










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Cirugía Oral y Maxilofacial
On-line version ISSN 2173-9161Print version ISSN 1130-0558
Rev Esp Cirug Oral y Maxilofac vol.38 n.1 Madrid Jan./Mar. 2016
https://dx.doi.org/10.1016/j.maxilo.2014.03.004
ORIGINAL ARTICLE
Surgical indications of orbital fractures depending on the size of the fault area determined by computed tomography: A systematic review
Indicaciones quirúrgicas de las fracturas orbitarias atendiendo al tamaño del defecto de fractura determinado por tomografía computarizada: Una revisión sistemática
Blas Garcia Garcia and Alicia Dean Ferrer
Departamento de Cirugía Oral y Maxilofacial, Hospital Universitario Reina Sofía, Córdoba, Spain
ABSTRACT
Introduction: Surgical treatment of the orbital fractures is used in an attempt to prevent or treat complications, such as the enophthalmos, double vision, or limitations in ocular movements. The aim of this study is to carry out a systematic review of the literature in order to quantify the fault area in orbital walls. It also aims to increase the volume of the orbital cavity in the orbital traumatism that determines the appearance of ocular symptomatology and that, in turn, may require surgical reconstruction.
Material and methods: An electronic search was conducted in Medline (Pub-Med) using the terms: "orbital", "volume", "fracture", "enophthalmos" and "computer". Only these studies that relied on CT measurements, only included fractures of floor and medial wall of the orbit, and fulfilled the criteria for high methodological quality, were selected.
Results: Various studies determine that fractures with areas greater than 1.102.00 cm2, as well as an increase in orbital volume, will lead to the appearance of enophthalmos in 1015% of the cases. In addition, for every 1 cm3 increase in the volume of the orbital cavity, the enophthalmos increases between 0.47 mm and 0.90 mm.
Conclusions: According to the published results, surgical orbital reconstruction is indicated for faults greater than 2 cm2, with a volume greater than 1.62 cm3, an orbital volume greater than 1015% of the orbital cavity, or when the fracture is located in the innermost region, between the floor and medial wall of the orbit in the so called "key area".
Key words: Orbital. Fracture. Volume. Enophthalmos. Computed tomography.
RESUMEN
Introducción: El tratamiento quirúrgico de las fracturas orbitarias pretende prevenir o tratar complicaciones tales como el enoftalmos, la diplopía o la limitación de los movimientos oculares. El objetivo de este estudio es realizar una revisión sistemática de la literatura para cuantificar el área del defecto de paredes orbitarias y el incremento de volumen de la cavidad orbitaria en traumatismos orbitarios que va a determinar la aparición de sintomatología ocular y que, por tanto, indica la reconstrucción quirúrgica.
Material y métodos: Se ha realizado una búsqueda electrónica en Medline (PubMed) utilizando los términos: "orbital", "volume", "fracture", "enophthalmos" y "computer". Se seleccionaron aquellos estudios que realizaban mediciones sobre TC, que incluían exclusivamente fracturas de suelo y pared medial de la órbita y que cumplían los criterios de alta calidad metodológica.
Resultados: Los distintos estudios determinan que fracturas con áreas de defectos superiores a 1,10-2,00 cm2 así como incrementos de volumen orbitario superiores al 10-15% conducirán a la aparición de enoftalmos. Además, por cada cm3 de incremento de volumen de la cavidad orbitaria, se produce un aumento del enoftalmos entre 0,47 y 0,90 mm.
Conclusiones: Según los resultados publicados, estaría indicada la reconstrucción quirúrgica orbitaria ante un defecto superior a 2 cm2, ante un incremento de volumen superior a 1,62 cm3, ante incrementos de volumen orbitario superiores al 10-15% de la cavidad orbitaria o cuando la fractura se localiza en la región más posterior, entre el suelo y la pared medial de la órbita en la llamada "área clave".
Palabras clave: Órbita. Fractura. Volumen. Enoftalmos. Tomografía computarizada.
Introduction
The purpose of the surgical treatment of orbital fractures is to restore the anatomy by reconstructing the orbital walls and reducing herniated soft tissues. Surgical reconstruction is indicated in order to prevent sequelae or to treat the complications derived from fractures of this type, such as such entrapment of the extraocular musculature, diplopia, limited ocular motility or enophthalmos.1
With respect to enophthalmos, the critical cut-off that classically indicates surgical orbital reconstruction is determined by the very definition of enophthalmos: a difference in the ocular position between the 2 eyes greater than or equal to 2 mm, measured on the anteroposterior axis by Hertel exophthalmometry.2,3
The explanation for why it is necessary to know the size of the orbital fracture defect that indicates surgical reconstruction lies in the fact that early surgical treatment of orbital fractures could reduce the complications outlined above, provided it is performed within the first 2 weeks after the injury.4,5 Moreover, the edema and emphysema produced in orbital fractures can mask a latent enophthalmos that can become evident toward the 2nd or 3rd week, when the edema and emphysema disappear.2 On the other hand, a number of studies published in recent years have shown that an increase in orbital volume, without taking into account the changes produced in the soft tissues (which are less determinant in the development of enophthalmos), correlates linearly with the development and severity of posttraumatic enophthalmos.6-12
The objective of this study is to carry out a systematic review of the literature to quantify, using measurements obtained from computed tomography (CT) images, the area of the defect in the orbital walls and the increase in volume of the orbital cavity in orbital trauma. As orbital fracture will result in the development of ocular symptoms, it is an indication for surgical reconstruction of the orbital walls. The quantification of these 2 data by CT could serve as a guideline and indication for this reconstruction.
Material and methods
All the searches were performed electronically according to the bases proposed in the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement,13 on 10 February 2014, using the Medline (PubMed), Cochrane Plus, Scielo and Education Resources Information Center (ERIC) databases and search engines. The inclusion and exclusion criteria were established a priori. The search involved the use of the medical terms: "orbital", "volume", "fracture", enophthalmos" and "computer".
With these key words, we found 27 articles, but selected only those that met the following inclusion criteria: (1) measurements made from CT images; (2) fractures that involved only one orbit; (3) orbital floor or medial wall fractures; (4) the determination of the volume or area; and (5) definition of the degree of enophthalmos according to the orbital defect. We also excluded those studies in which the site of the fracture was not specified and those that included lateral orbital wall or orbital roof fractures. Articles in which there was duplicity of cases were also excluded. In addition, we analyzed the bibliography cited in the selected studies to evaluate certain aspects that could be relevant.
A critical reading of the material was carried out in accordance with the critical reading program, Critical Appraisal Skills Programme: Spanish (CASPe),14 to determine the validity of the results, taking into account the following criteria: size and representativeness of the sample; mean patient age; duration of follow-up; and discussion of the biases and limitations of the study in the article. Only those articles for which positive responses could be given to a minimum of 8 out of 10 questions posed by the CASPe program were selected. These articles were classified as being of high methodological quality.
Of all the articles, five9,17-20 were considered to be of high methodological quality. In addition to these reports, we included all the articles cited in them that focused on the quantitative determination of the fracture defect size that would lead to the development of symptoms, and also met the abovementioned inclusion criteria, but had not been included in the original search with the aforementioned key words because of their titles. Thus, 4 more studies were added,11,15,16,21 for a total of 9 articles reviewed. Data were collected on all the important variables, including publication year, first author, country of origin and language, number of cases, type of measurement performed, patient ages, image acquisition system and the surface or volume measurements obtained (Table 1).
Table 1 - Image acquisition system and measurements obtained for surface area or volume.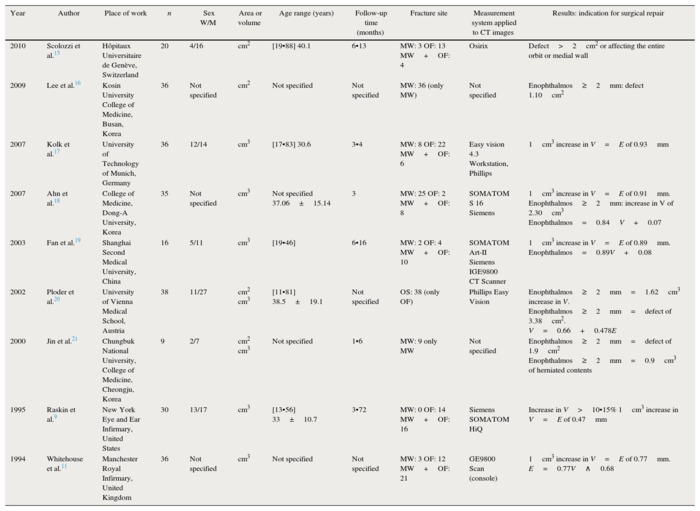
E, enophthalmos; M, men; MW, medial wall; n, sample size; OF, orbital floor; V, orbital volume in cm3; W, women.
Results
Study selection
We identified 9 articles9,11,15-21 that met all the above-mentioned inclusion criteria; they involved a total of 256 patients with unilateral orbital floor or medial wall fracture. All of the patients were studied by CT to determine the area of the fracture or the increase in orbital volume following traumatism. As very few articles discussed the possible biases and limitations, this parameter did not enable the discrimination of the quality of the studies. Thus, it was not considered a posteriori as a study quality criterion.
Description of the Studies Included
Nine studies published between 1994 and 2010, summarized in Table 1, described the relationship between the size of the orbital fracture defect and the development of posttraumatic enophthalmos. They involved a total of 9 separate groups of surgeons. The sample size in the different studies ranged between 9 and 38 cases, and the patients were enrolled consecutively in every case.
All of the authors used the contralateral orbit as a reference for comparing the measurements obtained. The follow-up period differed in each article, ranging between 3 and 72 months.
Study population
The age range across all the reports was from 11 to 88 years. Only 2 studies included patients under 18 years of age. In all, 68% of the individuals enrolled were men.
Fracture sites
All of the studies included only those orbital fractures that involved orbital floor or medial wall or a combination of both; thus, fractures of the orbital roof or lateral wall were excluded. Of the total of 256 fractures studied, 86 (33.6%) affected the medial wall alone, 105 (41%) were isolated orbital floor fractures and 65 (25.4%) involved both sites.
Degree of enophthalmos
The studies that determined the area of the orbital wall fracture defect reported measurements ranging between 1.10 and 3.38 cm2, which correlated with enophthalmos of 2 mm. With respect to the measurements of the posttraumatic volume, the finding was that, for every cm3 of increase in volume, enophthalmos ranging between 0.47 and 0.93 mm, depending on the study in question, was produced. Kolk et al.17 even define a portion of the orbital walls, the so-called "key area", located in the posterior part of the orbital cavity, between the orbital floor and medial wall, the involvement of which is associated with a higher incidence of sequelae (Fig. 1).
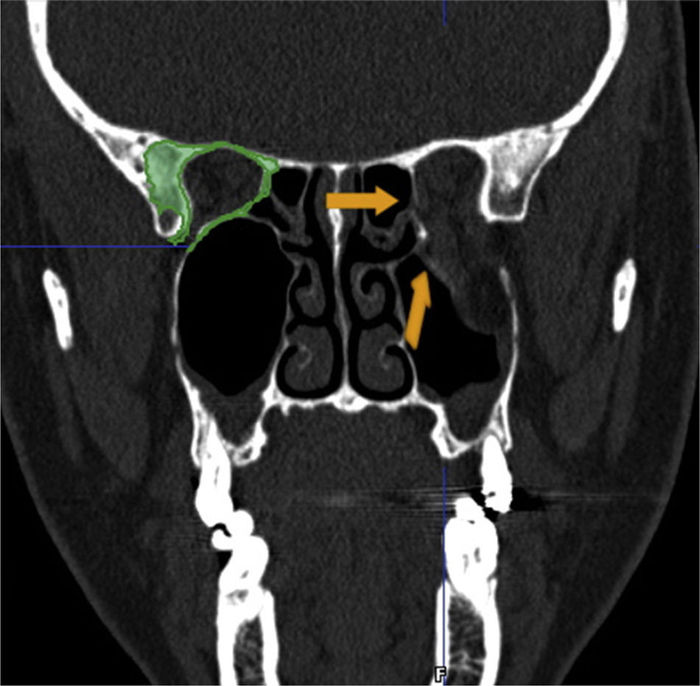
Fig. 1 - "Key area", corresponding to the zone of transition between
the posteromedial portion of the orbital floor and the medial wall.
The close correlation between the change in orbital volume resulting from fracture and the degree of enophthalmos was demonstrated by Anh et al., Fan et al., Ploder et al. and Whitehouse et al. using Pearson correlation. The analysis of the linear correlation of enophthalmos with the change in orbital volume resulted in the following mathematical formulas:
- Anh et al.18: E = 0.84V + 0.07. P < 0.001, SEE = 0.58 mm, r = 0.86, n = 35
- Fan et al.19: E = 0.89V + 0.08. P < 0.001, r = 0.95, n = 16
- Whitehouse et al.11: E = 0.77V ∧ 0.68. P < 0.001, SEE = 0.63 mm, r = 0.87, n = 11
- Ploder et al.20: V = 0.66 + 0.478E. P = 0.002, r = 0.64, n = 38
E: enophthalmos; SEE: standard error of the estimate; V: volume change in cm3.
Description of the systems for measuring the area of the fracture and change in volume
The measuring systems used by the authors varied depending on the publication year, with Osirix, which was utilized by Scolozzi et al.,15 being the most advanced software of those employed in the different studies included in this review.
Discussion
Enophthalmos ≥2 mm has classically been considered to require surgical reconstruction of the orbital walls to restore orbital function and correct the cosmetic sequelae associated with enophthalmos. Burm et al.22 and Lee et al.16 report late enophthalmos in 75% of the patients with untreated medial orbital wall fracture, an incidence that indicates the importance of an adequate evaluation of patients with orbital trauma of this type.
The causes of enophthalmos are considered to be: (a) prolapse of the orbital soft tissue contents into the maxillary sinus; (b) orbital fat atrophy; (c) loss of support by the orbital bones; and (d) increased orbital volume.23 At the present time, the major cause of enophthalmos following surgery for orbital reconstruction is considered to be the nonanatomic or inadequate correction of the defect, especially when the increase in volume has been produced by a fracture in the most posterior portion of the orbital floor or in the zone of transition between the posteromedial portion of the orbital floor and the medial wall, in the so-called "key area",17 in which small defects have a more severe impact on volume, compared to that produced at other sites.
On the other hand, the most important limitation common to all the studies published to date, including those referred to here, lies in the use of the intact orbit of the patients to determine the increase in volume produced in the contralateral orbit by the fracture. Under normal conditions, in the absence of orbital trauma, the volumes of left and right orbits can differ by up to 78%.7,23 Thus, this method of measuring the change in volume was the greatest limitation in all the articles.
Dolynchuk et al.24 demonstrated that enophthalmos can result from increases in orbital volume starting at 5% to 10%.16 This calculation takes into account the estimated normal variability (78%). One thing that does appear to be clear is that, given the high probability of the development of enophthalmos, surgery would be indicated when the volume had increased by more than 1015%.9
We should also point out the wide variability in the results obtained from the measurements, spanning ranges that are very far from one another, with the greatest differences being observed among those authors who determined the area of the fracture defect. Ploder et al.20 are the most conservative in this respect, reporting that a fracture area of 3.38 cm2 leads to 2 mm of enophthalmos, and Lee et al.,16 the least, indicating orbital wall reconstruction with defects of only 1.10 cm2. In contrast, the results in terms of the volume increase that the different degrees of enophthalmos will produce are more homogeneous, from which we can deduce that these values are more accurate for the determination of the degree of posttraumatic enophthalmos than the calculations based on the measurement of the area of the defect. This disparity in the findings can be explained by the variability in the means of CT image acquisition and the measuring methods employed by each group of authors. Moreover, the great advances made in these systems over the last 2 decades should be taken into account. During this time, the degree of accuracy in the measurements has increased markedly with the modern equipment for image acquisition and the development of new measurement software, that enable an increasingly thorough and precise study of the defects resulting from orbital fractures. Thus, it is logical to think that the most recent studies are based on more accurate measurements and, consequently, the data are more reliable.
With respect to the mathematical formulas obtained from the analysis of the linear correlation of enophthalmos and the orbital volume after fracture, they are useful tools for establishing a treatment protocol that enables the early determination of the degree of posttraumatic enophthalmos that, if surgery is delayed, could result in sequelae that are difficult to treat once established. However, the variability in the mathematical constants of each of the formulas described still make the results obtained from these equations unreliable, with the added difficulty that comes with having to have the adequate means and skill to measure the volume of the orbital cavity before enophthalmos develops.
Conclusions
The volumetric data provided by the studies included in this review are highly heterogeneous and, therefore, should be interpreted with caution. We consider that the values found in the most recent studies are more reliable because the measurement methods and image acquisition systems are more accurate than those of past decades.
There is no large-scale anthropometric study of the orbit that serves as a reference and permits the estimate of volumes without having to use the contralateral orbit.
Studies with large sample sizes are necessary to enable the establishment of accurate mathematical equations for the early prediction of the development enophthalmos ≥2 mm that will require surgical repair of the orbital walls.
To date, and according to published results, surgical reconstruction of the orbit should be indicated when the wall defect is greater than 2 cm2, when the orbital volume increases by more than 1.62 cm3, and when the orbital volume is increased by more than 10-15%.
Ethical disclosures
Protection of human and animal subjects. The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent. The authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interest
The authors declare they have no conflicts of interest.
![]() Correspondence:
Correspondence:
Blas Garcia Garcia
blasgg6@hotmail.com
Received 5 December 2013
Accepted 16 March 2014
References
1. Mucci B. A new perspective on blow-out fracture of the orbit. Injury. 1997;28:555-6. [ Links ]
2. Osguthorpe J.D. Orbital wall fractures: Evaluation and management. Otolaryngol Head Neck Surg. 1991;105:702-7. [ Links ]
3. Dulley B., Fells P. Long-term follow up of orbital blowout fracture with or without surgery. Mod Probl Ophthalmol. 1975;19:467-70. [ Links ]
4. Hawes M.J., Dortzbach R.K. Surgery on orbital floor fractures. Influence of time of repair and fracture size. Ophthalmology. 1983;90. [ Links ]
5. Kirkegaard J., Greisen O., Højslet P.E. Orbital floor fractures: Early repair and results. Clin Otolaryngol Allied Sci. 1986;11:69-73. [ Links ]
6. Bite U., Jackson I.T., Forbes G.S., Gehring D.G. Orbital volume measurements in enophthalmos using three-dimensional CT imaging. Plast Reconstr Surg. 1985;75:502-8. [ Links ]
7. Forbes G., Gehring D.G., Gorman C.A., Brennan M.D., Jackson I.T. Volume measurements of normal orbit structures by CT analysis. AJR Am J Roentgenol. 1985;145:149-54. [ Links ]
8. McGurk M., Whitehouse R.W., Taylor P.M., Swinson B. Orbital volume measured by a low-dose CT scanning technique. Dentomaxillofac Radiol. 1992;21:70-2. [ Links ]
9. Raskin E.M., Millman A.L., Lubkin V., della Rocca R.C., Lisman R.D., Maher E.A. Prediction of late enophthalmos by volumetric analysis of orbital fractures. Ophthal Plast Reconstr Surg. 1998;14:19-26. [ Links ]
10. Ramieri G., Spada M.C., Bianchi S.D., Berrone S. Dimensions and volumes of the orbit and orbital fat in posttraumatic enophthalmos. Dentomaxillofac Radiol. 2000;29:302-11. [ Links ]
11. Whitehouse R.W., Batterbury M., Jackson A., Noble J.L. Prediction of enophthalmos by computed tomography after 'blow out' orbital fracture. Br J Ophthalmol. 1994;78:618-20. [ Links ]
12. Charteris D.G., Chan C.H., Whitehouse R.W., Noble J.L. Orbital volume measurement in the management of pure blowout fractures of the orbital floor. Br J Ophthalmol. 1993;77:100-2. [ Links ]
13. Moher D., Liberati A., Tetzlaff J., Altman D.G., PRISMA GroupPreferred Reporting Items for Systematic Reviews and Meta-analyses: The PRISMA statement. Ann Intern Med. 2009;151:264-9. [ Links ]
14. Cabello JB, por CASPe. Plantilla para ayudarte a entender una revisión sistemática. En: CASPe. Guías CASPe de lectura crítica de la literatura médica, 1. Alicante: CASPe; 2005. p. 13–7. [ Links ]
15. Scolozzi P., Momjian A., Heuberger J. Computer-aided volumetric comparison of reconstructed orbits for blow-out fractures with nonpreformed versus 3-dimensionally preformed titanium mesh plates: A preliminary study. J Comput Assist Tomogr. 2010;34:98-104. [ Links ]
16. Lee W.T., Kim H.K., Chung S.M. Relationship between small-size medial orbital wall fracture and late enophthalmos. J Craniofac Surg. 2009;20:75-80. [ Links ]
17. Kolk A., Pautke C., Schott V., Ventrella E., Wiener E., Ploder O., et al. Secondary post-traumatic enophthalmos: High-resolution magnetic resonance imaging compared with multislice computed tomography in postoperative orbital volume measurement. J Oral Maxillofac Surg. 2007;65:1926-34. [ Links ]
18. Ahn H.B., Ryu W.Y., Yoo K.W., Park W.C., Rho S.H., Lee J.H., et al. Prediction of enophthalmos by computer-based volume measurement of orbital fractures in a Korean population. Ophthal Plast Reconstr Surg. 2008;24:36-9. [ Links ]
19. Fan X., Li J., Zhu J., Li H., Zhang D. Computer-assisted orbital volume measurement in the surgical correction of late enophthalmos caused by blowout fractures. Ophthal Plast Reconstr Surg. 2003;19:207-11. [ Links ]
20. Ploder O., Klug C., Voracek M., Burggasser G., Czerny C. Evaluation of computer-based area and volume measurement from coronal computed tomography scans in isolated blowout fractures of the orbital floor. J Oral Maxillofac Surg. 2002;60:1267-72. [ Links ]
21. Jin H.R., Shin S.O., Choo M.J., Choi Y.S. Relationship between the extent of fracture and the degree of enophthalmos in isolated blowout fractures of the medial orbital wall. J Oral Maxillofac Surg. 2000;58:617-20. [ Links ]
22. Burm J.S., Chung C.H., Oh S.J. Pure orbital blowout fracgure: New concepts and importance of medial blowout fracture. Plast Reconstr Surg. 1999;103:1839-49. [ Links ]
23. Parsons G.S., Mathog R.H. Orbital wall and volume relationships. Arch Otolaryngol Head Neck Surg. 1988;114:743-7. [ Links ]
24. Dolynchuk K.N., Tadjalli H.E., Manson P.N. Orbital volumetric analysis: Clinical application in orbitozygomatic complex injuries. J Craniomaxillofac Trauma. 1996;2. [ Links ]

