










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Cirugía Oral y Maxilofacial
On-line version ISSN 2173-9161Print version ISSN 1130-0558
Rev Esp Cirug Oral y Maxilofac vol.29 n.3 Madrid May./Jun. 2007
PÁGINA DEL RESIDENTE
What should the diagnosis and treatment be?
¿Cuál sería su diagnóstico y su manejo terapéutico?
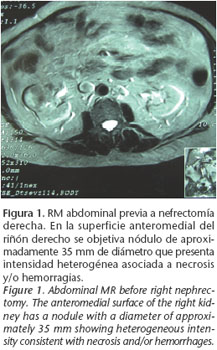
Male patient, 81 years of age, with a personal history of hypothyroidism, benign prostatic hypertrophy, glaucoma and right nephrectomy for renal clear cell carcinoma in June 2004 (Fig. 1). He currently has bilateral lung metastasis that is being followed by the Oncology Department which, to date, has not considered starting chemotherapy appropriate.
He had attended the Oral and Maxillofacial Surgery Department on an outpatient basis as a result of a tumor-like mass on the side of his tongue that had been developing for various weeks. His physical examination revealed an excrescent polylobulated and friable mass on the right posterolateral border of the tongue that measured 2x1 cm (Fig. 2). The remaining examination was normal, and clinically positive cervical adenopathy was not noted. Given these findings a biopsy sample was taken.

The pathology study indicated ulcerated clear cell carcinoma and, given the clinical antecedents of the patient, it was diagnosed as metastasis from renal carcinoma.
It was decided that local extirpation of the lesion should be the therapeutic strategy, as the general health of the patient was good and he was experiencing discomfort in the area. The lesion was excised using local anesthesia and direct closure was carried out
The surgical specimen obtained was described macroscopically as an irregular polylobulated formation with a maximum diameter of 1.9 x 1.1 cm that was brownish in color, and which had black areas on being cut. The definitive histopathologic study confirmed ulcerated metastasis of clear cell kidney carcinoma (Fig. 3).

The patient has to date made favorable progress.
Lingual metastasis from renal carcinoma
Metástasis lingual de carcinoma renal
R. del Rosario Regalado1, S. Gallana Álvarez2, T. Creo Martínez1, J. Herce López1, S. Pereira Gallardo3
1 Médico Residente.
2 Médico Adjunto. Servicio de Cirugía Oral y Maxilofacial.
3 Médico Residente. Servicio de Anatomía Patológica.
Hospital Universitario Virgen Macarena, Sevilla, España.
Discussion
Metastatic tumors to the oral cavity, especially to the tongue, are extremely rare. Only 1% of all intraoral malignant neoplasms are metastatic and, of these, only 5% appear on the tongue.1
Zegarelli et al.2 described a rate of 0.2% of all malignant lingual lesions. Primary tumors that later metastasize to the oral cavity appear to arise in the lungs, kidneys, skin and brain. This tends to happen with a greater frequency in patients that are over the age of 60, and only in 20% of cases do they arise before the primary tumor is discovered.3
Renal carcinoma represents the third infra-clavicular neoplasm in order of metastatic frequency in the head and neck region, occurring in 15% of cases.4
Generally, when renal carcinoma metastasis develops in the tongue, it tends to appear as an exophytic, pedicled, ulcerated mass with a tendency to bleed. These characteristics necessitate a differential diagnosis that includes pyogenic granuloma in response to a local irritant, and primary neoplasms of the oral cavity, even though these may have a glandular or epithelial origin. In any event, the pathologic study of the specimen will provide the definitive diagnosis.
In this case of ours, imaging tests were not needed for the extension study of the lesion, but had these been needed, a computed axial tomography is the modality of choice, as it allows discerning the extension and vascularization of the lesion. The preoperative angiography and secondary embolization reduce the risk of bleeding during the biopsy or resection, and it may be indicated in some cases.5 The therapeutic strategy that should be followed depends on the location of the tumor and on the metastasis, as well as the general health of the patient. In general, surgical excision is considered the first treatment option, for the primary tumor as well as for metastases in the head and neck. In this way the patient is offered a better quality of life and a possible cure. Traditionally renal carcinoma has been considered radio-resistant, but some studies have shown that this is effective for treating metastatic disease.6
Chemotherapy can be used as adjuvant treatment in cases of postsurgical recurrence. For treating metastatic disease, interleukin-2 is used or interferon alpha. The percentage of partial response is around 5-20%, and the percentage of patients with complete response is less than 5%.7
The prognosis for renal carcinoma with metastasis is poor. ODea et al. reported a survival rate at two years of 78% when metastasis to the oral cavity is identified, and a survival at 5 years of 50% when metastasis develops after a nephrectomy.8
References
1. Friedlander AH, Singer R. Renal adenocarcinoma of the kidney with metastasis to the tongue. J Am Dent Assoc 1978;97:989-91.
2. Zegarelli DJ, Tsukada Y, Pickren JW, Greene GW JR. Metastatic tumor to the tongue: Report of 12 cases. Oral Surg Oral Med Oral Pathol 1973;35:2002-11.
3. Meyer I, Shklar G. Malignant tumors metastatic to mouth and jaws. Oral Surg Oral Med Oral Pathol 1965;20:350-62.
4. Cheng ET, Greene D, Koch RJ. Metastatic renal cell carcinoma to the nose. Otolaryngol Head Neck Surg 2000;122:464.
5. Pritchyk KM, Schiff BA, Newkirk KA, Krowiak E, Deeb ZE. Metastatic renal cell carcinoma to the head and neck. Laryngoscope 2002;112:1598-602.
6. Simo R, Sykes AJ, Hargreaves SP, Axon PR, Birzgalis AR, Slevin NJ, Farrington WT. Metastatic renal cell carcinoma to the nose and paranasal sinuses. Head Neck 2000;22:722-7.
7. Reese DM, Corry M, Small EJ. Infusional floxuridine-based therapy for patients with metastatic renal cell carcinoma. Cancer 2000;88:1310-6.
8. ODea MJ, Zincke H, Utz DC, Bernatz PE. The treatment of renal cell carcinoma with solitary metastasis. J Urol 1978;120:540-2.
![]() Correspondence:
Correspondence:
Ruth del Rosario Regalado
Email: draruthdelrosario@gmail.com
1. Friedlander AH, Singer R. Renal adenocarcinoma of the kidney with metastasis to the tongue. J Am Dent Assoc 1978;97:989-91. [ Links ]
2. Zegarelli DJ, Tsukada Y, Pickren JW, Greene GW JR. Metastatic tumor to the tongue: Report of 12 cases. Oral Surg Oral Med Oral Pathol 1973;35:2002-11. [ Links ]
3. Meyer I, Shklar G. Malignant tumors metastatic to mouth and jaws. Oral Surg Oral Med Oral Pathol 1965;20:350-62. [ Links ]
4. Cheng ET, Greene D, Koch RJ. Metastatic renal cell carcinoma to the nose. Otolaryngol Head Neck Surg 2000;122:464. [ Links ]
5. Pritchyk KM, Schiff BA, Newkirk KA, Krowiak E, Deeb ZE. Metastatic renal cell carcinoma to the head and neck. Laryngoscope 2002;112:1598-602. [ Links ]
6. Simo R, Sykes AJ, Hargreaves SP, Axon PR, Birzgalis AR, Slevin NJ, Farrington WT. Metastatic renal cell carcinoma to the nose and paranasal sinuses. Head Neck 2000;22:722-7. [ Links ]
7. Reese DM, Corry M, Small EJ. Infusional floxuridine-based therapy for patients with metastatic renal cell carcinoma. Cancer 2000;88:1310-6. [ Links ]
8. ODea MJ, Zincke H, Utz DC, Bernatz PE. The treatment of renal cell carcinoma with solitary metastasis. J Urol 1978;120:540-2. [ Links ]

