










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
A spontaneous pneumomediastinum is not a common condition. It is defined as the presence of air in the area of the mediastinum for no apparent reason1. It can be directly caused by a number of situations or may be associated with them. These include drug consumption (heroin, cocaine or cannabis in inhaled form), which is one of the most frequent triggering factors2, although it is not the only one, given that other highly prevalent pathologies such as chronic obstructive pulmonary disease (COPD) or asthma are also common causes3.
This condition was described by Hamman in 1939 and its pathogeny was established by Macklin in 19443.
It is a benign illness, predominant in men, self limiting and idiopathic in 25% of cases, and its incidence in the population with addiction to inhaled substances is estimated to be between 1/800 and 4/200 cases4.
CLINICAL CASE
A 17 year old male patient was committed to a young offenders centre. He has no known allergies to medication or chronic diseases. The patient’s toxic habits include:
Tobacco consumer for 3 years, with an accumulated consumption of two packages/year.
Addicted to marihuana for one year, with daily consumption of 1 g/24 h.
Habitual consumer of inhaled cocaine (crack) at weekends, without specifying amount or period of addiction to said substance.
After 48 hours in the centre, he started to suffer from a retroesternal chest pain spreading out to the left shoulder, which increased overnight, accompanied by dyspnoea at rest for one hour.
Physical examination of the patient presented: dyspnoea at rest, respiratory auscultation with normal bilateral breath sounds. In the neck, the supraclavicular area and the anterior region of the chest, crackling was present, and oxygen saturation (SatO2) ar ambient air was 94%. Cardiac auscultation presented rhythmic tones without murmurs, although intensity was somewhat diminished.
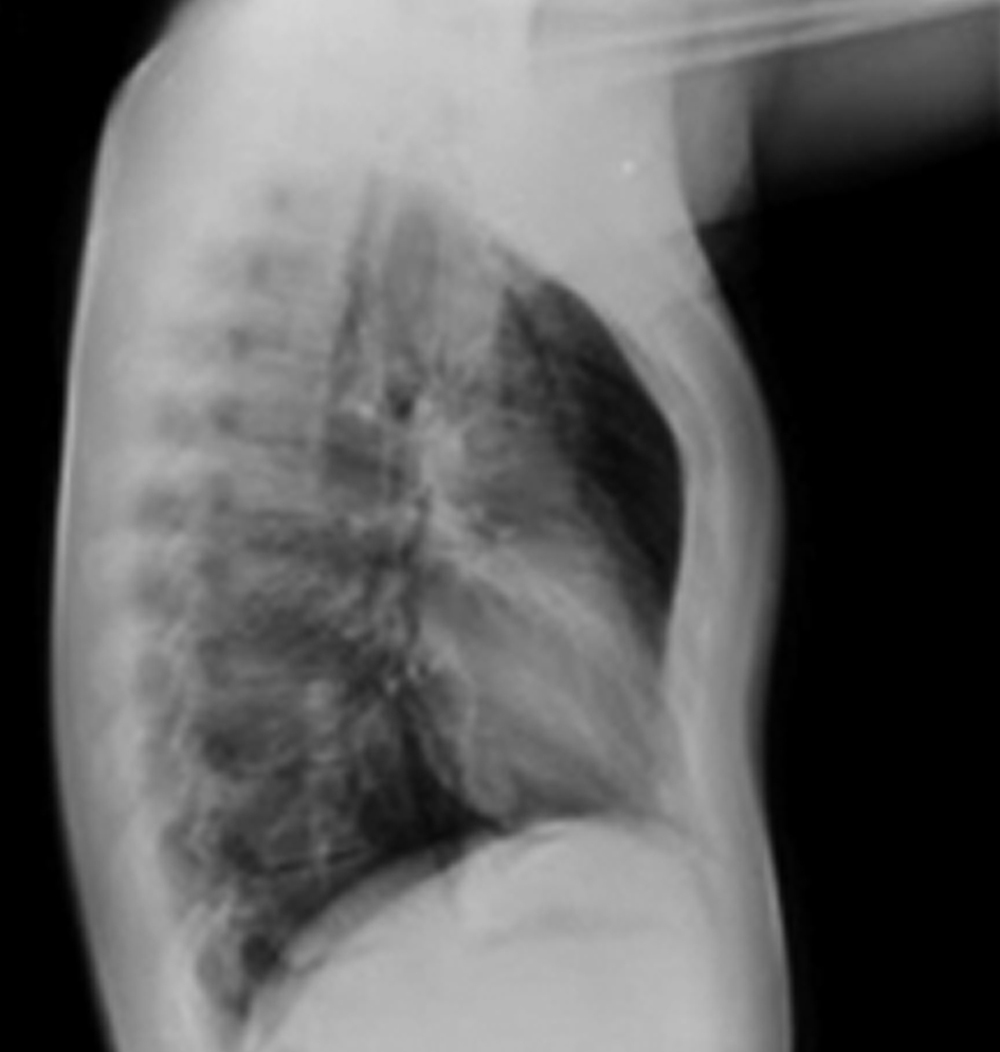
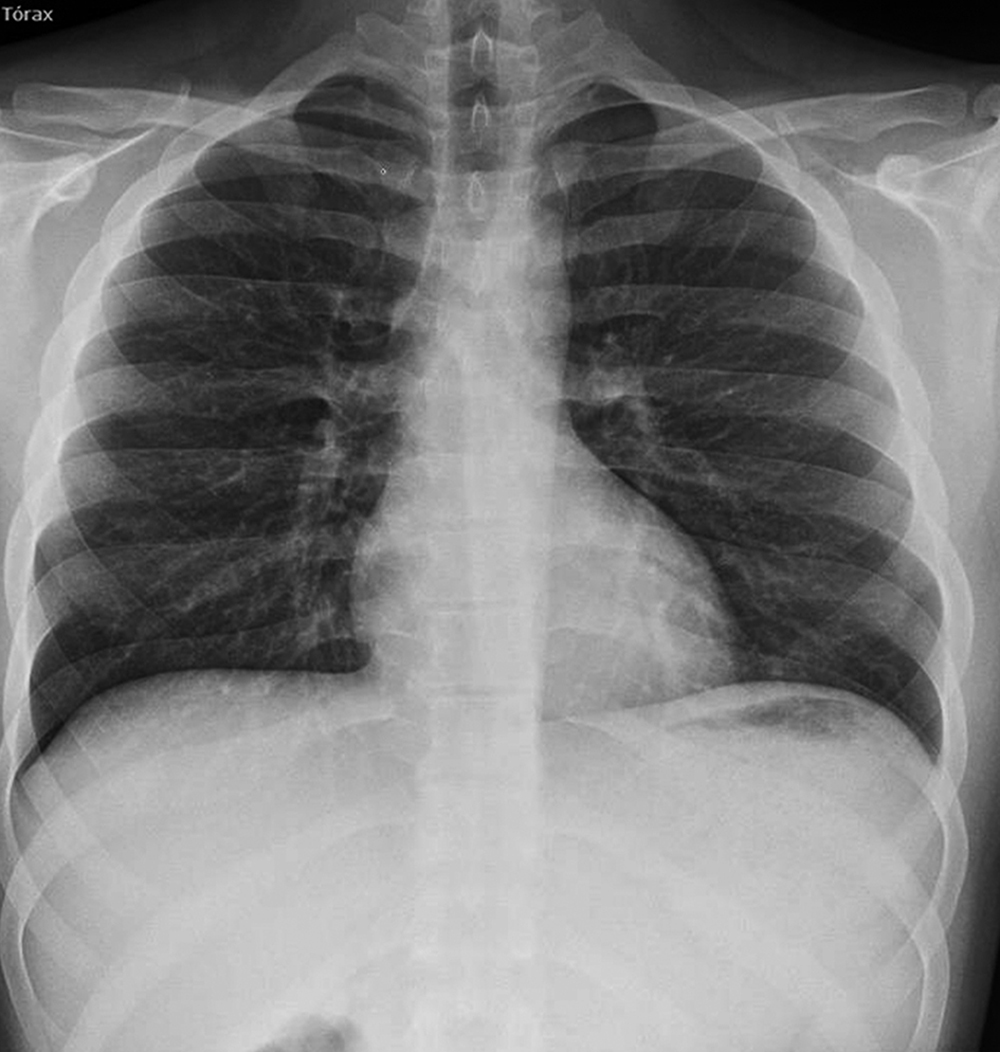
In view of the clinical signs, he was referred to the hospital accident and emergency service for an X-ray evaluation. A postero-anterior and lateral X-ray was carried out, in which air in the mediastinic area could be seen (Figures 1 and 2). A CAT scan was then carried out, which confirmed the presence of subcutaneous emphysema and air in the area of the mediastinum, with a clinical confirmation of spontaneous pneumomediastinum.

He was hospitalised under observation in A&E, with treatment consisting of oxygen therapy, analgesics and X-ray checks, and was discharged after 24 hours. A subsequent check was carried out by the respiratory medicine section and the family physician, with an X-ray check after 72 hours (Figure 3).
DISCUSSION
Spontaneous pneumomediastinum is a clinical syndrome characterised by the presence of air in the mediastinic space, without a prior trauma or surgery3 that might act as the triggering factor.
It is a pathology that presents mainly in young male patients in over 75% of cases5, between the second and third decade of life4, with an average age of 20 years5 and its course is mostly benign4.
The trigger factor of spontaneous pneumomediastinum is often unclear, since it may be associated with different causes or underlying situations, such as asthmatic crisis, chronic obstructive pulmonary disease triggered by coughing3, interstitial lung diseases4, intense efforts in sport (athletics, mountain climbing), after a forced spirometry, giving birth, hyperventilation on diabetic acidosis, vomiting, mechanical ventilation or deep inhalation of drugs: heroin, cocaine or cannabis2, due in this case to the Valsalva manoeuvre, carried out when inhaling the drug, which facilitates an alveolar rupture.
Therefore, the consumption of inhaled drugs, especially crack (cocaine base paste) is related to the appearance of spontaneous pneumomediastinum4.
The pathogenic mechanism is due to the increase of intra-alveolar pressure associated with coughing or exhaling with the glottis closed (Valsalva manoeuvre). When this exceeds the pressure of pulmonary vascularisation, there is an alveolar rupture in the base, which lets air out, leading to interstitial emphysema that fills the peribronchovascular sheaths and the interlobular septum. The pressure gradient allows the air to progress towards the hili and produce pneumomediastinum, or advance towards the pulmonary periphery and produce sub-pleural bullae and finally, pneumothorax5. Finally the air may extend towards the subcutaneous tissue of the thoracic wall and neck: subcutaneous emphysema.
The use of cocaine or its derivatives (base paste) as an inhaled drug has increased in recent years, replacing other drugs. The base paste or coca base is the cheapest, most contaminating and toxic product of cocaine. When used in inhaled form it is linked to cardiovascular and pulmonary complications, such as spontaneous pneumomediastinum, pneumothorax or both, and pneumoperitoneum. When addictive substances are sniffed or smoked, deep, forced inhalations are made, followed by Valsalva manoeuvres; this leads to a brusque increase in alveolar pressure that can cause the rupture of the alveoli next to the mediastinal pleura2. Pneumomediastinum is most often associated inhaling cocaine vapours, although in highly variable percentages, between 2.8% and 75%, according to the sources6.
The clinical form of presentation is usually sudden chest pain, and dyspnoea of variable intensity; there may be difficulty or pain in swallowing, a crackling sensation when swallowing and changes in the voice2. The determining factors in the clinical examination are usually the presence of a subcutaneous emphysema in the neck and supraclavicular area, along with auscultation in the apex of a crackling that synchronises with the heart beat (Hamman’s crunch). A chest X-ray is important and necessary, always, as shall be shown, in the posteroanterior projection, the lateral displacement of the mediastinal pleura, which shall run parallel to the mediastinal vascular structures and the cardiac silhouette; in the lateral projection, air can be seen near the pulmonary artery and in the retrosternal area. Respiratory or haemodynamic functions are not usually severely compromised, and no specific treatment is required, apart from clinical observation until the symptoms and radiological alterations are resolved1. By doing so, a differential diagnosis can be established with a spontaneous pneumothorax, which does require specific treatment5.
The diagnosis is carried out according to a compatible clinical picture and image studies. Treatment is conservative and the clinical course is usually benign1 and self-limiting7.

