










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Tumours located in the pterygopalatine and infratemporal fossae remain a challenge to surgeons due to its difficult access and complex anatomy. Surgery in these regions is changing thanks to the advances in endoscopic techniques. Despite, accessibility to deep-seated lesions in these regions remains difficult.
Traditionally, extensive anterior (transfacial or transmandibular) and lateral/posterolateral (transcranial) approaches have been used to access the pterygopalatine fossa and infratemporal regions1. These approaches offer good exposure; however, they have higher morbidity and complications such as unacceptable scarring and facial numbness may occur.
Over the last decades, there has been a gradual interest in endoscopic techniques applied to the craniofacial region. The endoscopic-assisted surgery to these regions is efficient and safe and offers lower morbidity. The progressively evolving experience has widened indications and greater exposure can be provided with the multi-angled and magnified views. However, many authors have questioned the accessibility of these techniques and its reliability, especially in oncological patients.
To access these areas in one single operation, several authors have recommended the combination of and endoscopic endonasal and sublabial transmaxilary approach1, joining advantages of both methods in cases of lesions located in the pterygopalatine and infratemporal fossa.
CASE REPORT
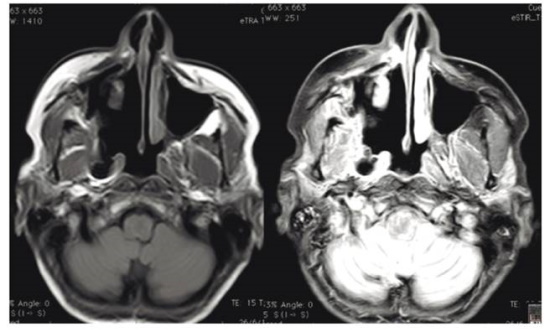
We report the case of a 47-year-old woman who presented with a right retropterygoid mass suggestive of a malignant tumor. MRI showed a retropterygoid mass located between the right medial pterygoid muscle and the lateral nasopharynx wall, measuring 15 x 10 x 17 mm (Figure 1).

Intraoperative navigation assisted-surgery was performed with preoperative 3D surgical planning (Figure 2). A right medial endoscopic maxillectomy was performed by the ENT team, followed by partial resection of the middle turbinate, ethmoidectomy and sphenoidectomy. Then a large maxillary antrostomy is performed to gain access to the posterior region of the sinus. The posterior wall was removed and the mass was localized and confirmed using intraoperative navigation assistance (Figure 3). The infraorbital nerve was visualized, and intraoperative biopsies were sent to discard tumoral infiltration.


Then, an open approach was performed through a vestibular incision in the right gingivobuccal sulcus. The periosteum was elevated, and the anterior maxillary sinus wall exposed. Then, an anterior maxillary wall resection is performed. Through the posterior wall of the maxillary sinus the tumor was reached. The lateral part of the right pterygoid plate and the tumor were removed and sent for anatomopathological exam. The anterior maxillary wall was repositioned and osteosynthesis with a titanium mesh and plates was performed. The mucosa was closed with absorbable sutures and nasal packing on the right side was performed with a merocele with antibiotic ointment. No intraoperative complications occurred.
The nasal packing was removed, and the patient was discharged from hospital 3 days after surgery. She complained of postoperative facial numbness (V2) that recovered in less than 6 months.
Definitive anatomopathological analysis showed a low-grade salivary gland carcinoma (hyalinizing clear cell type) with close surgical margins. The pterygoid plate was found free of disease. The patient received postoperative radiotherapy (Figure 4) shows a coronal plane of the 3 month post-operative MRI, showing complete resection and no radiological persistence of the tumor.
Discussion
The management of lesions in the pterygopalatine and infratemporal fossa remains challenging. These regions host a complex neurovascular anatomy. A profound knowledge of the anatomy of these areas is required when performing surgery safely.
In the pre-endoscopic era, the surgical approaches to the pterypgopalatine and infratemporal fossa included transmaxillary, maxillary swing and facial translocation procedures2. All of these carry risk of significant morbidity, including infraorbital neurovascular bundle injury, chronic maxillary sinusitis, oroantral fistula, facial numbness, epiphora, etc.3.
Endoscopic surgery is performed for lesions that extend beyond the paranasal cavities to the infratemporal and pterygopalatine fossa, being indicated not only in cases of inflammatory disease but also for both benign and malignant tumor resections where anatomy is complex and difficult to access4. A modified medial maxillectomy is a standard procedure to access the infratemporal and pterygopalatine regions endoscopically. Morbidity is significantly lower compared to open approaches and complications are reduced. Cosmetics and scarring is also more favorable. Nevertheless, it is not exempt of complications, which include dental and ipsilateral palate numbness and lack of emotional tearing2. Alar retraction can occur with this approach but is less prominent than when done open5.
The endonasal route approach allows minimally invasive through the anteromedial surface to access these areas6. Advances in endoscopic endonasal surgery, such as interventional radiology, with preoperative embolization, improved instrumentation, computer-based navigation and hemostatic materials have enabled endoscopic endonasal access to tumors of the pterygoapaltine and infratemporal fossa7. The endoscopic approach to these areas is feasible, safe and efficient with a low frequency of complications.
However, several authors have reported several disadvantages of endoscopic surgery such as worse hemostatic control. Its reliability in terms of oncological resection has also been questioned, given the reduced surgical field and more complex manipulation, and difficulties with the access to more lateral lesions have been experienced with this approach. When addressing malignant tumors far lateral in the infratemporal fossa, additional procedure beyond antrostomies are usually required2. This is especially important when an oncological resection is performed, since complete resection can be hampered due to difficulties in visualization and handling. Ensuring comfortable maneuverability and easy visualization of the region maximizes the chances of complete resection and surveillance2.
However, several studies have demonstrated similar exposure for endoscopic and open approaches. For instance, Xue et al.8) compared both anterior transmaxillary and endoscopic transnasal approaches on their exposure area and found no difference. Angled instruments and proper training and handling of the endoscope are recommended to maximize maneuverability and optimize results.
The combined transmaxillary and endonasal approach was first popularized by Al- Mefty9 et al. Theodospoulos et al.10) stated that the combined approach allows dissection within the whole pterygopalatine fossa and infratemporal fossa, providing adequate control of vascular structures.
This combined approach has the advantage of an anatomically favorable trajectory through the maxillary sinus1. Surgery is less invasive compared to classical open approaches and morbidity and scarring are diminished. The transmaxillary open approach allows greater exposure and surgical field in comparison to pure endoscopic approaches, specially to achieve hemostasis or when an oncological resection is performed, where maneuverability and visibility are essential. Exposure of the pterygopalatine and infratemporal fossa is greater, particularly in lesions located laterally where endoscopic reachability is more difficult. Also, compared to pure endoscopic approaches, it is less complex and technically demanding, since control of hemostasis and manipulation can be assisted through the anterior antrostomy, making surgery easier and safe. We consider that a thorough preoperative evaluation of imaging exams and intraoperative navigation as wells as a surgeon who is trained in the endoscopic approach to these areas are mandatory for successful results.
In conclusion, this combined approach offers advantages of both open and endoscopic approaches and shall be considered when access to the pterygopalatine and infratemporal fossa is required, especially in oncological patients where a pure endoscopic approach might be technically demanding. Large clinical series and further studies are needed to compare this combined approach to classical approaches.

