










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Pregnant women undergo important anatomical, physiological and psychological changes that often challenge job demands, especially at the end of pregnancy1,2. The transition from active work to maternity license after delivery depends on a delicate balance where many factors intervene, both work and non-work related3,4. In Spain, as in other countries with a consolidated social protection benefits scheme5, two optional types of social benefits have been developed to protect pregnant women and their foetus’s health. These benefits are aimed at guaranteeing the continuity of women’s labour relationship and to cover their salary if absences from work due to health issues are needed. One of them is the sickness absence (SA) benefit, applied when the absence is due to a health problem not related to working conditions. The other one is the pregnancy occupational risk (POR) benefit, available in only a few countries6,7 and applied when absence from work is needed to prevent exposure during pregnancy to occupational risk factors that cannot be avoided by job adjustments or other measures.
Sick leave among pregnant workers is a frequently discussed issue as their SA rates are usually high8,9. According to previous studies, three out of four pregnant women had at least one episode of SA10,11,12. Other studies have tried to identify predictors of SA during pregnancy and factors that could increase the probability of returning to work after a SA episode, such as job adjustments, among others13,14. Some studies have pointed out that there are not clear medical explanations for this phenomenon15,16,17. However, health related problems such as musculoskeletal pain before18 or related to pregnancy19, overweight20, and other factors including sedentary lifestyle21, tobacco, alcohol or other drugs consumption 22,23,24, women’s "double burden"17 and attitudes towards SA25 have been associated with SA during pregnancy. Furthermore, despite SA is a specific benefit to cope ill-health non-work related, exposure to some occupational risk factors, such as heavy load handling, forced postures or high psychosocial demands, have shown a significant influence on SA in workers during pregnancy 26,27 28 29.
In line with this situation, the study about sickness absence diagnoses and occupational risk factors influences on pregnant workers disability are needed to help women to stay at work in a sustainable, healthy and productive way.
Our hypothesis was that absences due to SA are not influenced by exposure to occupational risk factors but to factors not related to work, mainly to the pregnancy itself. The aim of the present analysis was to assess the association between SA and POR benefit according to information on medical diagnoses and exposure to occupational risk factors in a cohort of pregnant healthcare workers.
Methods
Study population
We selected 367 pregnancies with at least one episode of SA from a cohort of 428 women who worked at a public university hospital, Parc de Salut Mar (PSMAR), (3,841 workers including 74.6% women, 67% of them between 21 and 50 years old) and who started a pregnancy between 2010 and 2014. Among the 61 excluded women, 56 took only the POR benefit without any SA episode and 5 worked during the whole pregnancy. For each pregnant woman, we had a daily employment status record, where they could alternate three different statuses: active work, absences due to SA and absences due to POR. There were 68 pregnant workers (18.53%) who took both POR benefit and SA during the whole pregnancy.
Assessment of health conditions and exposure to occupational risk factors and covariates
The health status of each pregnant worker in relation to her workplace was assessed by an occupational physician. Furthermore, an occupational health safety specialist carried out the workplace risk assessment collecting detailed information about job tasks, equipment, use of personal protection equipment and other existing preventive measures. This risk assessment evaluated six types of risks: biological, chemical, physical, ergonomic, psychosocial and safety. All this information was summarised and a proposal of preventive measures to avoid or reduce exposure was reported. Risks were classified into trivial, tolerable, moderate, substantial or intolerable, taking into account the probability of exposure and its potential consequences on health30. The methodology applied in this study reproduces the one used in a previously published work over the same cohort31. These risk categories were grouped into a dichotomous variable (yes/no), being "yes" when the risk assessment report had qualified them as substantial or intolerable, and "no" for moderate, tolerable or trivial. In addition, each level of risk exposure was scored from 1 to 3: trivial and tolerable risks (one); moderate (two); and substantial and intolerable (three). A global risk exposure index was developed as the sum of the scores for each risk. The risk exposure index was grouped into tertiles: 6-9 (low risk), 10-11 (medium risk) and 12-18 (high risk).
Finally, the occupational physician, in coordination with the worker’s manager, established the conclusion considering the risk assessment report, the feasibility of job adjustments and the pregnant woman individual characteristics. When there was a risk (qualified as substantial or intolerable) that could not be eliminated or adjustments be implemented, POR benefit was managed with the Occupational Health Insurance Company.
Medical diagnoses of each SA episode were collected from the medical records of each worker and coded according to ICD-10. Maternal age (≤30, 31-35, ≥36), occupation (administrative/technical support, nursing aide, nurse, physician), type of contract (temporary, permanent), working shift (morning, afternoon, split-shift, night, others), and weekly work hours (<30, 30-35, 36-40) were also recorded.
Analysis
Firstly, we calculated the frequency of SA episodes and their percentages, the total duration and median duration (MD) and cumulative days of absence (DA) for each ICD-10 major diagnostic categories and grouping specific diagnosis codes. Secondly, using sequence analysis, we identified three trajectories of SA episodes in combination with active work and POR benefit episodes, and SA major diagnostic categories. The final number of trajectories was based on the dendrogram, a tree diagram that illustrates the arrangement of the clusters produced by hierarchical clustering and informs about how data are grouped together indicating the distance between them32. For each SA trajectory we calculated the frequency, the percentage of the total accumulated days of absence (AD), and the median duration (MD) of SA and POR according to occupational risk factors, age and other workplace variables. We conducted a χ2 test to assess statistical differences among trajectories and these variables.
Finally, the crude and adjusted relative risks (RR) and their 95% confidence intervals (CI 95%) were estimated to assess the association between each trajectory and exposure to occupational risk factors using logistic regression models with a robust variance. To calculate the RR for each occupational risk factor we considered those not exposed to that same risk factor (although exposure to the other risk factors could be present) as the reference category. Furthermore, for the global risk exposure index we considered the lowest tertile value as the reference category. A sensitivity analysis to confirm the relationship between exposure to occupational ergonomic risks and belonging to SA trajectory 1 and SA trajectory 2 by occupational categories was carried out. The statistical software RStudio and STATA 13 were used.
Confidentiality of personal data was preserved by anonymization of all processed information. The research project was evaluated and approved by the ethics committee of the hospital.
Results
A total of 655 episodes of SA were recorded among the 367 included pregnant workers, amounting a total of 28,313 AD and a median duration of 19 days (Table 1). The most frequent medical diagnosis group was health problems related to pregnancy (232 episodes, 35.4%), including mainly excessive vomiting (71 episodes, 2,641 AD), risk of abortive outcome (62 episodes, 3,644 AD) and risk related to delivery (39 episodes, 2,524 AD), accounting for a total of 12,039 AD (42.5%). The second most frequent group was musculoskeletal disorders (199 episodes, 30.4%), being low back pain the leading cause (178 episodes, 9,906 AD).
Table 1. Sickness absence (SA) episodes (N=655) during pregnancy, absence days (AD) and median duration (MD) by major diagnostic categories and diagnosis codes (ICD-10) among the sample of the pregnant workers cohort with at least one SA episode (N=367), Parc de Salut Mar 2010 - 2014
| ICD-10 | DIAGNOSTIC GROUP | N | (%) | AD | (%) | MD |
|---|---|---|---|---|---|---|
| O00-O9A | PREGNANCY, CHILDBIRTH AND THE PUERPERIUM | 232 | (35.42) | 12039 | (42.52) | 22 |
| O09.0, O20.0, O20.9 | Risk of abortive outcome / haemorrhage in early pregnancy | 62 | (9.47) | 3644 | (12.87) | 25 |
| O60-O75 | Complications of labour and delivery | 39 | (5.95) | 2524 | (8.91) | 49 |
| O21 | Excessive vomiting in pregnancy | 71 | (10.84) | 2641 | (9.33) | 6 |
| O16.9, O26.5, Z39.9 | Other health problems related to pregnancy | 60 | (9.16) | 3230 | (11.41) | 18 |
| M00-M99 | DISEASES OF THE MUSCULOSKELETAL SYSTEM AND CONNECTIVE TISSUE | 199 | (30.38) | 10471 | (36.98) | 45 |
| M54.3-M54.5 | Low back pain | 178 | (27.18) | 9906 | (34.99) | 48 |
| M25.5, M53.9, M54.2, M54.9, M75.0, M77.0, M79.1 | Other health problems related to musculoskeletal system | 21 | (3.21) | 565 | (2.00) | 12 |
| J00-J99 | DISEASES OF THE RESPIRATORY SYSTEM | 70 | (10.69) | 450 | (1.59) | 3 |
| J02.9 | Acute pharyngitis | 42 | (6.41) | 286 | (1.01) | 3 |
| J03.9, J11.1, J20.9, J32.9, J45.9 | Other health problems related to respiratory system | 28 | (4.27) | 164 | (0.58) | 5 |
| R00-R99 | SYMPTOMS, SIGNS AND ABNORMAL CLINICAL ANB LABORATORY FINDINGS NECa | 58 | (8.85) | 1993 | (7.04) | 7 |
| R53.1, R53.8 | Malaise and fatigue | 17 | (2.60) | 1097 | (3.87) | 54 |
| R00.0, R10.9, R19.7, R50.9, R60.0 | Other symptoms or signs NECa | 41 | (6.26) | 896 | (3.16) | 4 |
| Z00-Z99 | FACTORS INFLUENCING HEALTH STATUS AND CONTACT WITH HEALTH SERVICESb | 24 | (3.66) | 736 | (2.60) | 7 |
| F01-F99 | MENTAL AND BEHAVIOURAL DISORDERS | 16 | (2.44) | 862 | (3.04) | 32 |
| K00-K95 | DISEASES OF THE DIGESTIVE SYSTEM | 14 | (2.14) | 261 | (0.92) | 4 |
| N00-N99 | DISEASES OF THE GENITOURINARY SYSTEM | 7 | (1.07) | 206 | (0.73) | 21 |
| - | OTHER GROUPS* | 16 | (2.44) | 527 | (1.86) | 5 |
| - | MISSING/UNREGISTERED | 19 | (2.90) | 768 | (2.71) | 28 |
| TOTAL | 655 | (100.00) | 28313 | (100.00) | 19 |
a NEC: Not Elsewhere Classified; b Includes persons encountering health services in circumstances related to reproduction; * Includes: diseases of the nervous system, infectious and parasitic diseases, circulatory system diseases, eye and adnexa diseases, injury, poisoning and other external causes, ear and mastoid diseases and skin and subcutaneous tissue diseases.
SA trajectories are shown in Figure 1. Trajectory 1 includes women with SA due to musculoskeletal medical diagnoses as the main cause of absence from work, whereas women in trajectory 2 were absent from work because of SA due to pregnancy-related disorders. POR was the main cause of work absence in those women included in trajectory 3, combined with some SA mainly due to pregnancy-related medical diagnoses.
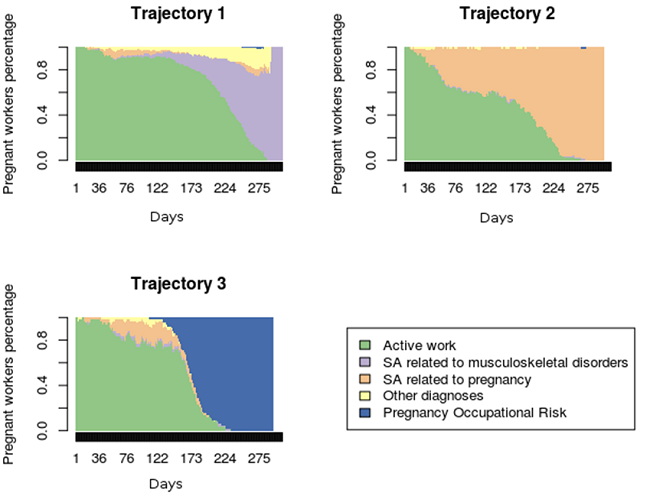
Figure 1. Sickness absence (SA) trajectories among a cohort of pregnant workers with at least one sickness absence episode during pregnancy (N=367), 2010-2014
Most women are fitted in trajectory 1, where 216 pregnant workers (58.9%) accounting for 14,942 days of SA (389 episodes) with a median duration of SA episodes of 15 days. Trajectory 2 included 92 pregnant workers (25.1%), with 12,414 days of SA (171 episodes) and a median duration of 24 days. There were only 59 women (16.1%) in trajectory 3 accounting for 6,403 days of absence due to POR (58 episodes) and only 957 days of SA (95 episodes), with a median duration of 112 and 4 days, respectively. Active work accounted for 75%, 48% and 55% of pregnancies time in trajectory 1, 2 and 3, respectively (Table 2).
Almost half of pregnancies in trajectory 3 (47.5%) had the highest score (12 to 18) of exposure to occupational risk factors. Conversely, this percentage was 22.7% and 33.7% for pregnancies in trajectories 1 and 2, respectively, and more than 40% of these women showed a low level of exposure to occupational risk factors (6 to 9). Statistically significant differences were observed between the three trajectories for the occupational risk score, occupation and working shift (Table 2).
Table 2. Description of sickness absence (SA) trajectories accordin to risk exposure, age and workplace variables among the sample of pregnant workers cohort with at least one SA episode (N=367), Parc de Salut Mar 2010 - 2014
| PREGNANCIES | TRAJECTORY 1 ACTIVE WORK / MUSCULOSKELETAL DISORDERS | TRAJECTORY 2 ACTIVE WORK / SA PREGNANCY-RELATED DIAGNOSES | TRAJECTORY 3 ACTIVE WORK / PREGNANCY OCCUPATIONAL RISK BENEFIT | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | (%) | N | (%) | EPa | ADb | MDc | N | (%) | EP | AD | MD | N | (%) | SA EP | AD SA | MD SA | PORd EP | AD POR | MD POR | pχ2 | |||||
| Risk factor exposure | |||||||||||||||||||||||||
| Biological | 167 | (45.50) | 88 | (40.74) | 142 | 6984 | 16 | 48 | (52.17) | 88 | 5911 | 29 | 28 | (47.46) | 39 | 374 | 3 | 28 | 3102 | 113 | - | ||||
| Physical | 10 | (2.72) | 5 | (2.31) | 9 | 521 | 7 | 1 | (1.09) | 1 | 204 | 204 | 4 | (6.78) | 8 | 57 | 5 | 4 | 374 | 98 | |||||
| Chemical | 25 | (6.81) | 12 | (5.56) | 15 | 588 | 15 | 9 | (9.78) | 13 | 1456 | 77 | 4 | (6.78) | 6 | 40 | 4 | 4 | 407 | 100 | |||||
| Safety | 54 | (14.71) | 19 | (8.80) | 44 | 2383 | 13 | 16 | (17.39) | 21 | 1377 | 36 | 19 | (32.20) | 27 | 181 | 3 | 19 | 2076 | 114 | |||||
| Ergonomic | 73 | (19.89) | 24 | (11.11) | 53 | 1877 | 11 | 21 | (22.83) | 43 | 2802 | 12 | 28 | (47.46) | 39 | 374 | 3 | 28 | 3102 | 113 | |||||
| Psychosocial | 95 | (25.89) | 52 | (24.07) | 85 | 3469 | 23 | 22 | (23.91) | 43 | 2768 | 24 | 21 | (35.59) | 32 | 287 | 3 | 21 | 2348 | 114 | |||||
| Non exposed | 126 | (34.33) | 94 | (43.52) | 161 | 5337 | 17 | 27 | (29.35) | 50 | 3780 | 29 | 5 | (8.47) | 11 | 114 | 3 | 4 | 510 | 132 | |||||
| Risk level exposure | |||||||||||||||||||||||||
| 6 - 9 | 161 | (43.87) | 107 | (49.54) | 189 | 6366 | 16 | 37 | (40.22) | 76 | 5252 | 15 | 15 | (25.42) | 29 | 406 | 6 | 14 | 1567 | 123 | |||||
| 10 - 11 | 98 | (26.70) | 60 | (27.78) | 111 | 4767 | 15 | 24 | (26.09) | 39 | 2999 | 33 | 16 | (27.12) | 24 | 173 | 5 | 16 | 1809 | 108 | 0.003 | ||||
| 12 - 18 | 108 | (29.43) | 49 | (22.69) | 89 | 3809 | 13 | 31 | (33.70) | 56 | 4163 | 24 | 28 | (47.46) | 42 | 378 | 4 | 28 | 3027 | 110 | |||||
| Maternal age (years) | |||||||||||||||||||||||||
| ≤ 30 | 71 | (19.35) | 42 | (19.44) | 76 | 3733 | 16 | 20 | (21.74) | 48 | 2144 | 8 | 9 | (15.25) | 15 | 220 | 7 | 9 | 958 | 107 | |||||
| 31 - 35 | 174 | (47.41) | 95 | (43.98) | 174 | 6692 | 17 | 41 | (44.57) | 77 | 5660 | 24 | 38 | (64.41) | 62 | 486 | 4 | 38 | 4243 | 114 | 0.068 | ||||
| ≥ 36 | 122 | (33.24) | 79 | (36.57) | 139 | 4517 | 13 | 31 | (33.70) | 46 | 4610 | 50 | 12 | (20.34) | 18 | 251 | 4 | 11 | 1202 | 110 | |||||
| Occupation | |||||||||||||||||||||||||
| Physician | 97 | (26.43) | 74 | (34.26) | 114 | 3263 | 21 | 18 | (19.57) | 33 | 2005 | 22 | 5 | (8.47) | 10 | 144 | 9 | 5 | 470 | 94 | |||||
| Administrative and technical support | 76 | (20.71) | 58 | (26.85) | 111 | 3426 | 14 | 16 | (17.39) | 39 | 2190 | 9 | 2 | (3.39) | 2 | 14 | 7 | 2 | 160 | 80 | 0.000 | ||||
| Nursing aide | 66 | (17.98) | 28 | (12.96) | 70 | 3298 | 12 | 19 | (20.65) | 29 | 2995 | 68 | 19 | (32.20) | 36 | 543 | 6 | 18 | 2012 | 113 | |||||
| Nurse | 128 | (34.88) | 56 | (25.93) | 94 | 4955 | 14 | 39 | (42.39) | 70 | 5224 | 29 | 33 | (55.93) | 47 | 256 | 3 | 33 | 3761 | 112 | |||||
| Type of contract | |||||||||||||||||||||||||
| Temporary | 126 | (34.33) | 83 | (38.43) | 142 | 4691 | 14 | 28 | (30.43) | 57 | 2630 | 16 | 15 | (25.42) | 25 | 299 | 6 | 14 | 1418 | 103 | 0.116 | ||||
| Permanent | 241 | (65.67) | 133 | (61.57) | 247 | 10251 | 16 | 64 | (69.57) | 114 | 5592 | 25 | 44 | (74.58) | 70 | 658 | 4 | 44 | 4985 | 114 | |||||
| Shift work | |||||||||||||||||||||||||
| Morning | 102 | (27.79) | 54 | (25.00) | 101 | 4240 | 15 | 35 | (38.04) | 57 | 4487 | 33 | 13 | (22.03) | 24 | 121 | 5 | 13 | 1453 | 108 | |||||
| Afternoon | 80 | (21.80) | 34 | (15.74) | 74 | 3476 | 9 | 23 | (25.00) | 37 | 3359 | 57 | 23 | (38.98) | 37 | 373 | 4 | 22 | 2405 | 111 | 0.000 | ||||
| Split-shift | 154 | (41.96) | 116 | (53.70) | 193 | 5963 | 21 | 25 | (27.17) | 57 | 3179 | 16 | 13 | (22.03) | 18 | 239 | 7 | 13 | 1298 | 108 | |||||
| Night and others* | 31 | (8.45) | 12 | (5.56) | 21 | 1263 | 38 | 9 | (9.78) | 20 | 1389 | 29 | 10 | (16.95) | 16 | 224 | 4 | 10 | 1247 | 120 | |||||
| Weekly work hours | |||||||||||||||||||||||||
| 36-40 | 246 | (67.03) | 147 | (68.06) | 261 | 9201 | 21 | 60 | (65.22) | 126 | 8236 | 17 | 39 | (66.10) | 63 | 611 | 3 | 39 | 4260 | 108 | |||||
| 30-35 | 59 | (16.08) | 32 | (14.81) | 65 | 2649 | 9 | 15 | (16.30) | 18 | 2018 | 58 | 12 | (20.34) | 20 | 121 | 6 | 12 | 1375 | 119 | 0.826 | ||||
| <30 | 62 | (16.89) | 37 | (17.13) | 63 | 3092 | 15 | 17 | (18.48) | 27 | 2160 | 44 | 8 | (13.56) | 12 | 225 | 8 | 7 | 768 | 116 | |||||
| Total | 367 | (100,00) | 216 | (58.86) | 389 | 14942 | 15 | 92 | (25.07) | 171 | 12414 | 24 | 59 | (16.08) | 95 | 957 | 4 | 58 | 6403 | 112 | |||||
aEP: Episodes; bAD: days of absence; cMD: median duration; dPOR: pregnancy occupational risk; *includes weekend shift.
The association between exposure to occupational risk factors and each trajectory separately is shown in Table 3. Pregnant workers in trajectory 1 had a negative association with safety and ergonomic risk factors (RR 0.56, 95% CI 0.35-0.90; RR 0.50, 95% CI 0.33-0.77, respectively), and with the highest global risk exposure index (score 12 to 18) (RR 0.68, 95% CI 0.49-0.96). Trajectory 3 was associated with safety (RR 2.75, 95% CI 1.59-4.75) and ergonomic risks (RR 3.64, 95% CI 2.18-6.06). The highest score of occupational risk factors exposure (score 12 to 18) was associated with trajectory 3 (RR 2.69, 95% CI 1.43-5.01). Trajectory 2 did not show any association with exposure to risk factors at work nor with any exposure score.
Table 3. Relative risk of the three clusters by risk exposure, age and workplace variables of the subsample of workers with at least one NWSA episode (N=367) of the pregnant workers cohort (N= 428), Parc de Salut Mar 2010 - 2014
| TRAJECTORY 1 ACTIVE WORK / MUSCULOSKELETAL DISORDERS | TRAJECTORY 2 ACTIVE WORK / SA PREGNANCY-RELATED | TRAJECTORY 3 ACTIVE WORK / PREGNANCY OCCUPATIONAL RISK BENEFIT | |||||||
|---|---|---|---|---|---|---|---|---|---|
| cRRa | (CI 95%)b | cRR | (CI 95%) | cRR | (CI 95%) | ||||
| Risk factor exposurec | |||||||||
| Biological | 0.82 | (0.63-1.08) | 1.31 | (0.87-1.97) | 1.33 | (0.79-2.21) | |||
| Physical | 0.85 | (0.35-2.05) | 0.39 | (0.05-2.82) | 2.6 | (0.94-7.16) | |||
| Chemical | 0.80 | (0.45-1.44) | 1.48 | (0.75-2.95) | 0.99 | (0.36-2.75) | |||
| Safety | 0.56 | (0.35-0.90) | 1.22 | (0.71-2.09) | 2.75 | (1.59-4.75) | |||
| Ergonomic | 0.50 | (0.33-0.77) | 1.19 | (0.73-1.94) | 3.64 | (2.18-6.06) | |||
| Psychosocial | 0.91 | (0.66-1.24) | 0.9 | (0.56-1.45) | 1.58 | (0.93-2.70) | |||
| Non exposed | 1.47 | (1.13-1.93) | 0.79 | (0.51-1.24) | 0.18 | (0.07-0.44) | |||
| Risk level exposure | |||||||||
| 6 - 9 | 1 | 1 | 1 | ||||||
| 10 - 11 | 0.93 | (0.68-1.26) | 0.97 | (0.58-1.62) | 1.59 | (0.79-3.22) | |||
| 12 - 18 | 0.68 | (0.49-0.96) | 1.2 | (0.75-1.94) | 2.69 | (1.43-5.01) | |||
| Maternal age (years) | |||||||||
| ≤ 30 | 1 | 1 | 1 | ||||||
| 31 - 35 | 0.92 | (0.64-1.33) | 0.84 | (0.49-1.43) | 1.72 | (0.83-3.56) | |||
| ≥ 36 | 1.09 | (0.75-1.59) | 0.9 | (0.51-1.58) | 0.78 | (0.33-1.84) | |||
| Occupation | |||||||||
| Physician | 1 | 1 | 1 | ||||||
| Administrative and technical support | 1,00 | (0.71-1.41) | 1.13 | (0.58-2.22) | 0.51 | (0.10-2.63) | |||
| Nursing aide | 0.55 | (0.36-0.86) | 1.55 | (0.81-2.96) | 5.58 | (2.09-14.95) | |||
| Nurse | 0.57 | (0.41-0.81) | 1.64 | (0.94-2.87) | 5,00 | (1.95-12.81) | |||
| Type of contract | |||||||||
| Temporary | 1 | 1 | 1 | ||||||
| Permanent | 0.84 | (0.64-1.10) | 1.19 | (0.77-1.86) | 1.53 | (0.85-2.76) | |||
| Shift work | |||||||||
| Morning | 1 | 1 | 1 | ||||||
| Afternoon | 0.8 | (0.52-1.23) | 0.84 | (0.49-1.42) | 2.26 | (1.14-4.45) | |||
| Split-shift | 1.42 | (1.03-1.97) | 0.47 | (0.28-0.79) | 0.66 | (0.31-1.43) | |||
| Night and others* | 0.73 | (0.39-1.36) | 0.85 | (0.41-1.76) | 2.53 | (1.11-5.78) | |||
| Weekly work hours | |||||||||
| 36-40 | 1 | 1 | 1 | ||||||
| 30-35 | 0.91 | (0.62-1.33) | 1.04 | (0.59-1.83) | 1.28 | (0.67-2.45) | |||
| <30 | 0.99 | (0.70-1.43) | 1.12 | (0.66-1.93) | 0.81 | (0.38-1.74) | |||
a cRR: Crude Relative Risk; b CI 95 %: Confidence interval 95%; c cRR: calculated taking non-exposed as the reference category; *includes weekend shift.
Regarding occupation and taking physicians as the reference category, nursing aides and nurses had a higher probability of belonging to trajectory 3 (RR 5.58, 95% CI 2.09-14.95 and RR 5.00, 95% CI 1.95-12.81, respectively) and less likely than physicians to belong to trajectory 1 (RR 0.55, 95% CI 0.36-0.86; RR 0.57, 95% CI 0.41-0.81, respectively). Split-shift, compared to morning shift, was associated with trajectory 1 (RR 1.42, 95% CI 1.03-1.97) and negatively associated with trajectory 2 (RR 0.47, 95% CI 0.28-0.79), and both the afternoon and the night shifts were associated with trajectory 3 (RR 2.26, 95% CI 1.14-4.45; RR 2.53, 95% CI 1.11-5.78, respectively). No differences were observed for maternal age, type of contract and number of weekly work hours.
After adjusting for maternal age, type of contract and working shift, most associations there are some changes (Table 4). In particular, trajectory 1 was negatively associated with exposure to safety (RR=0.67, 95% CI 0.46-0.97), ergonomic (RR=0.59, 95% CI 0.42-0.82) and psychosocial (RR=0.77, 95% CI 0.62-0.95) risks. Trajectory 2 did not show any association, except for exposure to psychosocial risks (RR=2.56, 95% CI 1.47-4.46).
Table 4. Risk of belonging to one of the sickness absence (SA) trajectories according to risk exposure among the sample of the pregnant workers cohort with at least one NWSA episode (N=367), Parc de Salut Mar 2010 - 2014
| TRAJECTORY 1 ACTIVE WORK / MUSCULOSKELETAL DISORDERS | TRAJECTORY 2 ACTIVE WORK / SA PREGNANCY-RELATED | TRAJECTORY 3 ACTIVE WORK / PREGNANCY OCCUPATIONAL RISK BENEFIT | |||||||
|---|---|---|---|---|---|---|---|---|---|
| aRRa | (CI 95%)b | aRR | (IC 95%) | aRR | (IC 95%) | ||||
| Risk factor exposurec | |||||||||
| Biological | 0.92 | (0.76-1.12) | 1.25 | (0.83-1.89) | 2.36 | (1.54-3.61) | |||
| Physical | 0.82 | (0.44-1.54) | 0.38 | (0.05-2.69) | 3.27 | (1.58-6.77) | |||
| Chemical | 0.78 | (0.51-1.17) | 1.75 | (0.96-3.19) | 0.84 | (0.32-2.19) | |||
| Safety | 0.67 | (0.46-0.97) | 1.08 | (0.68-1.73) | 1.83 | (1.16-2.88) | |||
| Ergonomic | 0.59 | (0.42-0.82) | 1.1 | (0.71-1.71) | 2.36 | (1.54-3.61) | |||
| Psychosocial | 0.77 | (0.62-0.95) | 2.56 | (1.47-4.46) | 2.56 | (1.47-4.46) | |||
| Non exposed | 1.32 | (1.40-1.59) | 0.83 | (0.52-1.31) | 0.29 | (0.10-0.81) | |||
| Risk level | |||||||||
| 6 - 9 | 1 | 1 | 1 | ||||||
| 10 - 11 | 1.04 | (0.85-1.27) | 0.89 | (0.54-1.45) | 1.14 | (0.58-2.24) | |||
| 12 - 18 | 0.73 | (0.57-0.94) | 1.11 | (0.69-1.77) | 2.16 | (1.19-3.92) | |||
a aRR: Adjusted Relative Risk for age and workplace variables; b CI 95%: Confidence Interval 95%; c aRR: calculated taking non-exposed as the reference category.
The stratified analysis by occupation (Table 5) showed that for physicians trajectory 2 was significantly associated with exposure to chemical and safety risks (RR=3.40, 95% CI 1.39-8.34 and RR=2.59, 95% CI 1.03-6.49, respectively); for nursing aides trajectory 3 was significantly associated with exposure to ergonomic risks (RR=6.15, 95% CI 1.99-19.03); and for nurses trajectory 3 was significantly associated with exposure to physical (RR=3.10, 95% CI 1.11-8.66), safety (RR=1.99, 95% CI 1.12-3.54), ergonomic (RR=1.79, 95% CI 1.03-3.11) and psychosocial risks (RR=3.19, 95% CI 1.58-6.43).
Table 5. Risk of beloging to Sickness Absence Trajectories (SAT) according to risk exposure by occupatiion among the sample of the pregnant workers cohort with at least one sickness absence (SA) episode (N=367), Parc de Salut Mar 2010-2014
| PHYSICIAN | ADMINISTRATIVE AND TECHNICAL SUPPORT | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SAT1 ACTIVE WORK / SA MUSCULOSKELETAL DISORDERS | SAT2 ACTIVE WORK / SA RELATED TO PREGNANCY | SAT3 ACTIVE WORK / PREGNANCY OCCUPATIONAL RISK BENEFIT | SAT1 ACTIVE WORK / SA MUSCULOSKELETAL DISORDERS | SAT2 ACTIVE WORK / SA RELATED TO PREGNANCY | SAT3 ACTIVE WORK / PREGNANCY OCCUPATIONAL RISK BENEFIT | ||||||||||||
| aRRa | (95% CI)b | aRR | (95% CI) | aRR | (95% CI) | aRR | (95% CI) | aRR | (95% CI) | aRR | (95% CI) | ||||||
| Risk factor exposurec | |||||||||||||||||
| Biological | 0.95 | (0.77 - 1.18) | 0.97 | (0.42- 2.22) | 2.65 | (0.31 - 22.89) | 0.69 | (0.14 - 3.34) | 2.33 | (0.25 - 21.70) | - | - | |||||
| Physical | 0.75 | (0.37 - 1.54) | 1.26 | (0.18 - 8.68) | 5.02 | (0.65 - 38.51) | - | - | - | - | - | - | |||||
| Chemical | 0.54 | (0.27 - 1.10) | 3.40 | (1.39 - 8.34) | 2.28 | (0.28 - 18.43) | 0.88 | (0.48 - 1.59) | - | - | - | - | |||||
| Safety | 0.73 | (0.40 - 1.34) | 2.59 | (1.03 - 6.49) | - | - | 0.41 | (0.07 - 2.38) | 1.42 | (0.36 - 5.63) | - | - | |||||
| Ergonomic | 1.03 | (0.72 - 1.47) | 1.22 | (0.34 - 4.44) | - | - | 0.64 | (0.29 - 1.43) | 1.53 | (0.41 - 5.75) | 5.10 | (0.27 - 94.55) | |||||
| Psychosocial | 0.86 | (0.70 - 1.07) | 1.16 | (0.49 - 2.73) | - | - | 0.67 | (0.18 - 2.47) | 2.90 | (0.54 - 15.49) | - | - | |||||
| Global risk index | |||||||||||||||||
| 6 - 9 | 1 | 1 | 1 | 1 | 1 | 1 | |||||||||||
| 10 - 11 | 0.99 | (0.76 - 1.26) | 1.14 | (0.34 - 4.02) | 0.84 | (0.44 - 1.60) | 0.68 | (0.36 - 1.26) | 1.91 | (0.50 - 7.33) | 5.10 | (0.27 - 94.55) | |||||
| 12 - 18 | 0.78 | (0.59 - 1.04) | 1.43 | (0.46 - 4.46) | - | - | 1.65 | (0.17 - 2.33) | - | - | 0.13 | (0.01 - 1.36) | |||||
| NURSING AIDE | NURSE | ||||||||||||||||
| SAT1 ACTIVE WORK / SA MUSCULOSKELETAL DISORDERS | SAT2 ACTIVE WORK / SA RELATED TO PREGNANCY | SAT3 ACTIVE WORK / PREGNANCY OCCUPATIONAL RISK BENEFIT | SAT1 ACTIVE WORK / SA MUSCULOSKELETAL DISORDERS | SAT2 ACTIVE WORK / SA RELATED TO PREGNANCY | SAT3 ACTIVE WORK / PREGNANCY OCCUPATIONAL RISK BENEFIT | ||||||||||||
| aRR | (95% CI) | aRR | (95% CI) | aRR | (95% CI) | aRR | (95% CI) | aRR | (95% CI) | aRR | (95% CI) | ||||||
| Risk factor exposure | |||||||||||||||||
| Biological | 1.15 | (0.67 - 1.98) | 1.24 | (0.55 - 2.75) | 0.59 | (0.25 - 1.39) | 1.00 | (0.66 - 1.51) | 1.28 | (0.67 - 2.44) | 0.72 | (0.38 - 1.36) | |||||
| Physical | - | - | - | - | 2.22 | (0.77 - 6.37) | 0.91 | (0.33 - 2.50) | - | - | 3.10 | (1.11 - 8.66) | |||||
| Chemical | 1.50 | (0.61 - 3.68) | 1.40 | (0.44 - 4.41) | - | - | 1.00 | (0.44 - 2.26) | 1.21 | (0.44 - 3.35) | 0.71 | (0.26 - 1.91) | |||||
| Safety | 0.93 | (0.48 - 1.81) | 0.71 | (0.27 - 1.90) | 1.45 | (0.65 - 3.19) | 0.59 | (0.31 - 1.13) | 0.96 | (0.51 - 1.82) | 1.99 | (1.12 - 3.54) | |||||
| Ergonomic | 0.14 | (0.02 - 1.00) | 0.62 | (0.21 - 1.81) | 6.15 | (1.99 - 19.03) | 0.65 | (0.40 - 1.07) | 1.02 | (0.58 - 1.80) | 1.79 | (1.03 - 3.11) | |||||
| Psychosocial | 0.46 | (0.13 - 1.63) | 1.44 | (0.37 - 5.52) | 1.59 | (0.46 - 5.57) | 0.53 | (0.25 - 1.14) | 0.63 | (0.32 - 2.90) | 3.19 | (1.58 - 6.43) | |||||
| Global risk index | |||||||||||||||||
| 6 - 9 | 1 | 1 | 1 | 1 | 1 | 1 | |||||||||||
| 10 - 11 | 1.40 | (0.82 - 2.40) | 0.52 | (0.17 - 1.62) | 0.91 | (0.33 - 2.49) | 1.11 | (0.66 - 2.19) | 1.06 | (0.48 - 2.31) | 0.87 | (0.37 - 2.02) | |||||
| 12 - 18 | 0.64 | (0.22 - 1.89) | 0.70 | (0.26 - 1.86) | 2.03 | (0.85 - 4.85) | 0.80 | (0.44 - 1.60) | 1.25 | (0.56 - 2.78) | 1.13 | (0.53 - 2.44) | |||||
aaRR: relative risk adjusted for age, type of contract and shift work; b 95% CI: 95% confidence interval; caRR: calculated taking non-exposed as the reference category.
Discussion
Pregnancy-related health problems and musculoskeletal disorders represented up to 80% of absence days due to SA in our cohort of pregnant women, being low back pain, excessive vomiting and risk of abortive outcome the most frequent particular medical diagnoses and showing a negative or no association with exposure to occupational risk factors, respectively. Logically, we also found that women who were highly exposed to occupational risk factors, mainly biological, ergonomic, safety, hygiene and/or psychosocial, had absences from work covered predominantly by POR benefit, with one or more previous SA episodes mainly attributed to pregnancy-related medical conditions early in the pregnancy.
Our results could be explained because the POR benefit was correctly used to prevent health problems that could be caused or aggravated by adverse working conditions, such as musculoskeletal disorders in women exposed to high exposure to ergonomic risk factors. These patterns were confirmed after adjusting by age, occupation, type of contract and working shift. Those women belonging to the trajectory with SA episodes caused mainly by musculoskeletal disorders where not associated to ergonomic and psicosocial risk factors, as it would be expected. A hypothesis is that these SA episodes due to musculoskeletal disorders could be directly consequence of the pregnancy or/and non-work ergonomic risk factors. No previous study has to our knowledge included this information.
An important result from our study is that absences from work covered by SA during pregnancy were not associated to exposure to occupational risk factors. However, for physicians, we found an association between exposure to chemical and safety risks with the SA trajectory with episodes due to health problems related to pregnancy. A possible explanation to these findings is that working conditions may play a role in worsening symptoms or diseases related to pregnancy.
The frequency of SA shown in our cohort (85%) was higher in comparison with other previous studies, where reported SA during pregnancy varies from 29% to 72%33,34,35. A possible explanation may be due to differences in SA definition since some authors only consider SA episodes as those lasting more than one week or just consider those that occur only in certain weeks of pregnancy. We have registered all episodes from the first day and during the whole pregnancy period.
The main medical diagnosis of SA were pregnancy-related health problems, which confirms their important role contributing to the observed increase of SA during female reproductive age36. Previous studies had also shown that other diagnosis such as pelvic girdle pain and fatigue/sleep problems as the main reasons of SA11,37. Musculoskeletal complaints contributed substantially to SA during pregnancy in our study, being the second most frequent cause of absences from work. In fact, this is similar to the frequency of musculoskeletal disorders in the whole working population, for both men and women38,39. As reported in several studies11,40-42, low back pain was the most frequent reason of SA in our sample.
Another important implication from our results is the importance of the two current social benefits in Spain to cope with imbalances between work and health during pregnancy. On the one side, SA benefit is mainly used when pregnant workers suffer from health problems mainly related to pregnancy and/or other no-work related risk factors; on the other, POR benefit is applied when they are exposed to occupational risks before health effects occur. Our results show the suitable complementarity of the two benefits, and suggest that SA seems to be used also as a complementary way to assess the balance between work demands and physiologic changes.
This study has several strengths. First, it is based on a detailed follow-up throughout pregnancy with a precise daily register of active work and absences by SA, with or without POR. In addition, for each pregnancy we obtained detailed information on medical diagnoses of all SA from medical and SA records and a comprehensive occupational risk assessment. However, the interpretation of our results should be done with caution because of some limitations. The main one is related to the sample size and the characteristics of the study population, reducing the external validation of our results. Our sample corresponds to pregnant workers of a public university hospital who maintained their full salary during either of the two benefits as a result of an agreement with the unions. There is a need to reproduce the study in other companies with difference SA benefits schemes (usually only 70% for salary in SA benefits unless otherwise complemented, and 100% for POR benefits in Spain). In addition, most pregnant workers (76%) included in our study had a permanent contract. Nonetheless, we did not observe any differences of the magnitude of the association by type of contract in our sample. In any case, it would be interesting to analyse the same trajectories in companies of other sizes and different workforces and sectors, and with a higher proportion of temporary contracts.
In summary, a provisional conclusion is that current social benefits seem to be adequate for protecting pregnant workers from exposure to occupational risk factors, and to cope with imbalances between working conditions, health-related problems and pregnancy. Nevertheless, a great majority of pregnant women in our cohort had absences covered by SA benefit, some of them before initiating the POR benefit towards the third trimester of pregnancy. A great majority of women in our cohort had absences covered by SA benefit that could not be caused by pregnancy itself, but also, as we have seen, to working conditions43. Maybe a better management of occupational risk assessment and information provided to pregnant workers, stressing the need of POR benefit when occupational exposures are high, could reduce episodes of SA. Further research therefore needs to focus on the effects of working conditions improvement and the role of specialized preventive interventions that may help pregnant workers to ensure an adequate balance between motherhood and active work.

