had non-significant ulcer stigmata that did not require endoscopic retreatment. Only six children (9.5%) had persistent stigmata of a visible vessel (Forrest IIa classification) or adherent clots (Forrest IIb classification). All these patients underwent endoscopic retreatment. Table 2 shows the changes in the Forrest classification of ulcer stigmata during the second look endoscopy compared to the initial endoscopy.
Table 2 Changes in the Forrest classification of ulcer stigmata during the second look endoscopy compared to the initial endoscopy

Rebleeding occurred in four children (6.3%) in the first group after the second look endoscopy despite endoscopic retreatment, and in three children (4.6%) in the esomeprazole infusion group. With regard to children with rebleeding, two patients in the second look endoscopy group and one patient in the esomeprazole infusion group required surgical hemostasis. Table 3 shows the stratification of the cumulative rebleeding rates from the first day until after one month of surveillance among the two treatment groups. There was no significant difference between the two groups with regard to the probability of rebleeding within 30 days after endoscopic treatment (log rank test p = 0.7). Figure 2 shows the Kaplan Meier comparison of the probability of peptic ulcer rebleeding within the two groups.


DISCUSSION
Scheduled second look endoscopy examined the bleeding ulcer 12-24 hours after the initial hemostasis, with the intention to re-treat a persistent stigmata of a recent hemorrhage and prevent rebleeding 13,14. High dose PPI infusion decreases the need for a second look endoscopy and significantly reduces the risk of rebleeding in patients with peptic ulcers. There are a lot of studies in adult population that support this 7,9,15, but pediatric studies are scarce. After therapeutic endoscopy, persistent hemostasis would be accomplished via the formation of clots over the bleeding arteriole. In vitro studies have shown that an acidic environment can induce a significant platelet disaggregation and would result in rebleeding of peptic ulcers via the dissolution of the clots over the bleeding vessel 16. An increase in intra-gastric pH would lead to a cessation of pepsin activity and allow persistent platelet aggregation. The effectiveness of high dose PPI infusion in preventing rebleeding was further confirmed in a large scale, multicenter, prospective, randomized study 17. An international consensus recommended the use of adjunctive high dose PPI infusion in adults after therapeutic endoscopy and stated that second look endoscopy should not be routine practice 18. However, no prospective, randomized studies in pediatric population have compared these two strategies for the prevention of ulcer rebleeding.
The current randomized trial is the first pediatric study that compared scheduled second look endoscopy and PPI bolus administration with a strategy of high dose continuous PPI infusion without endoscopic reassessment in order to evaluate the prevention of ulcer rebleeding. The PPI used in this research was esomeprazole. Esomeprazole is a proton-pump inhibitor used in children for the treatment of dyspepsia, peptic ulcer disease, gastroesophageal reflux, Zollinger-Ellison syndrome and Helicobacter pylori eradication together with antibiotics. This compound decreases the secretion of acid via the inhibition of the H+/K+-ATPase in the parietal cells of the stomach. By inhibiting the functioning of this transporter, the drug increases the intragastric pH. Esomeprazole is the (S)-enantiomer of omeprazole. The usual pediatric dose of esomeprazole varies between 0.5 and 1 mg/kg/day, and the standard adult dose should be used from 12 years of age or 40 kg in weight. Doses over 1 mg/kg/day in children have not been studied 19. Single 20 to 40 mg oral doses that are recommended for adults generally give rise to peak plasma esomeprazole concentrations of 0.5-1.0 mg/l within 1-4 hours. However, these levels may increase by about 50% after several days of once-daily administration. A 30-minute intravenous infusion of a similar dose usually produces peak plasma levels in the order of 1-3 mg/l 20.
In this pediatric study, high dose continuous esomeprazole infusion had a similar efficacy to second look endoscopy for the prevention of ulcer rebleeding. An esomeprazole infusion strategy reduced discomfort in children and avoided the huge workload generated by a second endoscopy.
The limitations of the study include the fact that the patient sample size in this study was smaller compared to other adult studies on the same topic. This is due to the fact that the number of upper gastrointestinal bleeding cases is significantly lower in children compared to adult patients. Further studies in larger samples of pediatric patients are necessary.
CONCLUSIONS
A pharmaceutical approach by a high dose continuous esomeprazole infusion in children after an initial endoscopic hemostasis has a similar efficacy compared to second look endoscopy and bolus PPI administration for the prevention peptic ulcer rebleeding. Thus, the discomfort of a second endoscopy in children can be avoided and is only recommended for selected high risk cases.
