









My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Salud Pública
On-line version ISSN 2173-9110Print version ISSN 1135-5727
Rev. Esp. Salud Publica vol.92 Madrid 2018 Epub June 06, 2018
ORIGINALS
More than a decade of improvement in medical and judicial certification in the statistics of causes of death
1Servicio de Epidemiología. Consejería de Salud. Murcia. España.
2CIBER de Epidemiología y Salud Pública. Madrid. España.
3Departamento de Ciencias Sociosanitarias. Campus de Espinardo. Universidad de Murcia. Murcia. España.
4Instituto de Medicina Legal y Ciencias Forenses. Murcia. España.
Background:
After the return of democracy to Spain and the assumption of governmental powers by the regional areas, measures were taken to improve cause-of-death statistics. The objective of this study was to describe the evolution of the activities undertaken to improve the quality of mortality statistics in the region of Murcia from 1998 to 2011.
Methods:
A descriptive epidemiological study of all the death documentation processed by the mortality registry in Murcia. Relative quality indicators were used to evaluate the fulfilment of documentation by doctors and court staff. This was backed up by information recovery regarding the causes and circumstances of death, and evaluating the impact on the mortality statistics of ill-defined, unspecific and less specific causes.
Results:
During the study-period, lack of temporal sequence on the medical death certificate reduced from an initial 46% to a final 21% (p<0.001). Retrieval of information from the various sources was successful in 93% of cases in 2001 compared with 38% at the start of the period (p<0.001). Regional rates of ill-defined and less specific causes have reduced more than the national Spanish rates, with a difference of 10.3 (p<0.001) and 2.8 points (p=0.001), respectively.
Conclusions:
Medical certification of death has improved both form and suitability. The regulated recovery of the causes and circumstances of death corrected medical and judicial information. Murcia presented lower age-adjusted death rates of less specific and ill-defined causes than the national average.
Key words: Mortality statistics; Quality control; Death certificate; Cause of death; International Classification of Diseases; Health information systems; Medical informatics; Coroners and medical examiners; Spain
INTRODUCTION
In Spain mortality statistics are produced from a single documentary source, which collates material from three possible origins: the Medical Death Certificate / Statistical Death Bulletin (DC), for the deaths of all who were not stillborn and died of natural causes; the Judicial Statistical Death Bulletin (JDB) for those deaths which involved judicial intervention; or the Statistical Birth Bulletin (BB) for stillborns. This has not always been the case, as the Medical Death Certificate merged with the Statistical Death Bulletin as a single notification form in 20091, and since 2011 the law has specified that liveborn babies who do not survive their first 24 hours should be declared in the DC rather than the BB1,2.
Following Spain’s return to democracy in 1978, and the decentralization of governmental and legislative powers to the Autonomous Communities, action to improve statistics of causes of death was initiated and developed, under the direction of the Spanish Statistical Office (Instituto Nacional de Estadística in Spanish). Among the most notable measures that were undertaken were the codification of death causes by the Autonomous Communities, the development of statistical indicators3, and the medical training on death certification4,5. At the same time, other improvements were introduced, such as the revision of documents and recovery of missing information through interviews with the certifying doctor, from the judicial courts and forensic administration, and/or revision of the clinical reports6.
With respect to the quality of reporting of causes of death, the most frequent errors came from illegible handwriting, lack of the Initial or Fundamental cause of death (the terms in Spain for the disease or condition directly leading to death), lack of physiopathological sequence among the death causes that were provided, and multiple death causes on the same line. Quality has previously been evaluated from several distinct viewpoints and by various agencies, without the existence of official standards. The authors of these evaluations followed their own criteria in assigning codes to imprecise causes of death7,8,9,10,11,12,13,14,15 or reassigned the codes probabilistically16.
Mortality statistics are now undergoing a paradigm shift, from paper-based documentary support and manual coding trough transition to all-electronic, via the Internet, and automated coding processing of death causes from digital documents. For evidence of this, we have only to look at the implementation of the Iris programme for the automated coding of death causes, which has been in place since 201417, or the option of online declaration of JDB information through the Neutral Judicial Point18. Additionally, there is also electronic reporting to the BB in maternity wards19, and planned - though as yet pending - online submissions to the DC from health centres (Spanish Organization of Medical Colleges, Organización Médica Colegial de España, www.cgcom.es/tecnologica/carne). Furthermore, there is the future, and also as yet pending, application of a civil registry law (in vacatio legis) which will index birth, marriage and death for each person (rather than in three separate registries)2.
Therefore, the evaluation of the period during which documentation was paper-based and death causes were manually coded is important - in order to adapt the standards and indicators of quality in the transmission, structuring, and exploitation of cause-of-death statistics to the new digital context.
The objective of this study was to describe the evolution in the quality of death certificates, using indicators for 1998-2011, including: a) medical fulfilment of the forms used for reporting deaths (DC and BB); b) the recovery of additional information regarding the causes and circumstances of the death; and, c) ill-defined, unspecific and less specific causes.
METHODS AND MATERIALS
This was a descriptive epidemiological study based on the analysis of all of the death certificates (DC, JDB, and BB) processed by the Murcia mortality registry between 1998 and 2011 (around 10 000 deaths yearly), in a region of approximately 1.5 million inhabitants, and where a quality programme was already underway. Flowcharts for the epidemiological study and for the documentation of the official Spanish mortality statistics can be seen in figures 1 and 2.


Figure 2 Institutional and documentary flowchart for the production of mortality statistics of death causes in Spain as applied to the region of Murcia
The objective of the death certificate quality programme was to detect formal mistakes on the forms used to report deaths (illegible handwriting, lack of a doctor’s signature, use of abbreviations) - in addition to errors that indicated a lack of knowledge about how to certify the causes-of-death (missing sequences of death causes, or entry of multiple death causes on the same line) (see annex 1 and figure 1). In parallel, those bulletins indicative of deficiencies in need of revision were identified (annex 2)20. This was accomplished by returning to the original sources to obtain additional information that would improve coding of the death causes (illegible fulfilment of forms, ill-defined causes, and lack of a timeline from external causes, like accidents).
The data was recovered by: a) structured telephone interviews with the certifying doctor, with the personnel of the civil registries or judicial administration, which included the Institute of Legal Medicine and Forensic Sciences; and b) through revision of clinical reports. After screening the documents for those that have required revision, the range of documents in need of revision each year ranged between a low of 170 and a high of 34221.
Finally, the quality of statistics of causes of death was evaluated based on the framework provided by the ninth and tenth revisions of the International Classification of Diseases (ICD-9 and ICD-10, respectively) and based on the criteria provided by experts in the field14,15,22,23,24 (http://apps.who.int/classifications/icd10/browse/2016/en). We have identified three groups of problematic cause-of-death reporting: ill-defined, unspecific and less specific causes. As ill-defined causes, we selected all of the codes from Chapter XVI of the ICD-9 (Symptoms, Signs, and Ill-Defined Conditions) and Chapter XVIII of ICD-10 (Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified), excepting those codes excluded by a recent update along with other codes for which there is a consensus in Spain (annex 3). We have included as unspecific causes, codes “.9” which do not indicate the organ affected, but instead provided only the affected system - along with external causes of undetermined intent (without judicial evidence), in addition to other causes utilized without sufficient information (for example, “hypotension, unspecified”, ICD-10 code, I959), or causes which are long-term effects of a disease or condition. For less specific causes, we have selected “.9” codes from other unspecified sections, and those for unspecified natural causes; and for external causes, that they had explained the reason without the circumstances, such as: a) disease with a generic mention of the infectious agent (e.g. bacterial foodborne intoxication, unspecified); b) neoplasms of unspecific sites in the body areas greater than organs and/or neoplasms of uncertain or unknown behaviour; c) other imprecise diagnoses with 3-character codes, “.9” codes that have not included other causes, rather unspecified causes; d) others. We have excluded precise diagnoses that can be used in a generic form (e.g. determinate cardiac arrhythmias, peptic ulcers, etc.). However, we have included heart failure, unspecified, and arteriosclerosis (ICD-10, I509 and I709, respectively).
Annual rates were age-adjusted to the (“old”) European Standard Population and for similarity with the age profile of the Murcian and Spanish populations.
Good quality documentation was evaluated as follows: reduction in the value of indicators for faulty filling out of forms and death certification knowledge; increases in the indicators for information recovery; along with the adjusted rates for ill-defined, unspecific and less specific causes in the statistics of causes of death.
In order to evaluate forward changes into the statistics due to ill-defined, unspecific or less specific causes, we have expanded the analysis period to 1980-2015, and replicated age-adjusted-rate calculation of these causes with the data for Spain overall for comparison.
We have used the prtesti command in Stata [StataCorp. 2015. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP] to carry out the statistical analysis of the comparison of proportions. For the comparison of adjusted rates between territories, we used the Wald test, in which the figure for the contrast is calculated as the difference between the rates divided by the standard error. The bilateral significance level was set at p <0.05.

RESULTS
As regards the quality of form fulfilment, we observed that the lack of physiopathological sequence showed a marked annual decrease, with rates below 31% since 1995 (p<0.001) (figure 4). Furthermore, the inclusion of pluripathology in the initial cause of death increased up to 1996 (p<0.001), only to decrease to levels close to 4% at the end of the study period (p<0.001). Doctors’ fulfilment of DC or BB with illegible handwriting maintained a minimum level throughout the study period. The use of abbreviations or acronyms of various meanings grew from 9% to 32% in 2007 (p<0.001), only to decrease to 21% in the last year (p<0.001).
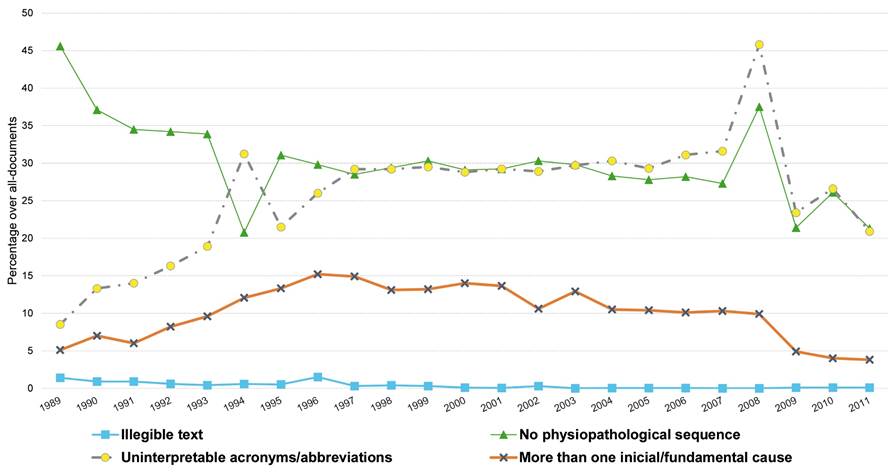
Figure 4 Formal aspects and know-how of the medical fulfillment of death causes in the Medical Death Certificate and the Statistical Birth Bulletin (lifeborns and stillborns)
The information revision regarding the causes and circumstances of the notification obtained positive (improvements) results (figure 5) with a positive trend, from a baseline of 38% to a final 93% (p<0.001). The opposite trend was found for deaths without access to information, which reached an initial and maximum of 62%, and a final and minimum proportion of 3% (p<0.001). While death causes subject to revision but later confirmed remained in an annual range between 2% and 17% (p>0.4), and frequently below 11%.

Figure 5 Information revision and recovery results of medical and judicial certification of death causes and circumstances
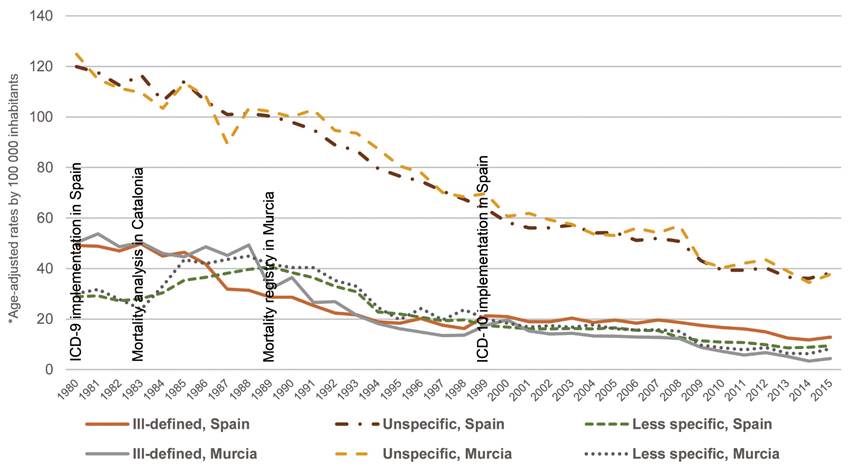
Among the quality indicators of statistics of death causes, the largest decrease was registered in age-adjusted rates by unspecific causes, followed by ill-defined causes, which crossed over with less specific causes in some years. At the end of the study, ill-defined causes registered the lowest rates (figure 6). Unspecific causes went from having higher rates in Murcia than for overall Spain (124.8 deaths per 100 000 residents in Murcia against 120.0), to being a little lower in Spain in 2011 (42.1 against 39.3, p=0.55). Ill-defined causes obtained similar rates in both territories (50.3 versus 49.2, p=0.65), with Murcia achieving the largest final decrease (16.1 versus 5.8, p=0.0001). Less specific causes started at similar levels (30.2 and 28.9, p<0.49) and showed less pronounced changes, with Murcia obtaining the lowest rates in the end (7.9 against 10.7 for Spain, p<0.0001).
DISCUSSION
The quality of medical certification of death certificates improved as regards physiopathological sequences for cause of death, and in lower rates of pluripathology being declared as the initial cause. The regulated revision of documents and recovery of data optimized the information provided, with positive results regarding access to information, and confirmation and modification of the circumstances of causes of death. At the same time, statistics of causes of death evidenced a significant and greater decrease in ill-defined causes in Murcia in comparison with Spain. The decrease has been less notable for less specific causes in Murcia, but comparable to the Spanish average for unspecific causes.
The fulfilment improvement in physiopathological sequences on medical certification can be attributed, in part, to medical training, given on the degree and postgraduate studies in Medicine and which we continue to deliver almost annually4 (www.murciasalud.es/certifica), which is provided within the training of specialist doctors (Resident Medical Interns)26. Moreover, the reduction in illegible handwriting can be put down to this prior training, and to the skill of the nurses doing the coding.
It is well known that other autonomous communities carried out and are carrying out improvement activities, which explains in part the reduction in mortality rates for ill-defined, unspecific and less specific causes across Spain. It is notable, however, that regional differences for these groups of causes improved in favour of the autonomous community of Murcia.
We are now in a mixed situation. A significant proportion of cause-of-death notifications still on paper, but with automatic processing now fully established. However, it should be possible: to evaluate the quality of OCR recognition of paper-based hand-written causes of death; to standardize death cause texts in data processing; and - while available - direct help to the medical fulfilment of the digital documents with defined diagnoses27. In Spain, there are different processes for the BB and JDB, pending the adaptation of their formats to the Iris coding system17. The processing of the BB and JDB should also be subject to evaluation of optical character recognition (OCR) quality, and normalization via the Neutral Judicial Point (the judicial website of the Spanish Statistical Office) or their entry into Iris.
It has already been demonstrated that the quality of judicial death reporting in Spain could be improved. There are several complementary interventions available, such as: cross-validation with medico-legal information13, or the adding of the recovered information from final veredict at the end of the statistical year. The information gathered by the Institute of Legal Medicine and Forensic Sciences could improve the statistical information28, in addition to the improvements that could be made by the judicial courts as regards indeterminate causes through the judicial inquest and post-mortem examinations29. It is for this reason that forensic doctors or their institution of Legal Medicine could be assigned a hierarchical role for notification/supervision on the causes and circumstances in the JDB notification over and above anatomo-histopathological diagnoses. It would be beneficial to provide specific accredited training during the medical specialization - as much in forensic medicine and pathology, for the characteristics already noted, as in other specializations - to improve the quality of death certification.
In the updated ICD-10 instruction manual from 2016, heart failure (I50) and hypotension, unspecified (I959) were included among the ill-defined causes. We understand that heart failure is a well-established syndromic diagnosis, as much in its congestive heart failure forms as those of the left ventricle. We have not included Sudden Infant Death Syndrome among the list of ill-defined causes, as it is the object of the judicial investigation in some autonomous communities. At the same time, we have not included either, acute renal failure or chronic kidney disease or failure, which are diagnoses identifiable in any medicine textbook14,15.
Our study is not totally comparable to previous studies carried out in Spain because it used diverse groupings of ICD-9 codes, although it were referred to similar concepts. In one of the articles, it is noted that the Murcia region presented a significant excess of ill-defined and less specific causes in relation to the Spanish average7, a datum which agree with the findings of our study along the period between 1985-1993 for less specific causes.
We have noted that the quality of statistics of causes of death was situated in a high group according to the WHO15, without having made available up-to-date information regarding the deaths completeness and death causes validity, representative of Spain7,9,10. Therefore, we could recommend the implementation of quality programmes for the improvement notification on statistics of causes of death. On this matter, indicators should be established for: form completion and knowledge regarding medical and judicial death certification; regulated information revision and recovery of information regarding the causes and circumstances of the death; as well as periodic monitoring of ill-defined, unspecific or less specific causes in mortality statistics.
ACKNOWLEDGEMENTS
We would especially like to thank Anna Puigdefàbregas, Miguel Ruiz-Ramos, Jesús Carrillo, the Regional Centre for Statistics of Murcia, and the reviewers of the manuscript. Besides, Ana B. Maldonado (Medical Resident in Preventive Medicine and Public Health) and Humberto Gómez. Finally, our thanks go to Carmen López for supervision of the Spanish language version of this manuscript.
REFERENCES
1. Cirera L, Segura A. Documentos médicos de la defunción actualizados: certificado médico de defunción y boletín estadístico de parto. Aten Primaria; 2010; 42(8):431-437. DOI: 10.1016/j. [ Links ]
2. Ley 20/2011, del Registro Civil. Gobierno de España. BOE núm. 175, de 22 de julio de 2011. [ Links ]
3. Segura A. Anàlisi de la mortalitat a Catalunya, 1983. Generalitat de Catalunya. Departament de Sanitat i Seguretat Social. Generalitat de Catalunya; 1985. [ Links ]
4. Cirera L, Martínez C, Contreras J, Navarro C. Aprendizaje y satisfacción de pre y postgrado de las causas de las causas de defunción, 1992-1996. Rev Esp Salud Públ. 1998; 72:185-195. [ Links ]
5. Ruiz-Ramos M, Cortés M. Evaluación de seminarios sobre criterios internacionales de la certificación médica de las causas de defunción. Atención Primaria 1996; 18(6): 324-6. Disponible en: http://www.elsevier.es/es-revista-atencion-primaria-27-articulo-evaluacion-seminarios-sobre-criterios-internacionales-14364. Acceso: 12/05/2016. [ Links ]
6. Navarro C, y Olivares (editores). Notas metodológicas. En: Estadísticas Básicas de Mortalidad de la Región de Murcia. Varios años. Disponible en: http://econet.carm.es/web/crem/inicio/-/crem/publica/catalogo_est_demografia4.html. Acceso: 2/05/2017. [ Links ]
7. Regidor E, Rodríguez C, Ronda E, Gutiérrez JL, Redondo JL. La calidad de la causa básica de muerte en el Boletín Estadístico de Mortalidad. España, 1985. Gac Sanit 1993; 7(34):12-20. [ Links ]
8. Segura A. La qualitat de les estadístiques de mortalitat. Tesis doctoral. Bellaterra: Universidad Autónoma de Barcelona; 1986. [ Links ]
9. García Benavides F. Estudio de la exactitud de las causas de muerte como índice de fiabilidad de las estadísticas de mortalidad. Tesis doctoral. Universidad de Alicante; 1986. [ Links ]
10. García J, Cirera L, Tomo M, Martínez C, Contreras J, Navarro C. Utilidad del boletín estadístico de defunción para la identificación de muertes extrahospitalarias en un registro poblacional de infartos agudos de miocardio. Rev Española Cardiol. 2001; 54(9):1041-1047. DOI: 10.1016/S0300-8932(01)76450-0. [ Links ]
11. Cirera L, Navarro C. Validez de la certificación de la muerte por cáncer en la Comunidad de Murcia. Oncol. 2002; 25(5):264-272. [ Links ]
12. Mathers CD, Ma Fat D, Inoue M, Rao C, Lopez AD. Counting the dead and what they died from: an assessment of the global status of cause of death data. Bull World Health Organ 2004; 83(3):171-7c. DOI: 10.1590/S0042-96862005000300009. [ Links ]
13. Gotsens M, Marí-Dell Olmo M, Rodríguez-Sanz M, Matos D, Espelt A, Peréz G, et al. Validation of the underlying cause of death in medicolegal deaths. Rev Esp Salud Publica 2011; 85(2):163-74 [in Spanish]. DOI: 10.1590/S1135-57272011000200005. [ Links ]
14. Ribotta BS, Escanés G. Códigos "poco útiles" en los registros de defunción en Argentina, Chile, Colombia y México (2000-2011). Med Salud y Soc 2014; 5(1):4-17. [ Links ]
15. World Health Organization. Health Statistics 2017. Monitoring health for the sustainable development goals. Completeness (%) and quality of cause-of-death data. WHO. World Health Statistics; 2017. Pp. 7 and 84. Disponible en: http://apps.who.int/iris/bitstream/10665/255336/1/9789241565486-eng.pdf?ua=1 [ Links ]
16. Foreman KJ, Naghavi M, Ezzati M. Improving the usefulness of US mortality data: new methods for reclassification of underlying cause of death. Popul Health Metr. 2016; 14:1-9. DOI: 10.1186/s12963-016-0082-4. [ Links ]
17. Instituto Nacional de Estadística. Iris: Codificador automático internacional de Causas de muerte. Consulta: 04/07/2016. Disponible en: http://www.ine.es/ss/Satellite?L=es_ES&c=INEDocTrabajo_C&cid=1259949358002&p=1254735116586&pagename=ProductosYServicios%2FPYSLayout [ Links ]
18. Instituto Nacional de Estadística. Informe metodológico estandarizado. Recogida de datos. Estadística de Defunciones según la Causa de Muerte. Acceso: 24/11/2016. Disponible en: http://www.ine.es/dynt3/metadatos/es/RespuestaDatos.html?oe=30417. [ Links ]
19. Instrucción 11.025, de 9 de octubre de 2015, de la Dirección General de los Registros y del Notariado, sobre comunicación electrónica de nacimientos desde centros sanitarios. Gobierno de España. BOE núm. 246, de 14 de octubre de 2015. [ Links ]
20. Consejería de Sanidad. Memoria [Años 1989-2011]. Consejería de Sanidad. Región de Murcia. España. Disponible en: http://www.murciasalud.es. Acceso: 11/11/2016. [ Links ]
21. Cirera L, Martínez C, Salmerón D, Navarro C. Proceso de codificación y detección de errores. Material y Métodos. Estadísticas básicas de mortalidad en la Región de Murcia (años 1989-2011). Disponibles en: http://www.murciasalud.es/publicaciones.php?op=mostrar&tipo=series&id=12&idsec=88. Acceso: 12/11/2016. [ Links ]
22. Organización Mundial de la Salud. Clasificación Estadística Internacional de Enfermedades y Problemas relacionados con la Salud, Novena Revisión (CIE-9). Ginebra: OPS/OMS; 1978. [ Links ]
23. Socialstyrelsen. Konverteringstabeller. [in Swedish]. Disponible en: http://www.socialstyrelsen.se/klassificeringochkoder/diagnoskodericd-10/konverteringstabeller. Acceso: 11/11/2016. [ Links ]
24. Cirera L. Instauración y evaluación de la CIE-10-mortalidad en España. Salud(i)Ciencia 2009; 17(3): Disponible en: http://www.siicsalud.com/buceador/buceadorsimple.php?todas=cirera&version=breve&lineas=20&version2=breve&lineas=20&I32.x=0&I32.y=0. Acceso: 11/11/2016. [ Links ]
25. Organización Mundial de la Salud. Clasificación Estadística Internacional de Enfermedades y Problemas relacionados con la Salud, Décima Revisión (CIE-10). Annex 7.3. Vol. 2. Ginebra: OMS; 2016. http://apps.who.int/classifications/icd10/browse/Content/statichtml/ICD10Volume2_en_2016.pdf?ua=1&ua=1. [ Links ]
26. Curso para MIR en formación sobre certificación de la defunción. Programa transversal y complementario del residente de la Región de Murcia. Disponible en: http://www.murciasalud.es/idea/course/category.php?id=70. Acceso: 11/05/2016 [ Links ]
27. Cirera L. Primer bienio de estadísticas de mortalidad con el codificador automático de causas de muerte Iris. Gac Sant. 2017. http://dx.doi.org/10.1016/j.gaceta.2016.11.009 [ Links ]
28. Puigdefabregas A, Freitas A, Gispert R, Castella J, Vidal C, Mellado J, et al. Deaths with medicolegal intervention and its impact on the cause-of-death statistics in Catalonia, Spain. [in Spanish]. Rev Esp Med Legal. 2017; 43: 13-19. [ Links ]
29. Salmeron D, Cirera L, Ballesta M, Navarro F. Time trends and geographical variations in mortality due to suicide and causes of undetermined intent in Spain, 1991-2008. J Public Health (Oxf). 2013;35(2):237-245. DOI: 10.1093/pubmed/fds103. [ Links ]
Suggested citation:Cirera L, Salmerón D, Martínez C, Bañón RM, Navarro C. More than a decade of improvement in medical and judicial certification in the statistics of causes of death. Rev Esp Salud Pública.2018;92: June 6 e201806031.
Annex 1
Indicators of the quality programme in fulfilment of the medical and judicial death certification
Indicators of formal aspects
Handwriting: Handwriting illegible for the nurse(s) and doctor of the registry. Applied to the Medical Death Certificate /Statistical Death Bulletin (DC) and the Statistical Birth Bulletin (BB) for stillborn or for liveborn babies who die within their first day of life.
Abbreviations and/or acronyms: Abbreviations and/or acronyms of various meanings that alter the selection of the underlying cause of death (that which is published in the statistics). Applied to DC and BB.
Signature: Lack of doctor’s signature and/or registration number in the case of the DC or BB, for the Judicial Statistical Death Bulletin (JDB) without judicial report, but with reference to the court and / or proceedings number, summary, or preliminary report.
Indicators of certification knowledge (know-how)
Sequence: Lack of physiopathological sequence when the immediate cause is not reported, nor the following characteristics seen in Figure 3. It is accepted as a proper sequence when a hyphen or other item appears in Antecedent and/or Initial/Fundamental* causes, always including filling in /completing the preceding cause sections.
More than one cause: If the form is completed with more than one pathology in the section for initial or fundamental cause, or on the preceding lines. Applied to both DC and BB.
* Initial/Fundamental are synonym in Spain and the label of the cause section for the disease or condition directly leading to death.
Annex 2
Indicators for the quality programme on the information revision and recovery of medical and judicial death certification
Indicators for the activation of the revision
Ill-defined death causes: all of the causes in XVI Section of the Ninth Revision of the International Classification of Diseases (ICD9) or from XVIII Chapter of ICD10.
-
Medical Death Certificate / Statistical Death Bulletin (DC), the Statistical Birth Bulletin (BB), or Judicial Statistical Death Bulletin (JDB):
Infrequent death causes or relevant for the health administration in the DC, JDB or BB with criteria for a phone call in order to improve the information regarding the underlying cause of death - that is published in the statistics. These underlying causes are called “warnings” in the terminology of the Spanish Statistical Institute.
Inconsistency of cause with sex / age.
Indicators of results
Positive (improvement): If the code for the underlying cause of death is changed to a non-ill-defined code.
Confirmation: If upon consulting as regards an ill-defined, infrequent or relevant code to the health administration, the code is kept as is following recovery of the information.
Without access: If the person consulted does not remember, does not collaborate, lacks more available information or cannot be consulted (cannot be located, has no telephone, has no medical registration number, or only answering machine, a change of address, etc.).
Others: None of the above (e.g. delays in obtaining judicial information, or the certifying medic being signed-off sick).
Annex 3
Codes from the International Classification of Diseases assigned to ill-defined, unspecific, and less specific causes of death
Unspecific causes
ICD-9: 1369, 1398, 1499, 1599, 1659, 1849, 1879, 1899, 1929, 1949, 195, 199, 2219, 2299, 2239, 2249, 2319, 2329, 2339, 2349, 2389, 2390, 2391, 2392, 2399, 2599, 2699, 2779, 2799, 2899, 3159, 3499, 3799, 3889, 4589, 4599, 5089, 5199, 5999, 6089, 6259, 6299, 6469, 6559, 6569, 6599, 6699, 6749, 7099, 7399, 7599, 7799, E980-E989.
ICD-10: B89, B949, B99, C269, C399, C579, C729, C759, C689, C76, C80, C969, D024, D099, D289, D299, D309, D369, D379, D386, D399, D409, D419, D449, D489, D759, D899, E349, E619, E639, E649, E889, E899, F89, F99, G969, G98, H579, H599, H939, H959, I879, I959, I99, J709, J989, K919, K929, L29, L989, M899, M949, M999, N399, N509, N949, N999, O269, O359, O369, O759, O909, O95, O96, O97, P95, P968, P969, Q899, Y10-Y34, Y872, Y899.
Less specific causes
ICD-9: 009, 0269, 0279, 0419, 0799, 1349, 2119, 2129, 2139, 2159, 2169, 2259, 2279, 2859, 2879, 3009, 3129, 3369, 3379, 3469, 3483, 3489, 3589, 3599, 3609, 3689, 4279, 4289, 4299, 4409, 4579, 5369, 5649, 5689, 5699, 586, 588, 589, 5939, 6119, 6149, 6259, 6479, 6559, 6569, 6599, 6869, 6989, 7019, 7109, 7169, 7199, 7299, 7329, 7331, 7369, 7389, 7429, 7479, 7489, 7519, 7529, 7539, 7559, 7569, 7579, 7589, 7597, 7609, 7619, 7639, 764, 765, 766, 7679, 7684, 7689, 7708, 7709, 7729,7759, 7769, 7779, 7789, E819, E9139, E9289, E9589, E9689.
ICD-10: A259, A289, A499, A64, B349, B889, D139, D144, D169, D219, D239, D339, D359, D439, D649, D699, E319, E619, G249, G319, G439, G589, G629, G64, G709, G719, G729, G909, G934, G939, G959, H449, H539, I499, I509, I519, I709, I899, K30, K599, K639, K669, L089, L309, L909, M139, M199, M219, M259, M359, M629, M799, M844, M939, M959, M969, N139, N19, N26, N27, N289, N649, N739, O989, P009, P019, P039, P05, P07, P08, P159, P209, P219, P229, P282, P283, P284, P289, P549, P619, P729, P749, P789, P839, Q079, Q289, Q349, Q459, Q529, Q559, Q639, Q649, Q749, Q799, Q829, Q849, Q897, Q999, V892, V99, W49, W64, W84, W99, X59, X84, Y09.
Own elaboration based on the ICD-10 WHO update, 2017.
Received: October 23, 2017; Accepted: March 21, 2018
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
