










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkINTRODUCTION
The reconstruction of the midface represents a major challenge in the field of head and neck reconstruction. This is particularly true when soft tissue and skin defects are associated with bone defect. Specifically, the maxilla supports almost the entire midface, and is essential for adequate functioning of the masticatory system, having an extremely variable shape1. Similarly, skin and soft tissue are extremely important for the aesthetics of the facial region. They are different in each patient and their color and volume are difficult to reproduce.
Several techniques have been proposed for the reconstruction of midface defects. Prosthetic obturators, local or regional flaps, and free flaps are useful for restoring facial structure, support orbital content, and separate oral and nasal cavities. However, free flaps represent the most suitable solution for the treatment of extensive defects of this region2. In fact, local or regional flaps might be insufficient when the reconstruction of the bone needs to be associated with the reconstruction of the soft tissue and the skin. In this regard, fibula, iliac crest and scapula rim flap were successfully used for this purpose3,4,5,6,7,8. Nevertheless, the shape of the bone obtained from these flaps is substantially different with respect to the maxilla3,4. Hence, the functional and aesthetic outcomes might be not good enough in the case of a large defect. Recently, the scapular angle osteomyogenous free flap has been increasingly used to overcome these inconveniences5.
The main aim of the present work was to describe the versatility and utility of the scapular angle osteomyogenous flap for the reconstruction of extensive defects of the midface.
MATERIALS AND METHODS
The medical records of four patients that had undergone maxillary reconstruction by using a microvascular scapular tip flap in our department were retrospectively reviewed to identify possible advantages and disadvantages of this type of flap. Failure or partial failure, aesthetic outcomes, and early and late complications were analyzed. All reconstructions were performed between November 2017 and June 2018. Brown's classification was used to define the maxillary defects.
Harvest technique
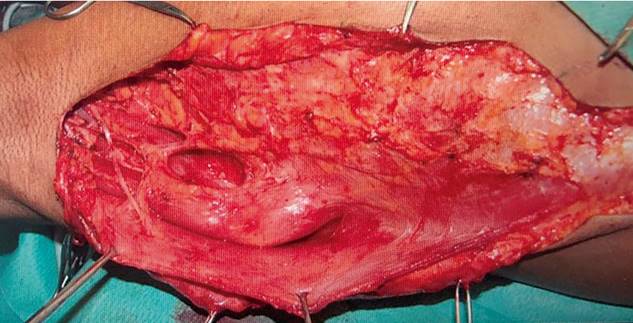
The torso of the patient is rotated approximately 45° and the pelvis 30°. This approach usually allows two teams to work simultaneously. When skin paddle is not required, an incision is performed from the mid axillary line to the inferior portion of the anterior border of latissimus dorsi. The first step is to expose the dorsal edge of the muscle latissimus dorsi. The dissection of the pedicle is anteromedial to latissimus. The next step is to define the vascular anatomy (Figure 1). The pedicle may be variable. The angular branch usually originates from the thoracodorsal artery (more frequently), from the branch to serratus, or from a trifurcation with these vessels (Figure 2). Importantly, the pedicle needs to be completely mobilized before performing the bone cuts in order to avoid injury to the vessels. Kocher forceps may be used to grasp the scapular bone and pull it out. This significantly increases visibility during the osteotomy and facilitates bone cutting. Although up to 14 cm of bone may be obtained with this flap, 6 cm should be sufficient for maxillary reconstruction. The dissection of the pedicle continues until the circumflex scapular vessels are clearly visible. The serratus anterior, subscapularis, and teres major are reinserted to the remnant bone with absorbable suture. The use of a large suction drain is recommended. Shoulder function usually completely recovers within 6 months post surgery9,10,11,12.

Report of cases
Patient 1. A 53-year old woman underwent several surgeries and 2 cycles of radiotherapy for a cystic adenoid carcinoma of the left maxilla. Thus, as a consequence of this catastrophic development the patient presented limited mouth opening (< 2 cm), large volume defect of the left midface, bone support defect (Type 3 Brown's classification), ocular dystopia and epiphora. Interestingly, she did not present diplopia. The quality of life of the patient 7 years after surgery was extremely poor and she demanded a new reconstruction. After a careful evaluation of the case we decided to remove the latissimus flap used in the previous reconstruction, the skin graft of the temporal region, and the extensive intraoral scar. The defect was reconstructed with a chimeric scapular tip osteocutaneous free flap (Figure 3). The microvascular anastomosis was performed with the facial vessels on the left side. The scapular bone was positioned vertically and fixed with two miniplates. A small portion of the serratus muscle was used to repair the intraoral defect with the aim of improving the mouth opening, while the latissimus with the skin palette was used to fill the soft tissue defect on the left midface. The final result was satisfactory. We observed a considerable improvement in the mouth opening (2,7 cm), a clear improvement in the orbital contour and an adequate filling of the midface. At the donor site, a seroma was observed in the initial days following surgery. This complication was treated with local compression. No other surgically related complications were observed during the eleven months post surgery.

Patient 2. This was a 56 year-old male who had undergone hemimaxillectomy (left side) (Type 2 Brown´s classification) and primary reconstruction with pedicled temporalis flap 7 years previously. An obturator and one zygomatic implant (left side) were used 2 years after the primary surgery to complete dental rehabilitation. However, the progressive atrophy of the temporalis muscle caused a significant retraction of the upper lip and an obvious collapse of the left midface (Figure 4). In addition, a chronic peri-implantitis occasioned frequent episodes of superinfection with fistulization at the level of the skin of the sub-palpebral region. As a result of this chronic infection, he also showed a considerable retraction of the sub-palpebral skin with ectropion and epiphora. Consequently, the patient reported an extremely poor quality of life and demanded a new reconstruction. In this case, a scapular tip flap was also used for the reconstruction. The microvascular anastomosis was performed on the left side with the facial vessels. The scapular bone was positioned vertically and fixed with two miniplates. A small amount of serratus muscle was used to add intraoral volume and to avoid communication with the mouth. No skin paddle was used in this case. The final result was extremely satisfactory (Figure 5). In particular, we observed a significant aesthetic and functional improvement. Moreover, no other episodes of superinfection were observed during follow-up. No complications at the donor site were observed three months after surgery.

Figure 4. Preoperative frontal view of patient 2. The figure shows aesthetic and functional sequelae of previous surgeries.

Figure 5. Patient 2 after reconstruction with osteomyogenous tip scapular flap. Clinical appearance 1 month after surgery.
Patient 3. This patient was a 59-year old man referred to our center with a positive biopsy for squamous cell carcinoma of the hard palate. The tumor involved almost all of the maxillary bone. Thus, the patient underwent total maxillectomy (Type 1c Brown's classification), bilateral neck dissection, and primary reconstruction with an osteomyogenous scapular tip flap. The microvascular anastomosis was performed with the facial vessels on the right side. The scapular bone was positioned horizontally to reconstruct the palatal defect and separate the mouth from the nasal cavity. Aesthetic and functional outcomes were acceptable and no major complications of the donor site were documented seven months after surgery.
Patient 4. A 69-year-old male affected by a squamous cell carcinoma of the left maxillary sinus involving left maxilla and orbital floor. After careful evaluation, the patient underwent hemimaxillectomy (Type 3 Brown's classification), left neck dissection, and primary reconstruction with a scapular tip flap. The scapular bone was positioned vertically to support the left midface and fixed with two miniplates (Figure 6). A titanium mesh was used to reconstruct the continuity of the orbital floor. The microvascular anastomosis was performed with the facial vessels on the right side. No complications at the donor site were observed nine months after surgery.

RESULTS
There was no flap necrosis or infection. All flaps showed a complete epithelization between 25 and 79 days. All anastomoses were performed with the facial vessels and there was no need to use arterial or vein graft. In 2 of the 4 cases, 2 teams worked simultaneously. No major complications were observed at the donor site during follow-up. With respect to functional outcomes, speech was considered normal in 3 patients and intelligible in 1. Similarly, mouth opening was classified as normal in 2 patients, mildly restricted in one patient, and moderately restricted in one patient. Feeding capacity was defined as normal in 2 patients and restricted in the other two. In relation to aesthetic outcomes, these were considered to be good in 3 patients and fair in the other one.
DISCUSSION
The scapular angle osteomyogenous flap represents a new and interesting alternative for the reconstruction of extensive defects of the midface. It was first described by Deraemaeker in 1988 and since then it has been increasingly used11. In fact, it ensures a number of advantages with respect to other composite flaps2,9. For instance, its pedicle can reach up to 20 cm, which is particularly important in maxillary reconstruction where there is a need to avoid vein or artery graft. In contrast, fibula and iliac crest have relatively short pedicles and this could create several problems in maxillary reconstruction. No arterial or vein grafts were used in our series. This allows for reducing the technical difficulties of the surgery and the risks related to arterial and vein graft. In addition, the scapular angle presents a similar structure to the native maxilla. Specifically, a robust cortical bone predominates in the lateral area, while the bone is spongier and more malleable at the medial edge. The shape of the scapular angle allows for a good reconstruction of maxillary defects, and osseointegrated implants are possible with this flap2,11. The flap may be oriented both vertically and horizontally, which allows for an efficient reconstruction of several types of maxillary defects. The entire hemi-maxilla -including the orbital floor and the palate- might be completely reconstructed if the flap is positioned vertically. Moreover, the flap can reproduce the entire palato-aveolar complex when it is oriented horizontally13. Another important advantage of this flap is its reliability. The vessels of the scapular vascular system are extremely resistant to atherosclerosis and can be used safely even in patients with pathologies of the peripheral vascular system. Moreover, several composite options are possible and muscle (teres major, latissimus dorsi, serratus anterior), skin and bone may be combined according to the type of defect. In this regard, this flap offers a more considerable mass of tissue when compared with fibular or iliac crest flap and it might be extremely useful in cases of extensive soft tissue loss. Moreover, each part of the flap receives an independent pedicle with mobile tissue components. This notably facilitates the flap set in2,9,11.
Other advantages of this reconstructive resource include easy remodeling and fixation. In fact, the bone can be ''greenstick''-fractured to guarantee a proper set-in and adequate projection. In contrast to fibula, no further osteotomies need to be performed for the proper set in13. The fixation of the bone may be accomplished with the use of miniplates or wire. In addition, the minimal donor site morbidity related to the harvesting of this flap and the rapid mobilization of the patients in the early postoperative period suggest that this flap might be particularly useful in elderly patients2,9.
In our opinion, scapular angle osteomyogenous flap may be extremely useful in the reconstruction of extensive defect of the midface and could therefore be regarded as an essential part of the armamentarium of each head and neck reconstruction service. Although the data related to the use of this flap are still relatively scarce, it has proven to be safe and reliable. Moreover, the resistance of the scapular vascular system to atherosclerosis represents a major advantage and makes this flap a useful alternative in patients with contraindications to free fibula flaps. This study presents some limitations. For instance, this is a retrospective study and the sample is small.

