










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Developmental Coordination Disorder (DCD) have been the most poorly recognized of the neurodevopmental disorders (Barra, 2019). It is one of the most prevalent childhood movement disorders, that affects around 5-8% of the child population aged between 4 and 11 years (APA-DSM-5, 2018). However, it is well-known that this disorder persists in adolescence (Ruiz, 2020). The first symptoms evident for children with this problem are related to their gross motor competence. Low skilled children may have problems achieving early motor milestones and fundamental motor skills. Likewise, during Physical Education (PE) classes, children with low motor competence have problems when they have to run, catch or dodge in games and sports, where they show an awkward style (Ruiz, 2020). The functional expression of this disorder is heterogeneous, but can involve deficits in fine motor skills, too. Different studies have shown that children with this condition have lower levels of participation in physical activities than their other peers without this problem, and are less likely to engage in both structured and unstructured physical activity and sport games, when compared to typically developing children (Li, Wub, Cairney & Hsieh, 2011). These children are less active and fit when compared to their classmates (Rivilis et al., 2011). The available research has shown that between 30% and 87% of children who reported these difficulties continued with them during the adulthood (Ruiz, Palomo, Gómez, & Navia, 2018; Williams, Thomas & Kirby, 2015).
There are other types of problems that prevent schoolchildren from attending and performing well in classes. Attentional problems have begun to be a problem among school children and appears to be associated with a wide variety of psychiatric difficulties, which are often co-morbid with it (Blank et al., 2019). This condition called ADHD (Attention Deficit and Hyperactive Disorder) could co-occurs with other childhood disorders far more often than it appears alone. ADHD children are typically characterized by developmentally inappropriate levels of attention, hyperactivity, and impulsivity that cause significant impairment in daily activities (excessive motor activity, difficulty to taking turns in PE classes, excessive talking, interrupting others, etc.). Canals, Morales-Hidalgo, Jané & Domenech (2016) consider that children with this neurodevelopmental disorder could show emotional disorders, too. These researchers found that among Spanish preschoolers the prevalence of this disorder was a 5,4%, lower than in the study of Catalá-López et al. (2012), where these researchers found a 6,8% of prevalence in Spanish children and adolescents. The hyperactive-impulsive and combined types were the most prevalent ones, and the rate of co-occurrence with other disorders was high with emotional problems. There were no considerations about motor coordination problems in these studies (Balbuena, 2016).
Attention deficit hyperactivity disorder (ADHD) and developmental coordination disorder (DCD) are both childhood disorders identified in the DSM-5 (2014) with a very similar population prevalence (Fernández et al., 2011). Thus, it is widely accepted that ADHD is a co-morbid disorder. Likewise, children with ADHD often demonstrate poor motor co-ordination or motor performance and balance. There are a substantial number of cases that have been observed, regarding problems in motor development and motor execution in children with attentional and hyperactive problems (Villa, Ruiz & Barriopedro, 2019). Clinical and epidemiological studies report that 30% to 50% of children with attentional problems suffer from motor coordination problems (Villa et al., 2019). These percentages are dependent on the type of motor assessment and the subtypes of ADHD Likewise, there are three subtypes of ADHD: 1. Combined: manifests three symptoms hyperactivity, inattention and impulsivity; 2. The predominance of attention deficit: the symptom of which is inattention; 3. Hyperactive-impulsive predominance: hyperactivity and impulsivity behavior predominates (Zamora, Calderón, Vélez & Moya, 2020).
Different researchers (Kaiser, Oosterhof, & Peelen , 2016; Pitcher, Piek, & Hay, 2003; Watemberg, Waiserberg, Zuk, & Lerman-Sagie, 2007) have demonstrated the association of DCD (a score between the 5th and the 15th percentile) with ADHD subtypes, and that the proportion of probable DCD among ADHD-I (inattentive subtype of ADHD) children was the highest, with 58% in the first study and 64.3% in the second study. The percentages were from 47.3% to 58.9%. for the combined type. Children with attentional problems display greater difficulties with the performance of motor coordination, planning and execution of complex motor skills, lengthy tasks, as well as novel chains of goal directed responses (Jodrá, Galera, Estrada & Domínguez, 2019). Furthermore, it is well known that children with attention-deficit/hyperactivity disorder demonstrate poor motor planning (Polanczyk, 2015), movement skill problems and poor levels of physical fitness (Cairney, Hay, Faught and Flouris, 2007; Harvey, Reid, Bloom & Staples, 2009; López-Sánchez, López-Sánchez & Díaz-Suárez, 2015).
Despite of the growing evidence that DCD is significantly associated with motor difficulties, many studies did not consider the role of ADHD symptoms in this relationship. Papadopoulos et al. (2013)did not find a difference at the Movement ABC-2 test (MABC-2) scores between both groups. With different assessment instruments (Licari & Larkin, 2008; McCarron, 1982) some researches did not find any difference in motor scores between the children with ADHD without motor problems and the Typical Developed Children (TD). Nevertheless, when the comparison was established between children with ADHD, DCD and the TD children, the difference was significant between these groups. There is a good evidence that children with ADHD have weaker motor skills than their peers with a special emphasis in fine motor skills (Harvey et al., 2009; Muñoz et al., 2019; Vavre-Douret, Lalanne & Golse, 2016).
It is unclear whether motor difficulties are inherent to ADHD or whether attentional problems are characteristics in DCD children. Although ADHD and DCD have many similarities, such as prevalence, high rates of comorbidities, and poor psychosocial outcomes, they appear to have somewhat different developmental pathways, which could reflect a combination of genetic and environmental factors that evolve over time (Goulardins et al., 2015). The evidence supporting common brain underpinnings is still very limited, while studies in well-defined samples point to non-shared underpinnings for ADHD and DCD, and the combination of ADHD and DCD may be not additive but potentially different (Goulardins, et al, 2015). On one hand, ADHD characterizes by age-inappropriate symptoms of hyperactivity, inattention and impulsivity. Its diagnosis takes place before age seven. On the other hand, DCD is an impairment in the development of motor coordination that is not explained by the child´s age or intellect, nor by other diagnosable neurological or psychiatric conditions. Likewise, both disorders co-exist with a comorbidity rate higher than 50% (Pitcher, Piek, & Hay, 2003; Villa et al., 2019), however, there are some authors who suggest, that both disorders might represent a single, all-encompassing disorder: Attention Deficit, Motor Control and Perception (DAMP) (Gillberg, 1992).
Although there is a wide range of literature about both disorders, the real fact is that the etiology of ADHD and DCD is still not well-understood (Gillberg, 2003). The scientific literature analyzed indicates that there are relationships between attention problems and problems of motor coordination (Carney, 2015) as previous studies had shown (Harvey and Reid, 1997). Comorbidity is considered the "rule rather than the exception" (Gillberg, 2010, p. 1543) for children with ADHD and may include intellectual disabilities, mood disorders, disruptive behavior, anxiety disorders, tic disorders, motor coordination problems and autism spectrum disorders. It could be argued that this relationship is due to a malfunction of the frontal lobe and, therefore, of the executive functions (Sergeant, Geurts & Oosterlaan, 2002). This relationship suggests that stimulating attentional processes through movement and physical activities, especially during the preschool and primary ages would yield reciprocal benefits. This is consistent with the existing evidence on how cognitive structures can be affected (especially attention) because of motor intervention at this time in children's lives (Olmedilla & Rodríguez-Igual, 2016, Thomas & Jhonson, 2008). Further evidence has also shown how coordination disorders in childhood do not manifest as an isolated problem (Miyahara, 1994). Therefore, it pointed out that coordination disorders (DCD) is closely related to the existence of problems that affect certain cognitive skills, such as the mental planning of a motor action (Dewey, Bonnie, Kaplan, Crawford & Wilson, 2002; Sugden & Wright, 1998). Longitudinal studies have revealed that children with coordination problems are at risk of learning difficulties due to the high comorbidity that exists with problems in cognitive abilities, such as those related to attention (Lyytine & Ahonen, 1989). Therefore, joint motor and cognitive assessment at early ages is highly recommended to identify the strengths and weaknesses of each child, and to be able to implement an educational intervention program to avoid future difficulties in learning (motor and academic) (Ruiz, Ruiz & Linaza, 2016).
Studies have shown that 50% of children with coordination problems were diagnosed concurrently with ADHD (Dewey et al., 2002). At school ages, research has shown how these children display lower values in their motor competence than school children who do not have any of the disorders (Chen, Tseng, Hu & Cermak, 2009; Dewey, Kaplan, Crawford & Wilson, 2002, Licari & Larkin, 2008, Martin, Piek & Hay, 2006, Shum & Pang, 2009). These results support the Posner Hypothesis (Woollacott & Shumway-Cook, 2002). This hypothesis considers that attention is the mechanism that determines the quality in the selection and processing of information for the operation of executive processes. Other studies also suggest that attention is relevant to postural control and preparation of action (Beauchet, Dubost, Gronthier & Kressig, 2005; Woollacott & Shumway-Cook, 2002).
From a neurophysiological point of view, the comorbidity of the DCD with ADHD is scientifically justified by coincidences that have been observed in the cerebral images that indicate that the bilateral inferior parietal lobe, the right dorsolateral prefrontal cortex and the left cerebellar lobes VI and IX, are closely related to the learning of motor skills, reaction time, motor planning and postural control (Biotteau et al., 2016). A lower activity of these brain areas contributes to the executive dysfunction that characterizes ADHD
Some research indicates that a severe symptomatology of inattention is a reliable predictor that there may also be serious motor coordination problems (Fenollar-Cortés & Fuentes, 2016). Arango (2015) also confirmed that the coordination levels of children with attentional problems medicated with methylphenidate (Ritalin or Concerta) and children ADHD + DCD (DAMP), show lower motor performance compared with those children without medication, or children cataloged as "typical / normal development" (TD).
The relationships between motor coordination performance and attention and hyperactivity disorders are very complex. One of the causes of low motor performance of these children is due to their lack of practice (Practice Deficit Hypothesis), since, after applying motor intervention programs, both children with coordination problems, with attentional problems and combined, improve their motor performance (Crova, Marchetti, Struzzolino, Forte & Pesce, 2014). In addition, low motor competence affects the self-image and self-esteem of schoolchildren and influences their participation in physical and sport activities (Piek & Rigoli, 2016; Ramón & Ruiz, 2015; Ruiz, Gómez, Jiménez Ramón, & Peñaloza, 2015).
Finally, different studies have shown how school children with attentional problems have had a motor experience and knowledge about motor skills lower than their peers without such difficulty, showing very negative feelings towards the practice of physical and sport activities (Harvey et al., 2004; Mora, 1997; Ruiz & Palomo, 2018). It can be accepted, that there are relationships between the two types of disorders, although it cannot be confirmed if one is the cause of the other. It is probable that a still unknown variable was the one that affects the motor and cognitive functioning of children. In order to clarify which movement difficulties are attributable to ADHD, studies need to control for the deficit in motor skills (DCD). Unfortunately, very few studies have done (Licari & Larkin, 2008; Pitcher, Piek, & Barrett, 2002).
The present study sought to compare the motor competence in ADHD with a normative sample (TD) before and after controlling for DCD If the attentional and hyperactive problems were responsible for motor difficulties, then one would expect the ADHD group to display lower motor competence than the normative group after eliminated those ADHD children than concurrently present DCD
MATERIAL AND METHODS
Participants
A total of 22 children with ADHD Combined Type (ADHD-CT; 12-13 years, 16 males, 6 females. SD 0.7) were selected because recent studies show that alterations in fine motor skills detected in children with ADHD are related to a specific motor deficit and can not be attributed exclusively to the symptoms of innatention or hyperactivity (Fernández, Burgos, Camino, López, Rico, Roncero, & Aguilar, 2011). 23 age-matched typically developing (TD) children with no movement difficulties, as evaluated by physical education teacher (16 males, 7 females), participated in this study. Participants were recruited through personal contacts from local school districts and parents. Children with ADHD were selected because parent report data indicated they met the inclusion criteria for ADHD according to the Diagnostic and Statistical Manual (APA-DSM-5, 2018) as assessed by a psychiatrist or a licensed psychologist from the School’s Department of Psychology. Four children with ADHD present learning disabilities (2 dyscalculia and 2 dyslexia). In addition, participants were considered for inclusion in the study if (1) they were capable of understanding and communicating with the investigators, (2) they were able to follow the given instructions, and (3) they were willing to engage in the requested motor skill performance. Based on the MABC-2 score (percentile score ≤ 5th), ADHD children were classified into two groups: Co-occurring DCD/ADHD (n=13) and ADHD group (n=9). Furthermore, 15 out of 22 were receiving medications (Concerta®) during the study. Parents were informed of their rights and the nature of the study and were asked to sign a consent form prior to their child’s participation. The Faculty of Sports Science and Physical Activity (Universidad Politécnica de Madrid) approved the study.
According to ethical principles, norms and international standards referred to in the Helsinki Declaration and the Human and Biomedicine Convention (Tuckman, 2000), the key factors of the study were included in a written informed consent form for participants to read and discuss with their families and psychologists.
Instruments
The Movement Assessment Battery for Children-2 (MABC-2, Henderson et al., 2011) is an evaluative tool that can be used to identify children who are significantly behind their age-matched peers in motor skill development. The MABC-2 measures both fine and gross motor skill performance for children in three age bands (3-6 years, 7-10 years, and 11-16 years). It contains eight tasks for each of the three age bands in three different constructs: manual dexterity, ball skills, and static and dynamic balance. Each task’s raw score can be converted to a standard score and to a percentile score to determine a child's motor delays compared to their age-matched norms. A total test score can be calculated by summing the eight task standard scores. Using the total test score, a percentile score can be found from the norm tables published in the MABC-2 manual to determine a child’s motor delays. The test percentile scores are described as a traffic light scoring system including a red zone, amber zone, and green zone. A percentile score ≤ 5th is classified in the red zone, indicating a significant movement difficulty. This zone is normally used for the diagnosis of Developmental Coordination Disorder (DCD). A percentile score between the 5th and 15th is classified in the amber zone, indicating a risk for movement difficulty, and a percentile score > 15th is classified in the green zone, indicating no movement difficulty detected.
Procedure
The MABC-2 was administered at a local elementary school gym by the primary investigator and research assistants. Participants were asked to wear exercise appropriate attire and shoes to complete the MABC-2. The primary investigator and research assistants followed the MABC-2 Manual when administering the tasks. Participants received detailed verbal descriptions and demonstrations prior to their motor skill performance. They were also provided additional instructions and demonstrations if they did not seem to understand or made mistakes during their practice trials. Furthermore, they were evaluated individually before attending Physical Education class. A research assistant, blind to the diagnosis and the purpose of the study, was trained to administer and then evaluate the children’s performance for each test item. Both the principal investigator and a research assistant evaluated the children’s MABC-2 motor performance in all three constructs. The empirical phase lasted two months. There were no difficulties thanks to the collaboration of the families and teachers. The assistant was considered trained once 90% agreement with the scores of the principal investigator was achieved. An inter-rater reliability test was performed between scores of the principal investigator and the assistant. Percentage of inter-rater agreement between the principal investigator and the assistant was high (97%).
Data analysis
Fine and gross motor skill raw scores were converted to percentile scores for each child using the MABC-2 conversion tables. That is, the percentile scores were generated for each area (i.e., manual dexterity, ball skills, static and dynamic balance) and their overall percentile scores (combination of all eight tasks). Results are reported as mean and standard deviation and 25th, 50th and 75th percentile. Normal distributions were checked with Shapiro-Wilk test. The requirement for normality was not met; therefore, non-parametric statistical analysis was performed. Mann-Whitney U tests were conducted on MABC-2 percentile scores to compare motor performance between groups. Additional subgroup analyses (co-occurring DCD/ADHD, ADHD, and TD) were also carried out using Kruskal-Wallis (KW) test to compare motor performance between groups. Bonferroni test was used for post hoc multiple comparisons. The effect size (ES) was calculated as η2 = Χ2/(N-1), where Χ2 denotes the statistic of KW and N denotes the total number of samples in all groups examined (Morse, 1999), and their interpretation was based on the following criteria: 0.01 ≤ ES < 0.06 small effects, 0.06 ≤ ES < .014 moderate effects, ES ≥ 0.14 large effects (Cohen, 1988). Cohen’s d effect size was also calculated to evaluate the motor delays. The statistical software package SPSS 21.0 (IBM Corp., Armonk, NY, USA) was used to analyse data. The level of statistical significance was set at 0.05.
RESULTS
Since the distributional tests showed that the requirement for normality was not met for most variables and some of the statistical indexes of shape showed departures from symmetry and mesokurtic distribution, non-parametric tests were used (Table 1).
Table 1. Skewness (S), Kurtosis (K) and Shapiro-Wilk statistic (S-W) of MABC-2 percentile scores for children groups.
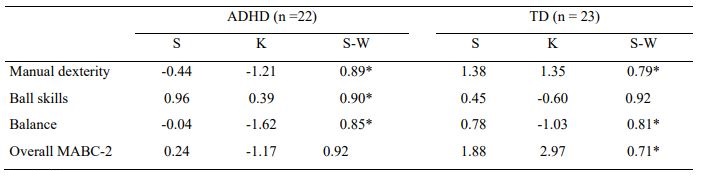
* p < .05
Table 2 showed descriptive data for percentile scores on each motor skill area and overall percentile scores (combination of eight tasks) for children with ADHD and typically developing (TD) children. Both groups showed big individual differences on all motor skills areas and on overall percentile scores. ADHD group scored significantly lower than the TD group on manual dexterity, Z = 3.89, p < .001, η2= .34, on ball skills, Z = 2.70, p = .007, η2= .17, static and dynamic balance, Z = 2.66, p = .008, η2= .16, and on overall percentile scores, Z = 4.23, p < .001, η2= .41.
Table 2. Mean (standard deviation) and percentiles of MABC-2 percentile scores for children groups. Effect size (η2)
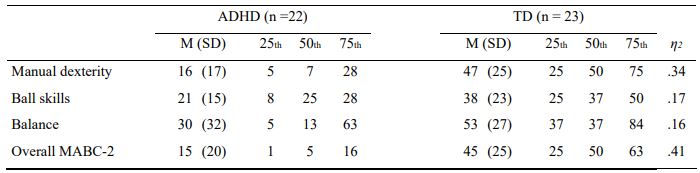
Note. ADHD = Attention Deficit/Hyperactivity Disorder Combined Type; TD = Typically Developing
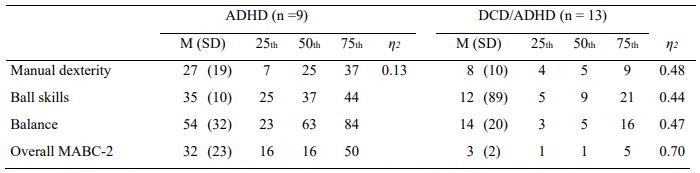
As evidenced by the traffic-light scoring system of the MABC-2, a 59.1% (n =13) of children with ADHD showed low motor performance (percentile score ≤ 5th), and 13.6% (n = 3) were at risk for motor delays (a percentile score between the 5th and 15th). Only 17.4% (n = 4) of TD children were at risk for motor delays. Based on the overall MABC-2 score (percentile score ≤ 5th), ADHD children were classified into two groups: co-occurring DCD/ADHD and ADHD Mean and standard deviation and percentile scores on each motor skill area and overall percentile scores these groups are presented in Table 3.
When comparing these two groups (DCD/ADHD and ADHD) with TD group, there were group differences across all motor skill areas (Χ2(2) = 19.21, p < .001, η2= .44 for manual dexterity, Χ2(2) = 18.88, p< .001, η2= .43 for ball skills and Χ2(2) = 17.11, p < .001, η2= .39 for balance) and on overall percentile scores, Χ2(2) = 28.66, p < .001, η2= .65. Post hoc analysis indicated that the DCD/ADHD group scored significantly lower than the TD group across all motor skill areas (p < .001 for all comparations), while ADHD group scored lower than the TD group only on manual dexterity (p < .05).
No differences were found between ADHD and TD groups comparisons on ball skills, balance and overall scores (p > .05 for all comparations). Finally, ADHD children scored higher on manual dexterity, ball skills, balance and overall scores than DCD/ADHD children (p < .01 for all comparisons). The motor delays on manual dexterity for DCD/ADHD (η2= .48) was greater than for ADHD children (η2= .13).
DISCUSSION
The present study sought to compare the motor competence in ADHD and a normative sample (TD) before and after controlling for DCD Results showed that: (1) students with motor coordination problems (DCD) and DCD/ADHD children perform poorly than controls (TD) on manual dexterity, ball skills, static and dynamic balance and overall motor skill development; (2) ADHD children only perform poorly than controls on manual dexterity; (3) DCD/ADHD children perform poorly than ADHD children on manual dexterity; and (4) The motor delays were large for ADHD-DCD and DCD children than for ADHD children on manual dexterity. These findings support that the symptoms of ADHD are in part responsible for motor delays on manual dexterity (Harvey & Reid, 2003; Whitmont & Clark, 1996).
Although in Spain there are some studies that analyze the fitness levels of students with ADHD, there are no studies that analyze their motor competence. This is the originality of the present study. Also, as is well known, the scientific literature, expresses in numerous studies, the relationships between the motor competence of students with ADHD, as indicated in the original manuscript attached. It is here, where our purpose of replication resides.
The impact of these relationships on the academic, social and motor performance of children that has been a source of concern for parents, teachers and researchers for several decades, have not been analysed in the Spanish context. Symptoms appear in the early stage of development and motor difficulties are not due to neurological, sensorial, or intellectual problems. The results have shown that there is a relationship between both types of difficulties among these children. The overlap between the two conditions was higher than 60%. Results of this study are very similar to other studies where it was estimated at about 50% of comorbidity (Fliers et al., 2008; Goulardins, Marques & De Oliveira, 2017). This link has included the different subtypes of ADHD, based on the behavioural symptomatology: predominantly inattentive (ADHD-PI, predominantly hyperative/impulsive (ADHD-HI) and both types of symptoms (ADHD-C).
In this study, children with ADHD performed lower in manual skills than the control group. Altough the inattentive subtype is typical of
comorbidity between DCD and ADHD, it corresponds to 30-40% of the total, with the combined subtype being the most frecuent (Blázquez et al., 2005). Groups of participants with DCD and DCD/ADHD performed lower than the control group on manual dexterity, ball skills, static and dynamic balance and overall motor skill development. Furthermore, the motor delays were larger for DCD/ADHD and DCD children than for ADHD children on manual dexterity. Slaats-Willemse, De Sonneville, Swabb-Barneveld, & Buitelaar (2005) claimed that fine motor problems might be a genetic marker for susceptibility to ADHD, something that Martin et al., (2006) did not supported in their genetic study. There are different hypotheses about the relationships between ADHD and DCD (Gourlardins et al., 2017). The first considers that motor difficulties are a basic expression of ADHD, whereas the second one suggests that ADHD is a secondary aspect of DCD Dewey and Volkovinskaia (2018) recognized that while DCD and ADHD are often comorbid, children and adolescents frequently present only one of these disorders.
It is reasonable assumed that adolescents with comorbid conditions would be more adversely affected with secondary health outcomes (Cairney, 2018). As Goulardins et al. (2017) indicated, while ADHD may predispose children to motor problems, it is unclear whether any such motor difficulties observed in this population are inherent to ADHD or are mediated by comorbid DCD The results of this study support that the symptoms of ADHD are in part responsible for motor difficulties on manual dexterity. Children with attentional and/or hyperactive problems could show problems to control and coordinate their bodies, a serious problem that can affect all kind of subjects, and mainly in PE classes, something that can be the origin of a sedentary life style (Cairney, 2018; Lange, 2018; Piek, & Edwards, 1997).
Another finding that emerges in this study is that from the 22 typically developing (TD) children, 12 children (a 38.7%) had developmental coordination problems or they were at risk of having these problems, what is higher that the international references of prevalence with this disorder (5 to 20%) (Rebelo, Serrano, Durante-Mendes, Paulo & Marinho, 2020). This is a serious problem that need to be recognised by educational authorities and teachers, especially physical education teachers who have the responsibility to evaluate and develop the motor competence of school children in School (Nichele et al.,2016). Physical education classes are contexts where children with ADHD or/and DCD can show their incompetence to solve motor problems and being discriminate by their mates. Knowing what children can do and perform is fundamental if teachers want to develop intervention programs and promote their development within the margins of the desirable for their age (Beyer, 1999; Harvey & Reid, 1997).
Physical Education teachers might have the knowledge, skill and experience to program interventions and palliate the effects of these conditions on children’s psychosocial development (Piek & Edwards, 1997; Ruiz & Palomo, 2018). Motor skill development is important for children, and motor incompetence may significantly affect general learning and school success. For this reason, early identification and intervention are important, not only to increase the likelihood that these children will be successful academically and socially, but also to prevent secondary emotional complications related to feelings of frustration and failure. Unless children with ADHD or motor coordination problems have been previously referred by their parents, and consequently identified by a medical practitioner, psychologist or therapist, the physical education teacher is the first professional that could provide primary care to these children (Ruiz & Palomo, 2018).
Barnard-Brak, Davis, Sulak, & Brak (2011) using a community-based, nationally representative sample of children aged 5 to 7 years old from the United States, found out that physical education, as a structured form of physical activity, may be considered as associated with lower levels of symptoms of ADHD over time. According to that there should be more researchers for early detection of motor problems among ADHD children. Unfortunately, motor problems in ADHD are still a neglected area of clinical and educational attention. The inclusion of physical therapists, occupational therapists, and physical education teachers in a multidisciplinary team that directs assistance to individuals with ADHD and DCD is essential. In addition, parents and teachers should be advised to manage attentional and motor problems to mitigate their impacts, especially regarding self-esteem and quality of life (Goulardins et al., 2017). An increased awareness and vigilance with these problems is necessary at school. Physical education teachers can improve the proportion of students with DCD who could receive a good assessment and subsequent intervention (Colombo, 2013; Harvery & Reid, 2005; Harvey, et al., 2009; Ruiz, Rioja, Graupera, Palomo & García, 2015).
More research is required to find the right intervention mix to address, not only the symptoms of these disorders, but also broader issues related to well-being, and social and individual functioning (Farhat et al., 2016; Santos de Oliveira, da Silva Oliveira, de Azevedo, Melo & Wanick, 2017; Yu, Sit & Burnett, 2018). The effect of exercise in motor coordination and attentional problems must continue to be investigated (Barnard-Brak, Davis, Sulak & Brak, 2011). The Attention Restoration Theory defends that short doses of physical activity, as 20-minute walk is beneficial for attention (Taylor & Frances, 2009). The present study suggests that the symptoms of ADHD are in part responsible for motor delays on manual dexterity and there is a relationship between DCD and ADHD
Future research should address the exact nature and long-term consequences of DCD in children with ADHD, because despite of the international scientific literature showing these relationships, the real fact is unknown. Moreover, they should be able to elucidate the effective treatment strategies for these disorders together and apart and evaluate the effect of physical activity programs in these two disorders, together o apart. Physical activity may provide a means for improving physical competence, health and being a benefit to ADHD children. As Huppand Reirman (1999) suggested, physical activities and sport can help children who suffer from ADHD and DCD on their social skills too.
CONCLUSIONS
More than 50% of the participants with ADHD presented motor coordination problems. Therefore, it is considered urgent to design an intervention plan to this type of students in Physical Education classes.
The results obtained in this research coincide with the results obtained in previous scientific studies.
It is not clear if motor coordination problems arise as a result of attention problems or vice versa. Hence the need for further investigation on this matter
The practice of physical and sport activities can contribute to the improvement of the coordination and attentional processes of these school children.
PRACTICAL APPLICATIONS
Design curricular projects for the early detection of this type of disorders. And the inclusion of motor coordination tests when children with ADHD are evaluated.
Promote the multidisciplinary working among Physical Education teachers and the School´s Psychologists at Schools.
Promote school intervention plans to avoid a sedentary lifestyle and psychosocial problems among children with ADHD and DCD

