










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Epidemiological studies have identified mental disorders as leading risk factors for all types of suicidal behavior (Hawton et al., 2013; Inder et al., 2014). Suicidality is most commonly linked to depression, and depressiveness in other mental disorders also increases the risk for suicidal behavior (Chesney et al., 2014; Isometsä, 2014; McGirr & Turecki, 2008). Furthermore, subjective feelings of depressiveness is often accompanied by suicidal ideation in non-clinical population (Tang et al., 2018).
Suicidality and Affective Temperaments
Recently, studies have been more focused on investigating the connection between temperament, personality dimensions, and suicidality. Prior studies on the topic of temperament and suicidality have mostly been based on the theoretical framework of affective temperaments by Akiskal and the use of Temperament Evaluation of Memphis, Pisa, Paris, and San Diego Auto-questionnaire (TEMPS-A) (Akiskal et al., 2005). Results have shown that the dominant expression of any affective temperament may be considered to be a risk factor for suicide attempts, except for hyperthymic temperament, which is usually a protective factor (Baldessarini et al., 2017; Baldessarini et al., 2016; Pompili et al., 2012). Anxious, depressive, and irritable affective temperaments were found to be significant risk factors for suicidal behavior in clinical population (Karam et al., 2015). Moreover, when comparing suicidal and non-suicidal patients, affective temperament seemed to be a better predictor of suicide risk than other risk factors (Baldessarini et al., 2017). A similar recent study conducted by Pompili et al. (2018) found elevated scores of all affective temperaments in the group of suicidal patients and in patients with a diagnosis of major depressive disorder (the highest scores were in anxious temperament, the lowest in hyperthymic temperament). These authors suggested a composite score model (anx + cyc + dep + irr – hyp) that predicts suicidal behavior the best. A composite score model with a somewhat different order of affective temperaments (dep + cyc + irr + anx – hyp) was suggested by Baldesarini et al. (2017). Other studies have also suggested similar models for predicting suicide attempts (Ardani et al., 2017; Tondo et al., 2018). A multicentric study that included nearly 3,000 patients suffering from depression, found significantly more hypomanic characteristics (risky behavior, psychomotor agitation, impulsivity) in the group of patients with depression who had a history of suicide attempts compared to the group with no history of suicide attempts (Popovic et al., 2015).
Estimates for the predictive value of temperament for suicidal behaviors has shown to be significant even in non-clinical population. The study that showed a link between temperament and suicidal ideation in healthy population suggests the importance of screening for suicide risk as part of suicide prevention (Skala et al., 2012). This is vital when we take into consideration data obtained through psychological autopsies in individuals who have committed suicide, which warn us that a great number of them suffered from some mental disorder that most frequently had not been diagnosed in their lifetime (Arsenault-Lapierre et al., 2003; Cavanagh et. al., 2003).
Suicidality and Personality Traits
Besides temperament, personality dimensions also contribute to suicidal behavior, particularly aggressiveness (Baca-Garcia et al., 2005; Goldney et al., 1997; Isometsä, 2014; Popovic et al., 2015), impulsivity (Baca-Garcia et al., 2005; Blüml et al., 2013; Brezo et al., 2006; Isometsä, 2014; Peters et al., 2016; Popovic et al., 2015; Rozanov & Mid’ko, 2011), and neuroticism (Blüml et al., 2013; Brezo et al., 2006; Popovic et al., 2015).
A review exploring personality dimensions and suicidality (Brezo et al., 2006) pointed toward high neuroticism as a significant contributor to suicidal ideation, suicide attempts, and suicides, and extroversion as a protective factor. Furthermore, neuroticism is prominent both in patients suffering from depression (Blüml et al., 2013; Petersen et al., 2001), as well as in those with a history of suicide attempts (Kumar et al., 2013; Rozanov & Mid’ko, 2011).
The presence of a mood disorder by itself has shown only limited predictive value when it comes to predicting suicide attempts, thus making research of other personality characteristics and risk factors imperative (Vázquez et al., 2018). Studies have indeed shown that personality plays an important mediating role between mental disorders and suicidal behaviors; however, they most commonly involved separate assessment of personality (character) traits and temperament traits. In this paper we aimed at taking as comprehensive and complex view of personality as possible, considering it from the aspect of temperament and character in conjuction, and assessing the manner in which these constructs are mutually interrelated on the one hand, and how each one of them contributes to attempted suicide in depressive patients, on the other.
Therefore, the primary aim of this study was to determine whether affective temperaments and personality (character) traits can predict suicide attempts in population of patients with depression.
Method
Procedure
This study was an observational cross-sectional study conducted during 2018, including patients diagnosed with major depressive disorder according to ICD-10 (World Health Organization, 2004). The study was conducted after obtaining approval from ethics committees in three different hospitals, out of which two were university clinics.
Inclusion criteria were to be over 18 years old, outpatients or inpatients diagnosed with a recurrent depressive disorder (F33) or major depressive disorder, single episode (F32) according to ICD-10. Exclusion criteria were psychiatric comorbidity according to ICD-10 (primarily bipolar disorder, psychotic disorder, addictive disorder, etc.), intensive care treatment at the time of testing, severe somatic comorbidity, severe cognitive dysfunction, and mental retardation.
Participation in the study was voluntary. Every subject was explained the purpose of the study, and interviews were conducted after an informed consent had been signed by each subject. The interviews were conducted by a psychologist with adequate clinical and research experience.
Sample
Two hundred and fifty-one patients were divided into two groups, one without previous suicide attempts (66.9%, 168 subjects) and the other with previous suicide attempts (33.1%, 83 subjects). The final sample consisted of 109 (43.4%) male and 142 (56.6%) female patients with no significant difference between groups in gender, χ2(1) = 0.000, p > .05, or age, t(249) = 1.014, p > .05. Mean age of participants was 49.13 ± 13.09 (range 18-81). Average illness duration was 7.17 ± 8.48 years, with 56.2% inpatients and 43.8% outpatients. Other demographic variables are given in Table 1.
Table 1. Additional Demographic Data for the Sample

Note. S = suicidal group; N = nonsuicidal group.
More patients with previous suicide attempts (25.3% compared to 17.3% in the group with no previous suicide attempts) had a family history of mental disorders, but this difference was not statistically significant, χ2(1) = 1.775, p > .001. However, family history of suicide attempts was significantly different between groups, χ2(1) = 11.320, p < .001, with more patients with previous suicide attempts (30.1% compared to 11.9%) having a family history of suicide attempts. There were no significant differences in the prevalence of chronic somatic diseases between the groups, χ2(1) = 2.611, p > .05, nor in length of time since first diagnosis, t(249) = 1.879, p > .05.
Instruments
Sociodemographic questionnaire. Constructed for this study, this questionnaire was used to obtain data on gender, age, education, work experience, marriage status, number of children. Information about patients’ current health and chronic somatic diseases, illness duration, and family history were obtained through patients’ medical history. Information on suicide attempts was confirmed after close inspection into official documents and patients’ medical history.
Temperament Evaluation of Memphis, Pisa, Paris, and San DiegoAutoquestionnaire (TEMPS-A). This instrument was used for the assessment of affective temperaments with good internal consistency and construct validity (α = .83), as well as satisfactory alpha coefficient for subscales (.73-.80) (Akiskal et al., 2005). The Serbian version comprised 41 true/false items grouped into six temperament traits (Ristić-Ignjatović et al., 2014): depressive (7 items describing sensitivity to suffering, tendency to complain about social role and social norms), cyclothymic (7 items describing rapid mood and energy swings), hyperthymic (7 items describing cheerful, optimistic, and energetic behaviour), irritable (8 items describing dysphoric, choleric, gloomy behaviour), anxious-cognitive (6 items describing worry-prone behaviour), and anxious-somatic (6 items describing somatic symptoms of anxiety). Every temperament type score is calculated by dividing the number of all the items that patients marked as “true” by the total number of items on specific temperament scale, thereby obtaining a score ranging from 0 to 1, with the higher score indicating greater prevalence of the given temperament type. External validation of the scale showed high correlation with the TCI-R temperament scale in Serbian population, while an average test-retest coefficient (rho = .82) implying stable validity over time (Ristić-Ignjatović et al., 2014).
Big Five Plus 2 Personality Questionnaire, short version (VP+2-70) (Čolović et al., 2014) is a self-reported questionnaire based on the theoretical framework of Big Five model which evaluates seven personality dimensions: neuroticism (anxiety, depression, negative affect), extroversion (cordiality, positive affect, sociability), conscientiousness (persistence, self-discipline, thoughtfulness), aggressiveness (anger, stubbornness, hardheadedness), openness (intellect, novelty seeking), negative valence (manipulativeness, negative self-image) and positive valence (feeling of superiority, positive self-image). The 70 items are answered through a Likert scale ranging from 1 (completely disagree) to 5 (completely agree). Results have so far shown adequate reliability (α ranging from .75 to .86), high correlation with the original scale (r ranging from .90 to .95), and good convergent and predictive value of the questionnaire.
Statistical Analyses
Normality was assessed using the Kolmogorov-Smirnoff test, t-test for independent samples, MANOVA and chi-square test were employed for evaluating statistical difference between the groups. Correlation was determined using the Pearson’s correlation coefficient, while the influence of independent variables on dependent variables was tested through multivariate logistic regression. The program used for these analyses was SPSS 21.0.
Results
Affective Temperaments
Affective temperament scale (TEMPS-A) has shown adequate internal consistency coefficients, ranging from α = .79 for irritable to α = .85 for cyclothymic temperament, with an average coefficient for the entire scale of α = .89. Scores for various temperament types in both groups of subjects are shown in Table 2
Table 2. Descriptive Statistics for TEMPS-A Scores

Note. Mean range from 0 to 1; Z = Kolmogorov-Smirnov test.
*p < .05, **p < .01.
In all temperaments and both groups, distributions of scores were deviating toward higher values, except for the hyperthymic temperament in the group of patients with previous suicide attempts, where they deviated toward lower values, and irritable temperament, where both group scores deviated toward lower values (Table 2).
TEMPS-A scores differed significantly between both groups of subjects: cyclothymic, t(249) = -3.612, p < .001, η2 = .05; hyperthymic, t(249) = 3.038, p = .003, η2 = .04); anxious-cognitive, t(249) = -2.654, p = .008, η2 = .03; and anxious-somatic, t(249) = -2.989, p = .003, η2 = .03, but the size effect was large only in depressive, t(249) = -5.628, p < .000, η2 = .11, and medium in irritable temperament, t(249) = -4.136, p < .000, η2 = .06. In all temperaments other than hyperthymic higher scores were predominantly in the group of patients with previous suicide attempts.
Differences between genders in the group of patients without previous suicide attempts were found only in anxious temperament where females scored higher. anxious-cognitive, t(166) = -2.794, p = .006, η2 = .04; anxious-somatic, t(166) = -2.160, p = .032, η2 = .03. Similar differences were found between genders in the group of suicidal patients: anxious-cognitive, t(81) = -2,181, p = .032, η2 = .03; anxious-somatic, t(81) = -2.451, p = .016, η2 = .07.
Personality Dimensions (VP+2)
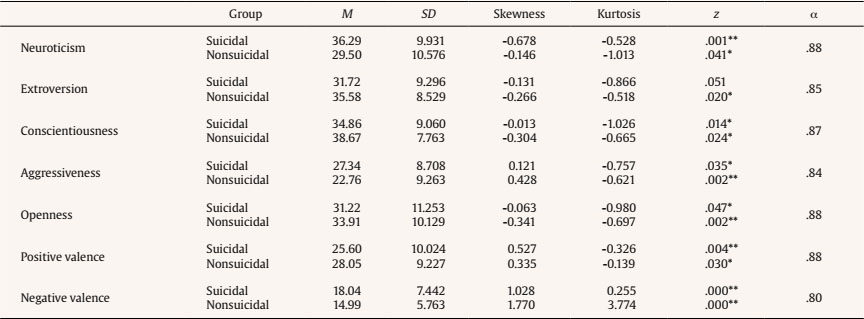
Internal consistency coefficient was high for the VP+2 scale (α = .90), with satisfactory subscale coefficients, ranging from α = .80 to α = .88. This is presented in Table 3, together with basic descriptive statistics. Most distributions of scores in both groups converged toward higher values of scales, except for aggressiveness and positive and negative valence, which converged toward lower values.
Between the two groups of subjects, differences were found in almost all scores on the VP+2 scale. In neuroticism, t(249) = -4.881, p < .000, η2 = .09; aggressiveness, t(249) = -3.754, p < .000, η2 =.05; and negative valence, t(249) = -3.562, p < .000, η2 = .05, higher values were found in the group of patients with previous suicide attempts, while extroversion, t(249) = 3.274, p < .001, η2 = .04, and conscientiousness, t(249) = 3.464, p < .001, η2 = .05, scores were higher in the group of patients without previous suicide attempts. Effect sizes were large for neuroticism and small in other personality dimensions.
Similar to previous section, analyses have shown that personality dimensions vary along certain demographic characteristics. In the group of patients with previous suicide attempts, males scored higher in negative valence, t(81) = 2.614, p = .011, η2 =.08, while in the group of patients without previous suicide attempts females scored higher in conscientiousness, t(166) = 2.677, p = .008, η2 = .04.
Relation between Suicidality, Temperament, and Personality Dimensions
The main aim of this study was to predict suicide attempts in depressed patients through personality dimension model VP+2 and affective temperaments TEMPS-A.
After including only affective temperaments in binary logistic regression analysis (Table 4), the model correctly classified 70.9% of cases by suicide attempt, with “depressive” and “irritable” temperaments being the only important predictors, goodness of fit, χ2(6) = 38.092, p < .01. The model predicted between 14 and 20% of the variance.
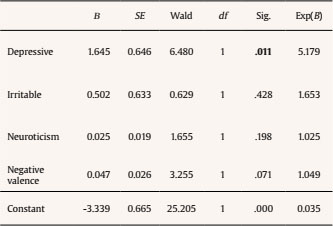
For VP+2 (Table 4), the model correctly classified 73.3% of cases, with “neuroticism” and “negative valence” being the only important predictors, goodness of fit, χ2(7) = 37.805, p < .01. The model predicted between 14 and 19% of the variance.

In the final step, on combining all variables that were previously found statistically significant in predicting suicide attempts (Table 5), we created a model which successfully classified 72.5% of cases, goodness of fit, χ2(4) = 39.488, p < .01. However, only “depressive temperament” was found to be a significant positive predictor (higher scores on depressive temperament predicted more suicide attempts in patients with depression). Out of all other variables, only “negative valence” was close to statistical significance. The model predicted between 15 and 20% of the variance.
Discussion
This study was focused on patients suffering from depression, since suicidal behaviour most commonly occurs in this population. We compared groups of depressed patients with and without previous suicide attempts.
There were no differences between the two groups in terms of gender, age, education, and marital status, which facilitated further comparisons between these groups since they were balanced with regard to most frequent control variables. The results of our study have demonstrated that the group of patients with previous suicide attempts diagnosed with depression scored higher on TEMPS-A in all types of affective temperaments other than hyperthymic, with the highest differences in depressive temperament (large effect size) and irritable temperament (small effect size). These results are similar to recent studies, particularly a meta-analysis conducted by Vázquez and associates (Vázquez et al., 2018). These authors found a significant and consistent relationship between previous suicidal behaviour and higher scores in depressive, cyclothymic, irritable and anxious affective temperaments, and lower scores on hyperthymic temperament. This meta-analysis identified depressive and irritable temperaments as particularly strongly associated with suicidal behaviour. We found similar results using a logistic regression model – depressive and irritable affective temperaments were significant predictors of suicide attempts on entering only affective temperaments. This could be explained by the fact that combination of depressive and irritable affective temperament is linked with tendency toward mixed mood states in depression, which have already been identified as an important risk factor for suicide (Perugi et al., 2015). What is more, aggressive outbursts and increased impulsivity, that are typical of irritable temperament (Akiskal et al., 2005; Ristić-Ignjatović et al., 2014), may make a difference to why some patients with depression attempt suicide while others never do.
The group of patients with previous suicide attempts scored significantly higher on neuroticism, aggressiveness, and negative valence, while the group of patients without previous suicide attempts scored significantly higher on extroversion and conscientiousness. Neuroticism and negative valence were also significant predictors of suicide attempts on entering only personality (character) traits. There are few reviews in literature with current knowledge about the connection between Big Five personality dimensions and suicidality. A review that included all three types of suicidal behaviour identified hopelessness, neuroticism, and extroversion as connected with suicidal ideation, suicide attempts, and completed suicides to the greatest extent (Brezo et al., 2006). According to the Big Five model, neuroticism is described as negative affect, depressiveness, and anxiousness (Čolović et al., 2014), and it is therefore expected for neuroticism to be mostly related to maladaptive coping mechanisms and negative affect (Gunthert et al., 1999). Results of prior studies have found a connection in personality traits between neuroticism, on the one hand, and depression and suicidal behaviour on the other (Bi et al., 2017; Koorevaar et al., 2013; Kumar et al., 2013; Rozanov & Mid’ko, 2011).
Apart from neuroticism, the group of patients with previous suicide attempts in our study showed higher scores in aggressiveness (anger, intransigence, hardheadedness), as well as negative valence (manipulativeness and negative self-image). Both concepts are similar – while aggressiveness could be considered as open aggression, negative valence is more in line with passive aggression. Aggressiveness is a personality dimension which has already been linked with suicidal risk, and it was considered to be an important mediator between depression and suicidality (Isometsä, 2014; Liu et al., 2017). Aggressiveness and negative valence are also highly intercorrelated and it is thus no surprise that negative valence is a significant predictor of suicide attempts in this study.
Results of a new Chinese study found higher levels of neuroticism in the group of suicidal patients with a psychiatric diagnosis, compared to those without a psychiatric diagnosis who scored higher on impulsivity (Bi et al., 2017). This study also found that suicidal subjects without a psychiatric diagnosis were under higher environmental stress (interpersonal conflicts, alcohol abuse, etc.) prior to the suicide attempt, while the clinical group had higher levels of suicidal risk and depressiveness.
The group of patients without previous suicide attempts in our study scored higher in extroversion and conscientiousness, which is concordant with findings from other studies. Several studies have shown that patients suffering from depression score higher on neuroticism, and lower on extroversion and conscientiousness, which are protective factors for suicidal behaviour (Blüml et al., 2013; Koorevaar et al., 2013; Petersen et al., 2001).
The only other study assessing both affective temperaments and personality dimensions as risk factors for suicide was carried out by Pompili et al. (2018). This study found that patients at risk of suicide have specific temperaments and personality profiles – they are characterized by depressive traits; predominant affective temperaments were irritable and anxious, and the predominant personality dimension was social introversion (which is comparable to negative valence in our sample). Even though patients with other diagnoses were included in this study as well, the results are comparable to our sample, pointing to certain risk factors as being present in suicidal patients regardless of diagnosis.
Limitations
Our study had a few limitations. First of all, considering that this is a cross-sectional study, drawing conclusions about causality was not possible. The second limitation was related to the fact that only self-evaluation instruments were used. Furthermore, we did not use instruments for assessing the current affective status of patients, thus not being able to determine whether these findings are state or trait dependent.
Conclusion
According to the results of our study, depressive and irritable affective temperaments, as well as neuroticism and negative valence, have been identified as significant predictors of suicide attempts in patients suffering from major depressive disorder. Once all significant predictive variables have been included into the model, the depressive affective temperament trait remained the only significant predictor of suicide attempts. This could be explained by the high intercorrelation between variables included in the prediction, most notably between depressive temperament and neuroticism, as well as irritable temperament and negative valence.
Prominent depressive affective temperament or a combination between depressive and irritable affective temperament, together with high neuroticism and negative valence, are personality characteristics of patients with major depressive disorder that require considerable caution due to suicide risk associated with these patients.

