










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Diabetes mellitus (DM) is one of the four noncommunicable diseases selected by world leaders for intervention on a high-priority footing1. It is also a major health problem because of its high prevalence and the financial burden it implies for national health systems2-3, and also because of the high morbidity and mortality levels caused by macrovascular and microvascular complications1,4-5.
Clinically speaking, the disease is marked by hyperglycaemia, brought about by changes in insulin secretion. The autoimmune destruction of pancreatic beta-cells is described as type 1 DM (DM1), while a progressive resistance to the peripheral action of insulin, with or without an associated deficit in secretion, is called type 2 (DM2)6 and is usually associated with increasing age, obesity, a family background of diabetes, groups belonging to ethnic and racial minorities, lack of physical activity, and chronic diseases such as high blood pressure and dyslipidemia5,7-8. In the past, DM2 was considered to be a disease of elderly adults, but it is also present in children, adolescents and young adults1,9-11.
According to the World Health Organisation (WHO), there were 422 million people over 18 years of age suffering from diabetes worldwide in 2014, which is a prevalence of 8.5%1. It is estimated that it shall affect 439 million adults (20-79 years of age) in 2030, increasing by 69% in developing countries and 20% in developed ones12. In recent decades, key epidemiological factors have been observed in the increase of diabetes, such as population growth, longer life expectancy, increased prevalence in each age group, obesity and unhealthy lifestyles1.
In line with WHO policies, health promotion and prevention programs are being implemented in Catalonia from the moment of entry into prison, and measures have been taken for early detection, appropriate control and management of DM13.
Controlling blood sugar levels has been shown to reduce microvascular and macrovascular complications, mostly in the case of heart attacks7. However, optimal management requires a multi-factor approach3,7,14-17 that not only includes controls of blood sugar levels but also of other risk factors18. Hence, glycosylated haemoglobin, controls of dyslipidemia and blood pressure, along with the prevention of smoking and obesity are the five pillars used to control DM3,7,19. The control objectives are: to obtain an HbA1c under 7%, pre-prandial blood sugar of 90-130 mg/dL and post-prandial blood sugar at 2 h under 180 mg/dL. The total cholesterol values are ideal if they are less than 200 mg/dL and if the blood pressure value is under 140/90 mmHg. Other objectives are not smoking and an adequate body mass index (BMI kg/m2)3,7. There are a large number of national and international clinical guides that promote education for persons with DM5,20, which set out to help patients and family members to increase awareness, technical skills and the right attitudes towards the effective control of diabetes, bearing in mind the needs, beliefs and life experiences of each person5. The phases of the education process should be based on achieving optimal metabolic control, preventing complications, creating good adherence to treatment, enabling the patient to acquire a positive attitude about the disease, and increasing or maintaining quality of life by changing lifestyles (avoid a sedentary lifestyle, follow specific nutritional requirements and do aerobic and resistance exercise)20-21.
Despite the importance of controlling and managing this disease, there is no published data in Catalonia about the prevalence of DM in the prison population, and what level of control there may be in prisons is unknown. This study was designed to shed light on these unknowns, and sets out to determine the prevalence of diagnosed diabetes and know more about the level of control of the disease.
MATERIALS AND METHODS
This is a descriptive, transversal study designed to know more about the prevalence of DD in the Catalonian prison population. The study was carried out in four randomly selected men’s prisons in Catalonia: three in Barcelona (CP d’Homes; CP Quatre Camins, in La Roca del Vallés; and CP Brians 2, in Sant Esteve Sesrovires; and one in Lleida (CP Ponent). The consultation period consisted of the months of April and May 2016. The patient’s clinical history was used as a source of information (primary health care clinic station, eCAP), taken from the Catalonian Health Institute (Instituto Catalán de la Salud) along with data obtained from a guided interview and an ad hoc designed questionnaire.
Sampling method
Purposive sampling of the interned prison population was carried out (n=4.307) in the participating prisons, without distinguishing between preventive or sentenced inmates with a diagnosis of type 1 or type 2 DM.
Variables studied
The following variables were collected and analysed: a) socio-demographic variables (gender, current age, age at the time of diagnosis, place of diagnosis, country of origin, educational level); b) clinical variables: type of DM, HbA1c, pharmacological treatment, metabolic syndrome: high blood pressure, high blood sugar, increased triglycerides, low level of HDL cholesterol and increase in abdominal circumference, BMI (kg/m2) with staging of normal weight (18-24.9), overweight (25-29.9) and obesity (≥30), drug use, infection from human immunodeficiency virus (HIV) and/or hepatitis C virus (HCV), and other comorbidities; c) other variables linked to: knowledge of how to act in situations of high and/or low blood sugar levels and participation in educational activities.
Information gathering technique
An ad hoc guided interview was prepared to collect data, which included the variables studied and which was previously reviewed and corrected by experts in diabetes. The interviews were conducted by nursing professionals of the centres that participated in the study. Patients were informed that they were going to be included, and they were asked to give their informed consent to participate and to use the data, thereby ensuring that the process was voluntary and anonymous. Administrative authorisation was requested from the medical management department of the prison where the research was going to take place.
Statistical analysis
The descriptive data is presented as absolute numbers, percentages and averages, with their corresponding standard deviation (SD). The prevalence of DD was calculated with an confidence interval (CI) at 95%. Control of the disease was considered to be ideal if Hb1Ac was lower than 7%, and high risk if Hb1Ac was over 9%5. A bivariate analysis was carried out to know more about the variables associated with optimal control of DM, and a multivariate analysis using a logistic regression model was performed on variables that presented statistical significance (p <0.05). The statistical program used was the SPSS v.21.0.
RESULTS
4,307 patients were analysed, 24.7% of whom were in preventive custody and 70.3% were serving sentence, with a mean age of 50.2 (SD: +/-6.3 years; range: 26-84). None of the inmates interviewed refused to participate, and there were no losses in the two months following application.
65.2% were Spanish; 18.3%, North African; 9.9%, Latin American; while the others were from Syria, Pakistan, Nigeria, Gambia, Guinea and Kosovo. As regards the educational level: 35.5% of those surveyed had not completed primary education; 35.5% had completed primary education; 26.8% had completed secondary school; 8.6% had passed the secondary school certificate exam; 9.7% had completed vocational training; 8.6% had completed university studies and 10.8% did not go to school at all. Their employment situation when entering prison was as follows: 20.4% said they were studying; 52.7% were working and 26.9%, were unemployed. Just 18.3% of the cases studied had a normal weight; 37.8% were overweight and 41.9%, were obese. The descriptive characteristics are presented in Table 1.
Table 1. Descriptive characteristics of inmates with diagnosed diabetes in prison
| Prevalence of diabetes (DM) diagnosed in prison (N=4.307) | 2.16% (n=93) | ||
|---|---|---|---|
| Type of diabetes | Diabetes type 1 23.7% | Diabetes type 2 76.3% | |
| Age | 42.4 ± 6.3 years | 52.6 ± 7.1 years | p <0.001 |
| Age diagnosed with DM | 25.2 ± 3.9 years | 44.1 ± 8.7 years | p <0.001 |
| Weight | 76.4 ± 5.1 kg | 87.1 ± 8 kg | p=0.02 |
| Drug user | 100% | 83.1% | p=0.03 |
| Knowledge about high blood sugar | 63.6% | 72.7% | p=0.05 |
| Knowledge about low blood sugar | 40.8% | 45.1% | p=0.02 |
93 inmates with DD were detected (prevalence of 2.16%; CI: 0.87-3.71), 23.7% with DM1 and 76.3% with DM2. Almost one third of the cases (32.3%) had been diagnosed during their stay in prison, while 39.8% were diagnosed in primary health centres; 26.9%, in hospital and 1.1%, in other types of health care systems.
Inmates with diabetes type 1 were slimmer than those with type 2 (76.4 +/5.1 kg compared to 87.1 +/8 kg; p=0.02), were younger (42.4 +/6.3 years compared to 52.6 years +/7.1; p <0.001), they had been diagnosed at a younger age (25.2 +/3.9 years compared to 44.1 years +/8.7 years; p <0.001), they were more likely to consume drugs (100% compared to 83.1%; p=0.03) and said that they knew what to do in the event of high and low blood sugar levels (63.6 and 72.7% compared to 40.8 and 45.1%; p=0.05 and p=0.02, respectively) (Table 1). 22.6% of the individuals studied were receiving insulin treatment; 51.6%, were taking oral anti-diabetic drugs and 25.8% were receiving both.
52.4% of the inmates with DD had optimal control of the disease (Hb1Ac below 7%) and 20.2% had high risk control (Hb1Ac under 9%). The distribution of the control results can be seen in Figure 1. The bivariate analysis showed that the variables that were associated in a statistically significant manner to the optimal control of DM were: a) presenting DM2; b) presenting metabolic syndrome; c) receiving OAD treatment; d) participating in educational activities; and e) and knowing what to do in the event of low blood sugar according to the inmates criteria. However, the multivariate analysis only associated optimal control with OAD (p=0.003; odds ratio, OR=3.97; CI: 1.60-9.88), while it disregarded the predictive value of the other variables (Table 2).
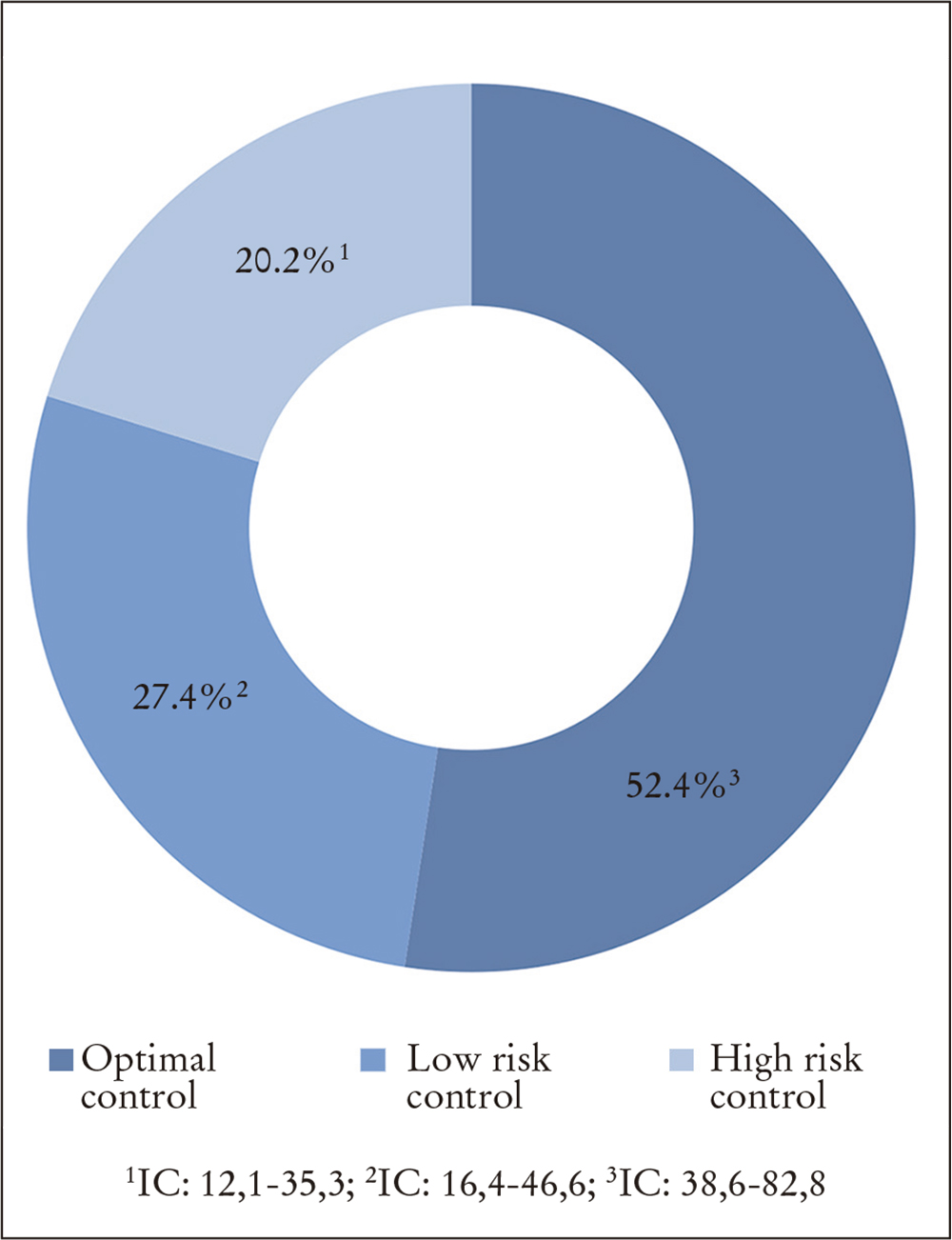
Table 2. Variables associated with optimal control of diabetes amongst inmates. Bivariate and multivariate analysis
| Bivariate analysis | Multivariate analysis |
|---|---|
| More frequent in DM2 (p=0.04) | |
| Treatment with OAD (p <0.001) | (p=0,003; OR=3,97, IC: 1,60-9,88) |
| Cases with metabolic syndrome (p=0.01) | |
| Participants in educational activities (p=0.02) | |
| Know how to act in the event of high/low blood sugar* (p=0.02) |
*Patient’s criteria.
OAD: oral anti-diabetic drugs; DM: diabetes mellitus; CI: confidence interval; OR: odds ratio.
DISCUSSION
The observed prevalence of DD amongst inmates in men’s prisons in Catalonia is 2.16% (CI: 0.87-3.71). This prevalence is much lower than the one estimated for the general public in Europe (7.3%), Spain (9.4%)1 and Catalonia, which in 2014 was 7.4% of persons over 15 years22 and, not surprisingly, is underestimated, despite the fact that in this study one third of the cases of diabetes were diagnosed while the patient was interned in prison. Such a possible underestimate of prevalence is a cause for concern, especially because many inmates present predisposing factors for diabetes, such as obesity, sedentary lifestyles, smoking, unsuitable diet and an increasing average age23-25. Many inmates also present poor social conditions, such as poverty, social exclusion and other inequalities in health terms26, which have been associated with a greater prevalence of diabetes. This is also the case in education, as there are three times as many persons with diabetes amongst those with primary or no studies as there are amongst the population with university studies22, and educational levels are generally much lower amongst inmates than amongst people outside prison.
Although many inmates present predisposing factors for DM, this pathology is more difficult to make out in such an environment25,27. As Vera et al.25 describe, the record of prevalence of chronic diseases was 19.7%, although 32.3% actually presented diagnostic criteria, but this did not appear in the clinical history. In particular, 3.7% of inmates had a prior diagnosis of diabetes, but another 1.6% presented diagnostic criteria that were not duly recorded in the clinical history.
As regards control, this study showed that only 52.4% of the inmates with DD received optimal control of the disease; and 20.2% received control defined as “high risk”. These results may be greatly affected by the profile of the estimated population, often drug dependent (100% of those who had DM1 and 83.1% of those with DM2), with few healthy habits, and also by the stay in prison, which is generally short, and which acts as an obstacle to implementing activities and imposes limits on obtaining good results. Imprisonment may also have a major effect on attitudes towards DM, since it is common for prisoners to give more value to the granting of release or other similar factors in their scale of values than to the concept of health and medical and therapeutic needs28-29. Reagan et al.30 consider that easy access to health care does not play a significant role in educating prisoners to make the necessary personal efforts to control the disease, and that the control of DM amongst prisoners is usually sub-optimal, also because inmates present limited self-care options and due to conditions in the prison environment itself, which do not favour optimal control of the disease31. This study showed that just one variable (treatment with OAD) was associated with optimal control of DM.
In the 90s, the St. Vincent Declaration underlined the urgent need to update epidemiological knowledge about diabetes in each European country to establish strategies of prevention and treatment of its complications32.
Despite the difficulties, the management of DM for such patients should similar to that used with the general public23, as should the educational process, which is essential in treatment. Lifestyle modifications take on tremendous importance in prison, because alongside the limitation of self-care23,33, there may also be less motivation to control the disease23,30. Inmates are also exposed to a number of psychosocial, physical and environmental factors that make them more vulnerable, which should be taken into account in any educational approach30.
The study shows the limitations of having been carried out solely amongst inmates in Catalonia, which may create some degree of uncertainty about the appropriateness of extrapolating the results for prisoners in the rest of Spain. However, the belief is that the socio-medical characteristics are similar in both groups, as the statistics from both prison administrations show34-35. On the other hand, a strong point of the study is that it was carried out with a large sample of patients, and this enables data to be obtained for the first time about the control of diabetes amongst prisoners in Spain. This study has confirmed that the prevalence of diabetes amongst inmates in Catalonia is low, although diagnosed diabetes is probably underestimated. Control of the disease is sub-optimal in almost half of the cases, although these results may be influenced by the short stay of many inmates, which makes control difficult, and by the profile of the persons diagnosed (many are consumers of illegal drugs, with little in the way of healthy habits). It is therefore recommended that the current diabetes programs in the prison context should be improved, and that new socio-educational and research strategies should be designed in order to increase diagnosis and optimise control of the disease.

