










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Sanidad Penitenciaria
versión On-line ISSN 2013-6463versión impresa ISSN 1575-0620
Rev. esp. sanid. penit. vol.19 no.1 Barcelona 2017
Fibromuscular dysplasia: unusual cause of abdominal pain
Displasia fibromuscular: causa infrecuente de dolor abdominal
M. Alonso-Alcañiz, J.M. Antolín, J.R. Rebolledo and C. Muñoz-Montano
Healthcare Department of Ocaña I
ABSTRACT
Spontaneous dissection of the renal artery is a rare phenomenon, and is more common amongst men. It is not a frequent cause of abdominal pain2, which is why diagnosis is often late.
The case under study is a 45 year old patient that presented sudden pain in the left renal fossa of 12 hours evolution, with no findings from the basic laboratory tests (lab testing, urinary sediment and ultrasound), an abdominal CAT was therefore carried out, which showed areas of renal infarction, as well as an emergency arteriogram, which gave findings of a possible Fibromuscular Dysplasia of the left intrarenal artery as the first diagnostic probability with a partially thrombosed focal dissection.
Key words: prisons; fibromuscular displasia; infarction; hypertension, renovascular; dissection; renal artery; abdominal pain; Spain.
Introduction
Spontaneous renal artery dissection (SRAD) is a rare event, more common among male patients2,3. It is an unusual cause of abdominal pain2 and thus a challenge for physicians to diagnose.
SRAD can present as a primary occurrence5,6 associated with systemic diseases such as severe atherosclerosis (most commonly)1,3,4, severe hypertension, connective tissue disease, fibromuscular dysplasia or cocaine use; or it can be secondary to severe trauma or endovascular surgery.
Clinical description
We report the case of a 45 years old smoking (20 cigarettes/day) patient with no previous record of drug use who suddenly presented with left flank pain of 12 hours evolution, which remained unchanged by position and responded partially to standard analgesics, with no accompanying fever or urinary symptoms. There was no record of previous trauma.
Upon arrival to the ER department his blood pressure (BP) was 148/96mmHg and his blood tests revealed high LDH levels, slight elevation of GOT and GPT and elevated white blood cell count. The rest of analytical parameters as well as his urinary sediment presented no alterations.
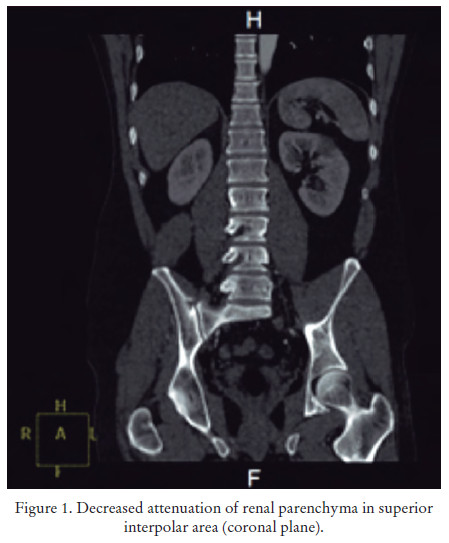
Abdominal echography was performed with no significant alterations due to which it was decided to perform an abdominal CT scan. This test showed focal areas of decreased uptake in the left renal parenchyma, compatible with ischemia/ infarction, as well as in the anterior-inferior region and the middle and superior-exterior parenchyma. The anterior branch of the left main renal artery presented an impaired repletion which caused a significant reduction of its diameter with apparent patency of distal branches; proximal to the repletion defect there seemed to be a double-lumen, thus the results were compatible with partially thrombosed focal dissection.
Urgent angiography revealed the presence of Fibromuscular Dysplasia in the left renal artery without indication of endovascular treatment due to the duration of the symptoms (he had presented flank pain for 24 hours now), due to which conservative management was decided.


Evolution
The patient was successively assessed by the departments of Nephrology and Urology. His BP was 122-130/80-86, he presented preserved renal function and negative proteinuria. Hence he was discharged and recommended to pursue consultation and monitoring by his Family Doctor.
Final note
The most common presentation of Fibromuscular Dysplasia is Hypertension1. Spontaneous renal artery dissection (SRAD) associated with Fibromuscular dysplasia is a rare entity whose clinical presentation usually suggests nephrolithiasis2 and requires the performance of conventional angiography or computed tomography (CT) angiography2, thus its diagnosis is usually delayed.
References
1. Tovar JL. Hipertensión arterial secundaria a displasia fibromuscular de la arteria renal. Nefroplus. 2010; 3(3): 27-34. [ Links ]
2. Borja F, Gonzalez R, Ursu M, Varela C, Vukusich A. Rev Méd Chile. 2008; 136: 1183-7. [ Links ]
3. Bodoira M, Kemps J, Caldiroli S, Marchetti G, Porley C, Almirón N, et al. Disección espontánea de arteria renal: reporte de un caso y revisión de la literatura. Revista Argentina de Cardioangiología. 2012; 3(01): 0043-5. [ Links ]
4. Cruzado-Vega L, Hernández-Jaras J, Martín-Abad L, Alonso-Gorrea M, Miralles-Hernández M. Tratamiento de hipertensión vasculorrenal por displasia fibromuscular de arteria renal con autotrasplante renal. Nefrología. 2013; 33(2). [ Links ]
5. Medline Plus. Hipertensión renovascular. En: www.nlm.nih.gov. [ Links ]
6. Valdivieso A, Bergoeing M, Vidal H, Heredia A, Turillas P. Disección espontanea de arterias renales (DEAR) complicada con infarto renal. Reporte de tres casos. XXXII Congreso Sociedades Chilenas de Nefrología e Hipertensión. Trabajos. Noviembre 2015. [ Links ]
![]() Correspondence:
Correspondence:
M Alonso Alcañiz
Healthcare Department of Ocaña I
Calle Mártires de Ocaña 4.
45300-Ocaña. Toledo (Spain)
Text received: 02/06/2016
Text accepted: 12/06/2016

