










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkIntroduction
The definition of gender violence or violence against women varies considerably according to variables such as the legal system of each country, and the sphere of action (e.g., legal, scientific, political, philosophical spheres; European Union Agency for Fundamental Rights, 2014). Nevertheless, in operational terms, the United Nations (1993) has defined violence against women victims as “any act of gender-based violence that results in, or is likely to result in, physical, sexual, or mental harm or suffering to women, including threats of such acts, coercion, or arbitrary deprivation of liberty, whether occurring in public or in private life” (Article 1). Succinctly, gender-based violence is any act directed towards a woman that leads to harm, including psychological injury.
Psychological harm is assessed differently in clinical and forensic evaluation. Thus, only posttraumatic stress disorder (PTSD) constitutes psychological harm in forensic evaluation (PTSD being the definition of psychological harm in forensic settings), but not other disorders leaving no trace of PTSD or PTSD subsyndromes (O’Donnell, Creamer, Bryant, Schnyder, & Shalev, 2006). PTSD is the psychological trace of victimization of a crime leading to the development of clinical symptoms resulting from the exposure to the traumatic event (crime). This ensures compliance with the legal prerequisite of establishing a causal relation between the alleged events (crime) and psychological harm (the psychological trace of victimization). Comorbidity and epidemiological studies have corroborated this relation (Kessler, Chiu, Demler, & Walters, 2005; Kessler, Sonnega, Hughes, & Nelson, 1995). Notwithstanding, in PTSD the traumatic event restricts the cause to specific criminal acts, fundamentally threats or physical and/or sexual assault. Hence, the diagnosis of PTSD leaves aside stressful events of a criminal nature which are neither relevant in type nor severity such as psychological and economic violence, or violations of fundamental human rights (Arce, Fariña, & Vilariño, 2015). As traces of psychological injury are restricted to PTSD, and other stressful events do not cause psychological injury (PTSD), there may be neither victim, nor crime. In these cases, if the remaining criteria of the PTSD diagnosis are fulfilled, the diagnosis is adjustment disorder (AD) (i.e., trace of psychological injury). Finally, the acute stress disorder (ASD) also constitutes a psychological trace of harm, whose differential diagnosis to PTSD rests on the symptom pattern being limited in duration from 3 days to 1 month, after which it becomes PTSD, that is, it is the same disorder, and thus constitutes a trace of psychological injury. Furthermore, forensic evaluation is required by courts to control the feigning of injury, that is, to guarantee the veracity of injury. Likewise, in both the DSM-IV and DSM-IV-TR a feigning differential diagnosis is mandatory in clinical evaluations in forensic settings (American Psychiatric Association - APA, 1994, 2000). Though this differential diagnosis has been deleted from clinical evaluation in the DSM-5 (APA, 2013), to become only a criterion of suspected feigning, this is not so for forensic evaluation where it remains mandatory. For this double evaluation of tracing psychological injury and detecting malingering, a multi-method approach combining the clinical interview with psychometric measures is essential (Rogers, 2008). Thus, standard clinical interviews, such as the SCID-5 (First, Williams, Karg, & Spitzer, 2015), are not valid as they lack an instrument for the feigning differential diagnosis, fail to establish a causal effect between the criminal act and psychological injury, and facilitate the feigning task by evaluating individuals according to a symptom recognition task (the individual is asked about symptoms). Thus, the forensic-clinical interview was designed and validated to overcome these three limitations in forensic evaluation (Vilariño, Arce, & Fariña, 2013).
In clinical assessment, PTSD should not be diagnosed if the symptom response pattern to the extreme stressor meets criteria for another mental disorder (e.g., depressive disorders, anxiety disorders), and these should be diagnosed instead of (or in addition to) PTSD. Accordingly, the clinicians’ primary diagnosis should be comorbid disorders to PTSD. As for comorbidity, PTSD is highly comorbid and estimated to range from 80 to 98.8%, with high rates of comorbidity and multi-comorbidity (APA, 2013; Brady, Killeen, Brewerton, & Lucerini, 2000; Kessler et al., 1995; Kulka et al., 1990). PTSD comorbid disorders are diverse, and depressive and anxiety disorders are among the most comorbid disorders to PTSD (Beydoun, Beydoun, Kaufman, Lo, & Zonderman, 2012; Elhai, Grubaugh, Kashdan, & Frueh, 2008; Kessler et al., 1995; Kessler et al., 2005; Rytwinski, Scur, Feeny, & Youngstrom, 2013).
Nevertheless, clinical diagnosis of PTSD should not be transferred to forensic determinations unless malingering is suspected. Thus, clinicians fail to diagnose malingering as it is not suspected in clinical setting (Rogers, 2008). But comorbidity, and mainly multi-comorbidity to PTSD with another or other disorders, is strongly related to severity (Kessler et al., 2005). Finally, clinical assessment may not guarantee the establishment of a causal relationship between the traumatic event (crime) and PTSD (clinical diagnosis does not imply the reality of Criterion A, the cause).
Nonetheless, these results were from the community and specific populations (e.g., war veterans), and not from women victims of gender violence (committed by a partner or ex-partner), where legal efforts are being developed worldwide to eradicate gender violence. Thus, a field study with adjudicated victims of gender violence (confirmed by unappealable legal judgement) was undertaken to evaluate the prevalence of symptoms, mental disorders, and comorbidity, and to quantify psychological harm in mental health markers in WVs-IPV.
Method
Participants
A total of 50 women victims of intimate partner violence (WVs-IPV), aged 19 to 64 years (M = 37.42, SEM = 1.50), participated in the study. All of the participants had reported the crime to the police and had undergone trial with an unappealable conviction of the aggressor (partner or ex-partner). In all cases, the judicial judgements confirmed victimization of physical and psychological violence.
Design and Procedure
The study design aimed to measure psychopathological symptomatology in a sample of real victims of gender violence by comparing the data obtained with that of the general normative population obtained with the SCL-90-R measurement instrument (Derogatis, 2002). The design sensitivity test (1-β) found, for an expected medium effect size, a sensitivity of .97, that is, the probability of detecting significant mean differences (α < .05) in the study between victims and the normative population would be, a priori, 97%. As for the comparison of proportions with a constant (.05), and an expected medium effect size, the design sensitivity was .99. Thus, the data analysis design was sensitive (> .80).
Data on WVs-IPV was gathered from the files of the Forensic Psychology Unit of the University of Santiago de Compostela, Spain. Strict inclusion criteria were applied to guarantee all cases of violence were real and, considering that in judicial cases of gender violence one must suspect attempts to falsify the truth in order to obtain a benefit (APA, 2013), the ground truth was taken to be the final court judgement (an “unappealable judgment”). Of the total final court judgements, in 32 (64%) the accused accepted the guilty plea, that is, the accused admitted the crime, and in 18 (36%) of judgments the evidence of guilt was overwhelming (e.g., expert reports, testimonies, violations of restraining orders), and exceeded the burden of proof for convicting the accused (Judgement of the Spanish Supreme Court: the principle of the presumption of innocence demands that no innocent persons should be found guilty, whereas it is suffice for the guilty to be generally convicted; sentence of the Spanish Supreme Court nº 213/2002, de 14 de febrero). In no case were the evaluations of the present study used as evidence in court.
Participants were assessed by a research psychologist trained and experienced in clinical evaluations. Participants were informed about the study aims and the relevance of the implications for forensic practice. All participants freely volunteered and gave written consent. Data were processed according to Spanish Data Protection Law (Ley Orgánica 15/1999, de 13 de diciembre, de Protección de Datos de Carácter Personal).
Measurement Instrument
Evaluation of psychological adjustment was undertaken using the Spanish adapted version of the SCL-90-R [Symptom Check List-90-R] of Derogatis (2002). This checklist consists of 90 items for individuals to report their psychological, psychiatric, and somatic symptoms that are structured in 9 symptomatic dimensions: somatization (α = .86), obsession-compulsion (α = .86), interpersonal sensitivity (α = .86), depression (α = .90), anxiety (α = .85), hostility (α = .84), phobic anxiety (α = .82), paranoid ideation (α = .80), and psychoticism (α = .77). Additionally, 3 global distress indexes were applied: the Global Severity Index (GSI), the Positive Symptom Distress Index (PSDI), and the Positive Symptoms Total (PST).
Data Analysis
The analysis of the effects on the symptomatic dimensions and distress indexes in the population of victims of gender violence was performed by comparing the mean for the population under study with the normative population mean (test value; a normative sample was preferred as a comparative group to a control group, as the latter is always biased in relation to the experimental group; Schmidt & Hunter, 2015), using one sample t-test. Mean injury in WVs-IPV (comparison of mean injury in the sample under study with the baselines, the means for the normative population; Corras et al., 2017; Seijo, Fariña, Corras, Novo, & Arce, 2016) was quantified in each dimension using the BESD (Rosenthal & Rubin, 1982), which served to obtain the lower and upper limits of injury for 95% of the sample, and calculate the minimum and maximum injury values. True psychological harm was estimated (ρ) correcting r through attenuated correction (criterion unreliability).
On the premise that the sample of the study, although it was gathered by a purposive sampling, shares the same characteristics measured being representative of the population of victims in the measured injury (i.e., homogeneity of the population in psychological harm), the generalization of the results to the population was analysed. Moreover, to analyse the generalization of the results to other studies with other samples of the same population, the 95% confidence interval (CI) for the true effect size (ρ) was calculated; if the CI does not include zero, 97.5% of other studies with women victims would obtain a mean minimum effect size above the lower limit of the interval (difference in terms of standardized ρ scores between the sample of WVs-IPV and the normative population) (Jacobson & Truaux, 1991; Schmidt & Hunter, 2015). Effect size was computed, as mean comparisons were made, in Cohen’s d. Then, the effect size was corrected for attenuation (true effect size, δ). Confidence intervals for δ were computed, obtaining standard error from Schmidt & Hunter’s (2015) formula.
Nevertheless, as this study dealt with mental health (APA, 2013) with legal (victims of a crime, including violence against women, are defined according to the injury sustained such as injury to mental health; United Nations, 1988, 1993), and forensic implications (in forensic practice the designs are N = 1), the study of means must be complemented with the study of cases. Thus, the 80% credibility interval for δ was computed, and if it did not include zero the injuries would be generalizable to 90% (90% of victims would have a standardized δ score, a higher score than the lower limit of the interval) of victims of gender violence (Fariña, Redondo, Seijo, Novo, & Arce, 2017), and the clinical significance was computed (study of cases; Jacobson & Truaux, 1991) to estimate the probability of severe clinical injury.
Owing to their value in deriving implications for clinical practice and forensic evaluation (Amado, Arce, & Herraiz, 2015), the statistical probability of superiority (PS) was calculated, that is, the probability that a WVs-IPV would obtain a higher score (injury) than women in the normative population, and the U2, which is an estimate of the probability of correctly classifying WVs-IPV as real cases.
The classification of WVs-IPV as caseness (severe) was performed taking a score higher than Z of 1.96 (clinical significance; Jacobson & Truaux, 1991) in the normative sample (≈ T70) as the criterion (cut-off score). As a Z score of 1.96 has a one-tailed confidence level (1-α = .975, P97.50) of .025, then the registered probability among WVs-IPV over this score was contrasted in each dimension and index with a constant (.025, expected probability of caseness into the normative sample). Effect size was estimated by odds ratio; 95% confidence intervals for the observed proportion of caseness were obtained. If confidence intervals had no zero, the results may be generalized to other studies from the same population as the sample would be representative of the population. Additionally, the observed proportion lower limit interval was compared with a constant (.025). Significant differences would inform that the minimal observed proportion of caseness in other studies would be greater than in the normative population. Though in forensic practice injury must implicate the diagnosis of the disorder (all criteria should be met), the psychometric instrument only provides a diagnostic impression (the diagnosis corresponds to the clinical interview); moreover, not all injuries have clinical significance. Thus, in forensic evaluation, the psychometric measure is taken as an indicator of validity convergent with the measure of the clinical interview. Additionally, the cut-off point was established to determine when an individual would fall into the region of a potential clinical case. Addressing this issue, the Spanish manual of the SCL-90-R (Derogatis, 2002) classifies a case as clinical if the GSI (or, alternatively, two symptomatic dimensions) is higher than the 90 percentile of the normative population. This cut-off corresponded approximately to a Z score of 1.28 (one-tailed, 1-α = .90, P88.49). This classification would correspond with moderate deterioration in categorical terms. Consequently, the score ranges corresponding to a Z of 1.28 and 1.96 in each dimension and index were calculated.
Cohen’s categories for classifying effect sizes were employed: small (d = 0.20), moderate (d = 0.50), and large (d = 0.80), with an additional category “more than large” effect size. Arce, Fariña, Seijo, and Novo (2015) created this category for extra-large effect sizes in several settings (e.g., forensic, personnel selection), where intentional distortions of the responses must be suspected. This is defined by a Cohen’s d of 1.20, that is, the mean difference between the compared groups was larger than 1.20 SD (Z = 0.849) corresponding to a percentile of 80.23, i.e., 80.23% of the possible effect sizes obtained would be below this criterion (P55.57, P63.68, and P71.57 for small, moderate, and large effect size, respectively). To convert effect sizes, the tables from Salgado (2018) were used.
In addition to the design sensitivity of the data analysis comparing the means and the expected intermediate effect size being good (≥ 97%), the effect size found in each analysis and sample size, with an α of .05, was estimated, and the sensitivity of the data analysis in detecting differences in each comparison. This finding may be crucial for the interpretation of the results, since the ratio between α and β, where β is higher than α, indicates a conservative bias in the results (tendency to minimize injury in victims).
Results
Estimated Injury in Mental Health Markers in the Population of Women Victims of Gender Violence
The results of the comparison of symptom dimensions in WVs-IPV revealed that victimization had significant effects (more symptoms) in all dimensions (see Table 1). Indeed, women victims of gender violence reported more somatic symptoms, a mean 36% of the sample (ρ), ranging (study of cases) from women with 9% injury (lower limit of the confidence interval for ρ) to 58% (upper limit of the interval); 53% in obsession-compulsion, ranging from 30 to 70%; 45% in interpersonal sensitivity, ranging from 19 to 64%; 53% in depression, ranging from 30 to 70%; 48% in anxiety, ranging from 23 to 67%; 20% in hostility, ranging from women without any effects in the manifestation of hostility (negative lower limit) to women with an increase of 45%; 44% in phobic anxiety, ranging from 18% to 64%; 43% in paranoid ideation, ranging from 17% to 63%; and 38% in psychoticism (in non-psychiatric populations it was related to social alienation and not primary psychotic symptoms; Fariña, Arce, Vilariño, & Novo, 2014), with an increase in more psychotic symptoms ranging from 11% to 59%. The results were not only significant, but also highly powerful (power ≥ .99), with a good equilibrium between power and significance (α/β ≈ 1), except for the hostility dimension, in which the relation α/β = .33, that is, the probability of the true effects was more significant, and 3 to 1 bigger (in comparison to the probability of them being lower or less significant; bias in line with a type II error); an effect size in the quantification of injury from small-moderate (.10 > ρ < .30) in hostility; and from moderate-large (.30 > ρ < .50) in somatization, interpersonal sensitivity, anxiety, phobic anxiety, paranoid ideation, and psychoticism; and large (ρ > .50) in obsession-compulsion and depression. These results are generalizable to other studies with the same population (the 95% confidence interval for ρ did not include 0), with the exception of the hostility dimension where there may be studies without effects or slightly negative ones (less hostility). Nonetheless, the adverse effects in the health dimensions were not generalizable to the population of women victims of gender violence (the 80% credibility interval for δ included 0). Finally, the probability of finding higher scores (HS) in the different symptomatic dimensions in the population of women victims of gender violence (as compared to the normative population) ranged from 61% in hostility to 80% in depression and obsession-compulsion, whereas the correct classification of victimization of gender violence (U2) derived from the scores of the clinical dimensions ranging from 16% in the hostility dimension (58%, that is, 8% higher than the random 50%, and 16% higher than the total, 100%) to 46% in obsession-compulsion and depression.
Table 1 Contrast of the IPV-Vs and the Normative Sample in the Symptom Dimensions and Distress Indexes. One-sample t-Test
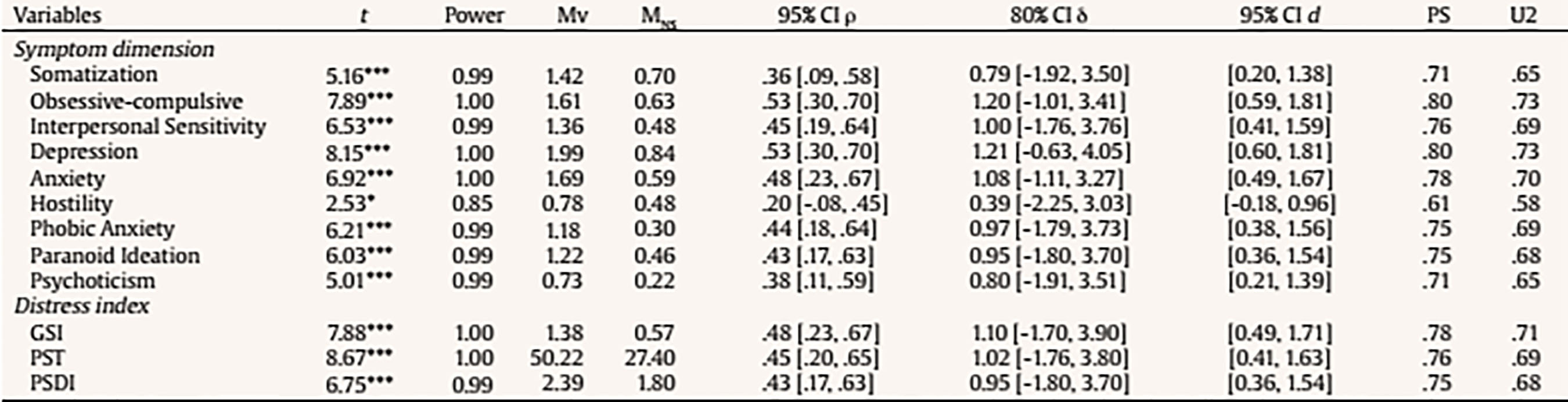
Note. df(49). MV = mean of the IPV-Vs group; MNS = test value, mean of the normative sample.
As for the global psychological distress indexes (see Table 1), the results showed higher global severity (GSI), more positive symptoms (PST), and higher distress related to positive symptoms (PSDI), linked to victimization in gender violence, leading to a 48% mean increase in global severity, ranging from 23% to 67% of the 45% of the positive symptom total, ranging from a minimum of 20% to a maximum of 65%; and of 43% of distress referring to positive symptoms, ranging from 17% to 63%. These results were both statistically significant and highly powerful (power ≥ .99), and generalizable to other studies in the same population (the confidence interval did not include 0). Notwithstanding, psychological distress was not generalizable to all women victims of gender violence (the credibility interval included 0), given that victims may exhibit adverse effects, no effects, or even distress indexes below the mean for the normative population. As for the estimates of the probability of superiority (PS), the results revealed that the probability of victims exhibiting higher severity, more positive symptoms, and higher distress in positive symptoms as compared to the general population was 78, 76, and 75% respectively. With reference to the classification of victimization (U2), the GSI correctly classified 42% of victims, with a PST of 38% and a PSDI of 36%.
Epidemiology of Clinical Cases and Mental Health Markers in Women Victims of Gender Violence
In terms of epidemiological cases (clinical significance), the measures enabled both dimensional and a global estimates. On the dimensional level (see Table 2), 30% of victims of gender violence were classified as significant (significance rate higher than .025, which was the probability of individuals from the normative population with a zeta score above or equal to the 1.96 cut-off score), such as the cases of 30% somatization, 38% obsession-compulsion, 42% interpersonal sensitivity, 48% depression, 44% anxiety, 14% hostility, 48% phobic anxiety, 38% paranoid ideation, and 32% psychoticism. These results were both significant, powerful, and generalizable to other studies on populations of women victims of gender violence (the 95% confidence interval for the probability of cases did not include 0, i.e., there will always be cases in all of the dimensions). Moreover, the minimum probability of cases in the WVs-IPV population in each dimension (lower limit of the confidence interval), with the exception of the hostility dimension, was significantly higher (i.e., similar results were obtained in other samples of the same population) than the probability expected for the general population (see Z2 in Table 2). Likewise, the effect sizes were large (OR ≥ 4.25, d ≥ 0.80) in hostility (i.e., 5.6 times more probable to find cases in the population of women victims gender violence than in the normative population); and more than large (OR ≥ 9.6, being equivalent to a Cohen’s d of 1.25, i.e., the probability of cases in the population of women victims of gender violence was more than 9.6 times higher than in the normative population), in somatization, obsession-compulsion, interpersonal sensitivity, depression, anxiety, phobic anxiety, paranoid ideation, and psychoticism. Accumulatively, 62% of the WVs-IPV were classified as clinical cases (severe injury) in at least one clinical dimension, and 52% in two or more dimensions.
Table 2 Clinical Significance (Caseness) in the Symptom Dimensions and Distress Indexes

Note. 1Spanish female norms ≥ Z 1.96 (one-tailed confidence level = .025); f(p) = frecuency (proportion); Z1= zeta score for the comparison of the registered proportion of caseness among IPV-V with a constant (.025); OR = odds ratio effect size; 95% CIp= 95% confidence interval for p (observed proportion); Z2= zeta score for the comparison of the registered proportion of caseness among IPV-V with a constant (0.25).***p < .001.
At a global level, the GSI, PST and PSDI indexes (see Table 2) significantly classified as caseness (over .025) 48%, 38%, and 42% of the WVs-IPV, respectively, with a more than large effect size (OR ≥ 9.6). Significant effects may be generalized to other studies (see 95% CIs for p in Table 2) on the same population (CIs for the observed probability of cases did not pass zero); and the lower probability of cases in the population of WVs-IPV (lower limit of the interval) was significantly higher than in the normative population (see Z2 in Table 2), that is, the probability of severe injury in the three global indexes would be significantly higher than in the normative population in all of the samples taken from the population of WVs-IPV. Additionally, 58% of the WVs-IPV were classified for severe injury in one or more distress indexes.
The analysis of the results on the prevalence of moderate clinical injury showed it was only significantly higher than in the normative sample in the depression dimension, and the global PST index (see Table 3). Finally, the prevalence of moderate and severe injury in the population of WVs-IPV exhibited a similar pattern of results to severe injury (see Table 3).
Table 3 Moderate Deteriorate and Total Deteriorate (Moderate and Clinical Significance) in the Symptom Dimensions and Distress Indexes

Note. 1Classification criterion as moderately deteriorated where a Z score for 1.28 is the lower limit and the upper limit of 1.96; ftotal(p) = total frequency of moderately deteriorated and clinical significance (probability); Z1 = zeta score for the comparison of the registered proportion of clinical deteriorate among IPV-V with a constant (.075, expected probability among normative population into the range of 1.28 and 1.96 zeta scores); Z2 = zeta score for the comparison of the registered proportion of deteriorated and moderately deteriorated among IPV-V with a constant (.10, one-tailed confidence level for a Z score of 1.28).*p <.05; ***p <.001.
The study of the diagnostic syndrome profiles exhibited higher elevations, i.e., effect sizes (see Table 2) on depression, anxiety, and phobic anxiety (code 457). Secondary elevations were registered in obsessive-compulsion and interpersonal sensitivity (code 457.23). The ordinary diagnosis for this profile in clinical setting is ‘major depressive syndrome’ and, in forensic setting, ‘adjustment/post-traumatic stress disorder’.
Discussion
This study entailed certain design limitations that have implications for the generalization of the results. First, the sample consisted of women whose claim of victimization of gender violence was vindicated by an aggressor’s unappealable legal conviction, thus the generalization to clinical samples (no feigning is suspected; Rogers, 2008) and sociological samples (the legal definition of victim and the self-definition of victim differ) should be taken with caution. Second, the sample was composed almost exclusively by women reporting gender violence or gender violence reported by a third party (cases of severe violence), but excluded women who had not reported their aggressor as a result of the psychological injury itself or for other reasons (Boira, Carbajosa, & Méndez, 2016). Third, the victims of the present study were simultaneously victims of physical and psychological violence as confirmed by the legal judgements (besides being victims of economic or sexual violence, regardless as to whether it was cited or not in the legal judgement), and both are the most common manifestations of gender violence (Lövestad, Löve, Vaez, & Krantz, 2017; Novo, Herbón, & Amado, 2016), that is, mixed violence leading to greater injury to health (Fernández-González, Calvete, & Orue, 2017; Hegarty et al., 2012), whilst in other manifestations of violence injury may have less of an impact (Moral, García, Cuetos, & Sirvent, 2017). Fourth, the measures of injury to health overlapped with the most relevant dimensions of mental health and the most frequent clinical diagnoses (the SCL-90-R was designed on the basis of the DSM), without evaluating directly disorders related to secondary traces of psychological violence such as impulsive or sexual disorders, and those related to drug abuse (Dillon, Hussain, Loxton, & Rahman, 2012; Fariña et al., 2014). Fifth, injury to mental health is neither inevitably nor exclusively the outcome of psychological violence, and may be the consequence of other concurrent causes (e.g., partner breakup, judicial litigation), nor the interaction of gender violence with other factors. Moreover, psychometric evaluation does not establish a causal relation, which rests on the forensic-clinical interview (Vilariño et al., 2013). This underscores the need for evaluating the psychological injury of victimization using a multi-method approach combining psychometric instruments with the clinical interview (Graham, 2011; Rogers, 2008). Bearing in mind the limitations to the generalizations in the present study, the following conclusions may be drawn:
Victimization of gender violence was associated in the population of WVs-IPV to a significant increase in the presence of clinical symptoms in all of the dimensions and distress indicators, and these results were generalizable to other studies in the same population. Nevertheless, not all the victims of victimization of gender violence sustain injury to mental health or psychological distress. Thus, case by case evaluation is required to assess injury by quantifying the dimensions and indexes that are affected.
The probability of the victimization of gender violence leading to an increase in clinical symptoms (does not imply clinical significance, but rather clinical symptoms) affected more than half of the victims in each of the clinical dimensions, ranging from a minimum 61% in hostility to a maximum of 80% in depression (dysphoric experiences, disheartened, anhedonia, desperateness, impotence, lack of energy, self-destructive thoughts, and other cognitive and somatic phenomena characteristic of depressive conditions), and obsession-compulsion (behaviour, thoughts, and impulses considered absurd and intrusive by the person suffering from them, generating anxiety that is difficult to overcome). Furthermore, the distress indicators revealed greater severity in the population of victims, to the extent that approximately 3 of every 4 victims informed of higher severity (78% on the GSI, 76% on the PST, and 75% on the PSDI) than the normative population.
The clinical dimensions were useful for the classification of gender violence and correctly classified the victimization of gender violence in approximately 50% of cases. Moreover, distress indicators correctly classified approximately 40% of the victims. This classification is both relevant and useful for developing forensic techniques requiring a strict classification criterion of victimization, that is, without committing false alarms (classification of non-victims as real victims).
The quantification of injury adjusted to the categories of the DSM (i.e., mild, moderate, severe), with the classification criterion being the Global Assessment Scale (Endicott, Spitzer, Fleiss, & Cohen, 1976), found mild injury in hostility (20%; difference between absent or minimum symptoms – higher limit than normality – and mild symptoms), moderate (30%; difference between absent or minimum symptoms and moderate symptoms) in somatization, and psychoticism, and severe (40%; difference between absent or minimum symptoms and severe symptoms) in obsession-compulsion, interpersonal sensitivity, depression, anxiety, phobic anxiety, and paranoid ideation. The injury measured by the global distress indicators was severe (40%).
The rate of caseness (clinical significance) was significant in all of the dimensions, that is, injury was observed to affect not only forensic psychological traces, but also psychological adjustment as a whole. Thus, once forensic techniques have demonstrated the psychological trace of injury (only injury from PTSD, AD, and ASD constitute forensic traces of injury), and the causal relations with the reported criminal acts, the comorbid disorders also constitute injury and have implications in terms of civil compensation. The clinical significance of the judicial population of WVs-IPV has been substantiated in other communities of Vs-IPV (European Union Agency for Fundamental Rights, 2014; Hathaway et al., 2000; Lövestad et al., 2017).
The classification rate of clinical cases (severe injury) in the sample of WVs-IPV ranged from approximately 50% (two or more dimensions) to 60% (one dimension), that is, severe injury was fundamentally comorbid. Given that the rate of severe clinical cases almost overlapped with the psychological traces observed in victims of gender violence (Vilariño, Fariña, & Arce, 2009) and that the primary diagnosis for the observed clinical profile in the sample was a depressive disorder in a clinical setting and an adjustment disorder in forensic setting, the correspondence in the assessment of injury between the forensic psychological evaluation (psychological trace) and the clinical evaluation of cases (severe injury) in other disorders or dimensions in WVs-IPV was extremely high and multi-comorbid (more than two disorders or dimensions). It is hardly surprising that multi-comorbidity is associated to severe injury (Kessler et al., 2005).
The probability of victims of gender violence presenting moderate injury in the clinical dimensions was not significant, with the exception of depression. Moreover, the rates on the GSI and PSDI indexes were not higher than expected for WVs-IPV, with the exception of PSDI, which was higher than expected. Once again, depression, the clinical injury most comorbid with psychological traces, was significantly prevalent in moderate cases with an increase in injury to positive symptoms, but not in general distress (i.e., GSI, PST). In line with the work of Kessler et al. (2005), bi-comorbidity (comorbidity between two disorders or dimensions) of psychological traces (when diagnosed) with a depressive disorder is linked to less injury (moderate) than multi-comorbidity (severe). It should not be overlooked that the conclusions refer to a population of WVs-IPV, in this case, of psychological traces and a depressive disorder, but other specific cases may differ in the comorbidity disorder and psychological traces.
In line with comorbidity studies on community populations (Kessler et al., 2005; Rytwinski et al., 2013), the highest comorbidity rates with victimization were observed in depression (clinical significance of 48%) and the anxiety dimensions (generalized, 44%, and phobic, 48%).
It should be noted, given its relevance for the judicial evaluation of cases of gender violence and to injury in hostility (thoughts, feelings, and behaviour typical of aggressive states, anger, irritability, rage, resentment), that, even though their effects were small, they may explain instances of a victim’s violent behaviour (14% clinical cases of hostility, and 12% of moderate injury; thus, 25% of victims reported severe or moderate injury in hostility). Violent behaviour may be directed at the aggressor or other family members. When violence is directed at the aggressor, the legal system relies on a tool for interpreting such violence: legitimate defence. However, when violence is directed at other family members, mainly children, cases are judged differently, with a victim of gender violence having direct responsibility in the violence on their own children. But, if violence on children is linked to psychological traces of victimization of gender violence, the judicial reasoning may be otherwise. It is for judges and the courts to determine if an accused is exonerated from responsibility on the grounds of violence being the outcome of injury. In any case, psychological evaluation is able to demonstrate that it is injury associated to victimization of gender violence.
The victimization of gender violence should not be viewed as only a judicial or social issue, but also a public health concern given the extent and severity of the injuries in mental and physical health, and the impact on other family members (Bosch, Weaver, Arnold, & Clark, 2017).
Further research is required to assess the efficacy and value of clinical dimensions and distress indicators in correctly classifying victims, taking into account they are crucial for the development of forensic techniques (forensic task: classification of real victims by controlling the rate of false cases as real, i.e., false positives, would be zero). Moreover, studies should be undertaken to determine the comorbidity and multi-comorbidity rates in victims of gender violence, particularly for psychological traces. Finally, further work is required to examine the mechanisms underlying an aggressor’s violence on a victim, and if it later should be part of an individualized intervention program for aggressors (Arce, Fariña, & Novo, 2014; Carbajosa, Catalá-Miñaña, Lila, & Gracia, 2017; Ferrer-Perez, Ferreiro-Basurto, Navarro-Guzmán, & Bosch-Fiol, 2016; Lila, Gracia, & Catalá-Miñana, 2018; Sjödin, Wallinius, Billstedt, Hofvander, & Nilsson, 2017).

