










 Custom services
Custom services
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkContribution to scientific literatura
This article intends to state the importance of the creation of interdisciplinary teams for the management of medical supplies. Ulcer development is a complex health issue, with many factors involved and a major impact on patients’ quality of life, and associated to a significant economic cost; therefore, a rational use of medical supplies is crucial for prevention and pressure ulcers care. However, experiences in the interdisciplinary approach in this area are limited.
The outcomes of this study revealed that the integration of the pharmacist in interdisciplinary teams is an opportunity to improve the management of these products.
Introduction
The population older than 65 years has almost doubled in our country during the last decades, from 11.2% in 1981 to 17.3% in 2011. Future forecasts about population state that by 2050 there will be over 15 million of elderly people, almost twice the current number, and they will represent over one third of the entire Spanish population (36.4%)1. Besides, demographical studies foresee a major growth in functionally dependent elderly population.
With the objective to cover the increasing needs of the population, health and social care resources have experienced a major development in recent years. Currently, elderly nursing homes provide care to a population with increasingly complex health problems, who require multiple types of care, halfway between hospital and home2. These are frequently fragile patients who require an interdisciplinary approach focused on the person, and it is essential to determine a systematic therapeutic plan based on a multidimensional assessment3. Along this line, the WHO has pointed out that collaboration between different professionals improves health outcomes, particularly for those patients with complex needs4.
Pressure ulcers (PUs) represent a frequent complication in immobilized patients, and have a very negative impact on their health and quality of life. In an epidemiological study conducted in 2013 by the GNEAUPP, the prevalence of PUs in the nursing home setting was estimated at 13.4% (CI95%: 12.6-14.2)5. In terms of ulcer care, the European Wound Management Association (EWMA) has prepared a positioning document about their approach by an interdisciplinary team. Its authors state that, individually, the different healthcare professionals have no sufficient skills to address the complex needs of patients with ulcers, and that all members of the interdisciplinary team should share the responsibility to achieve the desired results 6.
In economic terms, the expenditure in medical supplies (MS) represents an average 7.5% of healthcare expenditure in European countries; in Spain, the percentage is 6.2%7. Frequently, at hospital level, the use of MS exceeds the use of medications. In a study conducted in a medical-surgical hospital, wound dressing, gauzes, bandages, and other wound dressing materials were among the groups of MS that originated the higher expenses (15.6%)8.
On the other hand, from a regulatory point of view, Spanish legislation allocates to all healthcare professionals the responsibility for a rational use of MS, and assigns to Pharmacy Units the role of guaranteeing their effectiveness, safety and efficiency9.
The objective of the present article is to describe and evaluate a procedure for MS management in PU care, from an interdisciplinary perspective, and coordinated from a Pharmacy Unit (PhU), with the aim to achieve a rational use of MS in the nursing home setting.
Methods
Setting of the study
The present study has been conducted in the nursing home setting, on centres assigned to a centralized PhU. The study included all elderly nursing homes assigned to the PhU up to 2014. All those assigned subsequently have been excluded, as well as centres for persons with intellectual disability and centres for chronic mentally-ill patients.
Interdisciplinay team
On June 2012, an interdisciplinary work team was created to improve the management and the rational use of MS in those centres assigned to the PhU. The team was formed by the nursing coordinators from the centres where care was provided, and a DUE (Nurse with University degree) from the PhU, as well as the Pharmacist responsible from the Functional Unit of Medical Supplies Management. With the objective of establishing the team priorities, the initial situation was analyzed through an economic study of the expenditure in medical supplies during 2011, on the Group A according to Pareto of the total use of MS (80% of accumulated use).
The team established biannual meetings, and agreed on the following lines of action: selection of products, conditions of use, periodical analysis of the use of MS in the centres, control of stocks in the centres, and epidemiological analysis of PUs in the centres. The economic objective was saving in purchases, at least 10%. Outcomes of team-agreed interventions were assessed.
Lines of action
a) Selection of medical supplies
Based on the centralized public tender issued by the local healthcare authorities, the team conducts a selection of wound dressing and materials to be available at the centres. To this aim, an assessement of the technical characteristics of products, an economic simulation of their use in different scenarios, and a study of their utility in our setting of care is performed.
The ability to select products for PU care has been evaluated through the percentage of products selected in relation to the total range of products available in the current public tender.
b) Conditions of use
A consensus regarding the conditions of use for certain products that require closer follow-up, due to their high cost and/or special conditions of use is reached. In this way, the use of this type of products will require an individual request (Figure 1), which includes information about its use and a section for entering details about the patient and the PU evolution.

c) Periodical analysis of the use of medical supplies in the centres
The PhU provides each centre with information about six-monthly consumption of medical supplies and monthly use per patient of wound care material. The list of products included in the Group A according to Pareto is also included. The team conducts a comparative analysis in order to establish agreed strategies in order to improve the use of medical supplies.
In order to assess the impact of the team interventions regarding the use of medical supplies we calculated for each centre, the difference between the expenses at the beginning of team formation and three years afterwards.
d) Control of stocks in the centres
The interdisciplinary team determines that there must be a control of stocks in the centres at least every six months, in order to minimize immobilized products, adjust the quantities ordered and, ultimately, optimize the management of medical supplies.
e) Epidemiological analysis of PUs in the centres
In order to learn about the situation regarding ulcer care in the centres, and establish common strategies of care, a descriptive retrospective study was conducted in 2014 about the risk of development of PUs and patients with PUs. The following information was collected every six months for each centre: number of beds, number of patients admitted during that period, number of patients classified into each risk category according to the Norton scale, number of patients with PUs, number of PUs at the start of the semester and during the semester, number of patients with new PUs and number of PUs with external origin (hospital, home, other nursing homes). This information was provided biannually to the PhU directly and voluntarily by professionals.
The descriptive analysis conducted in 2014 has been presented through the distribution of patients according to their risk of PUs, the prevalence and incidence of ulcers and patients with ulcers, as well as the percentage of ulcers with external origin (hospital, home, other nursing homes). Additionally, the prevalence of ulcers at the start of the second semester of 2014 has been calculated. No previous data were available.
Results
An interdisciplinary team was formed with representatives from 18 elderly nursing homes with a total number of 1,599 beds.
Data collected analysis on healthcare expenses by the PhU of the La Cañada Nursing Home during 2011 revealed a 21% expenditure in medical supplies in relation to the total expenses (medications and MS). Table 1 shows the list of products included in the Group A according to Pareto, calculated for the whole set of centres in 2011. Products for ulcer prevention and healing represented 72% of the total expenditure on medical supplies. Within this group, the first six products were foam wound dressings (53.9% of the accumulated consumption).

Seven meetings have been held, with a mean of 12.7% attendants per meeting since the creation of the team on June 2012 and until December 2015.55.5% of nursing staff representatives of the centres attended at least half of the meetings.
During the first 12 months of follow-up, the monthly savings of wound-care materials purchasing was at least 17% (median= 36.4%; range= 17.5 to 54.9) with regard to the 12 months previous at the creation of the team.
After the assessment process, 27 products (15%) were selected from the 180 offered in the tender process. Table 2 shows the proportion of products from each category. In eight categories, the percentage of products selected was less than 25%, including foam wound dressings, silver wound dressings, hydrocolloids and alginates.
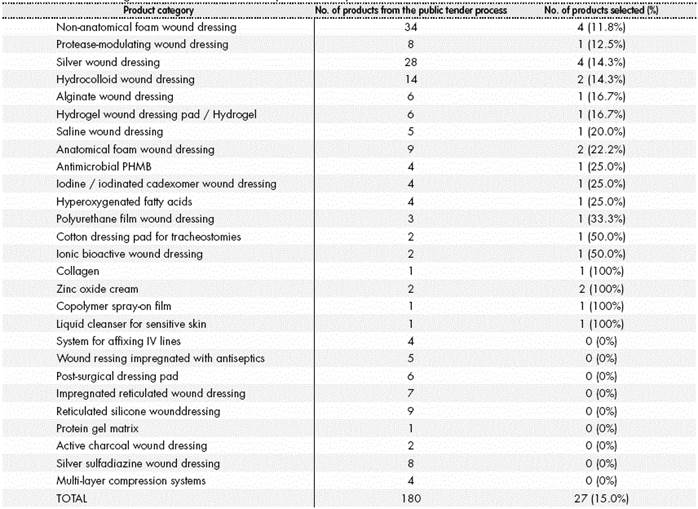
The interdisciplinary team agreed on the individual request for five products: ionic bioactive wound dressings, protease-modulating dressings, saline dressings, polyhexamethylene biguanide antimicrobial dressings (PHMB), and iodinated cadexomer dressings.
In 16 centres there was a reduction in the use of wound dressing materials. The median differences in the use of these products was -32.3% (range= -95.9 to 100). Besides, a reduction in use of more than 50% was confirmed in 7 centres (38.9% of the total). The distribution of the variation of use in the centres is represented in Figure 2.
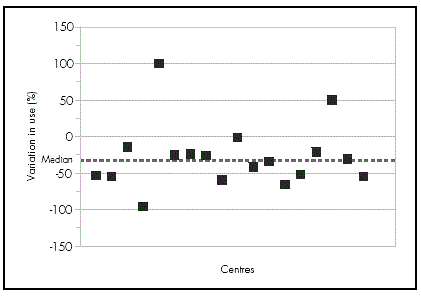
Table 3 summarizes the information about the risk of PU and patients with PUs in 2014, broken down into semesters. This table includes data from 12 centres, which are different for each semester. More than 45% of patients admitted to the centres had medium or high risk of developing PUs. In the second semester, there was evidence of a higher incidence of patients with ulcers (2.15 new cases/100 patients/month). The prevalence of patients with ulcers (cases/ 100 patients/month) was 2.76 in the second semester. The prevalence of patients with ulcers and the prevalence of ulcers, calculated at the start of the second semester of 2014, was 4.91% and 5.59%, respectively. Regarding the origin of ulcers, the fourth part of them were originated outside the nursing homes.

Discussion
The involvement of the pharmacist in interdisciplinary teams orientated towards the rational use of medication has become increasingly more relevant in the different settings of care. However, this involvement is still limited in the case of medical supplies, regardless of the high cost these represent, both at hospital level and in the nursing home setting. On the other hand, due to the fast technological innovation, these products are reaching high technical levels of complexity, requiring a wide knowledge and experience for their management.
Given the impact in terms of health, quality of life, and associated economic costs represented by the development of PUs in institutionalized elderly patients, it is essential to address the care of Pus and the management of the wound dressing materials as a team.
The creation of an interdisciplinary team coordinated by a PhU in the nursing home setting has allowed to conduct interventions targeted to a rational use of medical supplies. The involvement of the centres in the team can be considered satisfactory, taking into account the number of attendants per meeting. In our setting, different factors determine the involvement of the professionals of the centres, such as the geographical distance between the centre and the PhU, as well as the diversity of companies managing the centres and the PhU.
The outcomes obtained in the present study confirm that products for PU prevention and care represent a significant expenditure in the nursing home setting (72% of the total expenses in medical supplies); therefore, the interdisciplinary team focused their efforts on an efficient use of this group of products.
As our study shows, the management of medical supplies by an interdisciplinary team formed by nurses and pharmacists leads to positive outcomes in economic terms, presenting significant savings in the purchase of wound care materials during the follow-up period. This goes in line with the EWMA report, which points out the economic savings as one of the benefits of working in teams in chronic wound care, and provides positive outcomes in terms of ulcer cure and amputation rate6. Likewise, the experience of teams formed by nurses and pharmacists demonstrates, in a cost-effectiveness study about ulcer care in elderly nursing homes, that the interventions led to significant savings in costs, as well as an improvement in outcomes, measured as the proportion of cured ulcers and the time needed until complete cure10. One of the most relevant team interventions has been setting up an interdisciplinary procedure for the evaluation and selection of medical supplies, based on clinical and economic criteria. The selection process has been assessed as very positive by the members of the team, and the selection of medical supplies made covers the majority of needs of the persons under care. Besides, given that the selection limits the number of products managed in the centres, there is a simplification of management procedures in terms of ordering, storage and dispensing processes, as well as the review of expiration dates, etc.
On the other hand, this study has shown the variability of the information collected in the different centres regarding the record of ulcers and the use of different cut-off points for the scale of ulcer-risk assessment. This fact is a consequence of the different management and organization of each centre, and it can have an impact on the level of care assigned to patients, according to the centre where they are living. Moreover, from a statistical point of view, this variability leads to bias in the calculations made, and therefore represents a limitation to compare our data with other studies. This situation has been the basis to develope a document of consensus in order to standardize ulcer records in the centres.
Regarding the epidemiological analysis of PUs in the centres, it is observed that the institutionalized population in our setting presents major frailty characteristics, because more than 45% are at medium or high risk of developing PUs. In terms of PU prevalence, the value calculated at the start of the second semester of 2014 was 5.59%. This percentage is significantly inferior to the one reported in the 4th National Study of Prevalence of PUs elaborated by the GNEAUPP in 2013, which states a 13.4% prevalence of PUs in nursing centres4. This difference can be partly explained by the variability of ulcer records in the centres, and there could have also been a non-response bias, because it is possible that the data reported mainly came from those professionals more motivated in terms of preventing and addressing PUs.
Finally, the care setting where the PUs were originated has been studied. It is worth highlighting that one in four PUs are originated outside the centres.
This value is similar to the one found in the study by the GNEAUPP, where 34.8% of PUs recorded in nursing centres have an external origin4. Other study in a medium and long stay nursing centre calculated a mean prevalence of external ulcers of 20.5%11. This high proportion of ulcers originated in settings outside the nursing homes reveals the need to develop programs for PU prevention that include the different levels of care in a coordinated way, thus minimizing the negative effects of transition of care.
This study states that the creation of an interdisciplinary team, where the pharmacist gets closer to patient needs, and nursing professionals share responsibility for selection and management of medical supplies, generates a setting of collaboration between professionals, leads to positive results regarding the rational use of medical supplies, and represents an opportunity for improvement in patient care.

