










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.12 no.30 Murcia abr. 2013
ADMINISTRACIÓN-GESTIÓN-CALIDAD
Training for home care service staff and its benefits to users/patients
Formación del personal de ayuda a domicilio y el beneficio generado en el usuario
Simonelli Muñoz, Agustín Javier*; Solano García, Lidia*; Campillo Cano, María
*Departament of Nursing. School of Nursing. Universidad Católica de San Antonio. Murcia. E-mail: agsimonelli@ucam.edu
ABSTRACT
Home care service is essential for the care and maintenance of many people in their homes. Aware of the need for qualified home care assistance to dependent persons, we have considered some important points as to check the level of training of home care aides in the province of Almería in terms of daily household support, on the one hand and on the other, to determine how these dependent people are benefited by home care service.
This study aims to describe, observe and present a cross-section of a randomly selected sample of a total of 66 professionals working as home care aides (HCAs) throughout the province of Almeria.
Results show that the HCAs in our sample do not meet the minimum training requirement published in the BOE. More than 84% of the sample either have not completed any course related to the job or if they have done so, they have only done below the 600 hours required. Thus, we believe that in order for the HCA to be able to provide quality home care and give real benefit to users, personnel qualification and supervision are necessary for them to adequately do their job and comply with the existing legislation.
Key words: aide; training; home care service; benefit to users/patients.
RESUMEN
El servicio de ayuda a domicilio es básico para el mantenimiento de muchas personas en su domicilio. Debido a la existencia de unas necesidades de atención cualificada a las personas dependientes nos planteamos: por un lado, comprobar el nivel de formación de los auxiliares de ayuda a domicilio de la provincia de Almería, saber las actividades que realizan diariamente en los domicilios y, por último, determinar el beneficio en el usuario que aportan con su cuidado.
Se trata de un estudio descriptivo, observacional, transversal en el que se seleccionaron a través de un muestreo aleatorio simple a un total de 66 personas que trabajaban como auxiliares de ayuda a domicilio (AAD) por toda la provincia de Almería.
Los resultados muestran las AAD de nuestra muestra no cumplen los mínimos de formación que vienen reflejados en el BOE, pues más del 84% o no tienen cursos relacionados o los tienen por debajo de las 600 horas. Así, creemos que para que los AAD puedan proporcionar unos cuidados de calidad que reporten un beneficio real en los usuarios, es necesario cualificar y supervisar a dicho personal para que puedan cumplir adecuadamente su trabajo conforme a lo dispuesto en la legislación vigente.
Palabras clave: auxiliar; formación; ayuda a domicilio; beneficio usuarios.
Introduction
For decades, we have experienced a series of important social and demographic changes in our society. One of such significant changes is the increase in the life expectancy of our elderly, which, in turn, has brought about an increase in the number of this ageing population1,2.
In addition, there is another series of steady changes in a large number of people, who, in spite of their illness and disability3, live on their own as a consequence of the lack of space to accommodate them in public nursing homes, amongst other reasons1.
Traditionally, a dependent person was assisted by the members of his or her own family, mainly women2,4,5. Nowadays, as a result of the changes in patterns of family structure, as for instance, women's participation in the labour force and the changes in family models, a significant modification has also been observed in terms of family/household support 6 In the same manner, home care service comes into view as the need to take care of the elderly people arises, the longest possible time in their own homes, as their usual environment7.
Home Care Service [Servicio de Ayuda a Domicilio (SAD)] is defined in the "Andalucía Social Services Act 2/88 approved on 4th of April (art. 10, par. 3)"8 as a kind of "service that caters to benefit individuals and families in terms of home, social, and personal assistance, at the same time, enabling self-support in their household environment."
In 2012, the Department of Equality and Social Welfare of the Regional Government of Andalucía officially decreed on 21st of March the regulation of Home Care Service as basic compensation of the Common Social Services Benefits (BOJA no. 65, 3rd April 2012)9. This decree establishes the basic applications of such benefits offering complete home care service to its recipients, stressing its instructive and preventive nature.
Because of its extremely preventive and normalized nature, home care assistance acquires special relevance as part of the Social Services Benefit of the Public System that offers complete assistance to different needs, assuring a personalized homely attention, thus, avoiding displacement caused by confinement in a nursing home and preventing stress in the family as loss of self-esteem, hopelessness, dejection, sadness, stress, frustration, burden and loneliness10-13, decreasing their anxiety14 through psychological and social intervention. Such intervention will surely favour and enhance the patient's capacity to achieve maximum personal autonomy15.
Indeed, it is logical, at this point, to raise doubts and questions about the persons who will be involved in carrying out the tasks of this service, such as the kind of training background Home Care Service workers must have on the one hand, and, on the other, the kind of professionals who will have to supervise their work considering its transitory and complementary nature.
Meanwhile, the Public Administration clearly establishes, as published in the supplement of the BOE 22nd of March 200416 issue, the minimum requirement for any candidate opting to work as a Home Care Aide (HCA): the possession of a Professional Certificate equivalent to a 600-hour training course.
The completion of a 600-hour training course necessary to obtain the Professional Certificate is outlined in a combined programme of theory and practice as specified in the following modules:
1. Hygiene and home health care (230 hours).
2. Psychosocial home care and support (270 hours).
3. Household support and family diet (100 hours).
These modules are fundamental tools to deliver professional care as the job demands formal, high-quality health care in order to benefit the clients or patients.
With regard to supervision, we firmly believe that nursing plays a basic role inasmuch as the nature of the job involves instruction and supervision. Nursing is a field related with home health care, and more specifically with the tasks caretakers have to carry out in areas such as prevention, training, assistance and rehabilitation. This affirmation becomes even more relevant if we take into account the four main pillars of the nursing profession:
1. Instruction: The quality of Personal Assistance Service depends mainly upon the training of the professionals involved17. If we take a close look at the course content as published in the State Official Bulletin Supplement16, we may observe that the whole course practically covers health care science and specifically, nursing, which is why nurses are the best choice to train homecare aides.
2. Assistance: The nurse will have to supervise and coordinate the progress of the HCA's work since the patients are usually elderly, highly dependent and affected with several diseases18 at the same time. In this regard, social workers are definitely not qualified to attend to their health care needs and to make certain decisions on matters affecting the patients' health.
3. Research: Investigating in this field will surely help improve the situation of the patients, their families and the HCAs themselves, as well as the effectiveness of the Home Care Service, whose main beneficiary is the society in general.
4. Management: To achieve maximum diligence, efficacy and efficiency in order to benefit not only the different agencies of the public administration but also the patients, who are the same recipients of this service.
It is necessary to underline the transitory and complementary nature of home care service, which coincides with Orem General Theory of Nursing19. The idea of this kind of assistance is temporary and not for life. The main point is to get the clients/patients to learn to be self-sufficient by getting them involved in taking care of themselves (Healthcare and Self-sufficiency Theory), even when the client is not capable of carrying out this task themselves19.
The preparation of this study is based on the existence of the demand for qualified healthcare service in response to the needs of dependent persons and for the means, which our society, through its social policies, has to develop in order to satisfy such demand. It is, then, but fair to meet this challenge through the personalization of the services offered, the application of new technologies in granting social benefits and in the information system in order to uplift the sector's standard20. By doing so, we eventually achieve an improvement in the quality of these dependent persons' lives insofar as they will not be obliged to abandon their homes and to guarantee their holistic health care. Likewise, we consider the topic of this study relevant and necessary as there has been a dearth of research studies on this field.
Objectives
1. To verify the knowledge and training level of home care aides in the province of Almería.
2. To find out about the daily activities carried out in the homes of the clients/patients.
3. To determine the general good provided by home health care service depending on the aides' knowledge and training level.
Methodology
We have designed our study based on description, observation and a cross-section analysis in order to fulfil the objectives presented.
Study Population
The target study population is the home care aides who work in the province of Almería for ASER, the company that provides home care service personnel.
The study population is comprised of HCAs that meet the following criteria:
Inclusion criteria:
- HCAs, with no age limit and of both sexes, who attend annual conferences in the municipality of Mojácar.
Exclusion Criteria:
- HCAs who are unable to answer the questionnaire individually.
We intend not to make the selection criteria restrictive to be able to extrapolate the results to the target study population.
Sample
The sample is composed of a total of 66 people working as HCAs throughout the province of Almería at the time the survey was conducted. From the said sample, 51 (92 as the target population) were working in the municipalities whose population is less than 20,000 and 15 (total study population) were working in the municipalities of El Ejido and Roquetas de Mar, each of which has a population of over 20,000.
The study sample was obtained through the company which provides Home Care Services and which has a signed agreement with the Provincial Council of Almería in municipalities with less than 20,000 inhabitants. A detailed explanation of the research study was given -its scope, its target objectives- and the approval was granted. It was finally decided that a simple random sampling be used since at the time of the survey, there were a total of 92 HCAs distributed throughout the provincial territory, a rather complex situation to resolve. The data were gathered during ASER's (the company's) annual conference, which offers the possibility for all its workers to attend.
A questionnaire developed by the authors of this study was used as a tool for collecting data. Questions were open-ended but mostly close-ended. The study variables are described as follows:
- Independent Variable (I.V.): The occupational training of the Home Care Aides. Assessment through the completion of courses that exceed 300 hours for Home Care Aides.
- Dependent Variable (D.V.): Benefits patients or users derive from health care (formal care). Assessment by using three variables: 1. If they usually plan things out in their daily work/tasks; 2. If they correctly define what "to plan" is; 3. If they record in some way the activities they carry out. To obtain the result, another variable is created, which is the sum of these three (variables) and the score assigned from 1 to 3 points, with 3 as the minimum and 7 as the maximum score. We assess whether or not they correctly define "planning" according to two definitions set by the Royal Spanish Academy21 and the Dictionary of Nursing22. The former defines it as "a general plan, methodically organized and usually on a large scale, to obtain a certain objective..." whereas, the latter defines it based on the following situation: "... After identifying the real and potential problems related to the daily activity, the patient takes part in the setting of appropriate objectives, which must be achieved through the nurse's actions.
Statistical Analysis
The data gathered were processed in the Microsoft Excel database and were exported to the SPSS statistics program 15.0 version.
The determination of absolute and relative frequencies are expressed in percentages. Calculation of measures and typical determinations. Levene's test was employed to check the equality of variances and Student's t-test was used to determine the significant differences between variables. For hypothesis testing, the results obtained for p< 0.05 will be considered significant.
Results
From HCA sample (n=66), 98.5% are women. 77% worked throughout the province of Almería (municipalities with less than 20,000 inhabitants), 12% in the town of El Ejido and the rest, 11%, in the town of Roquetas de Mar.
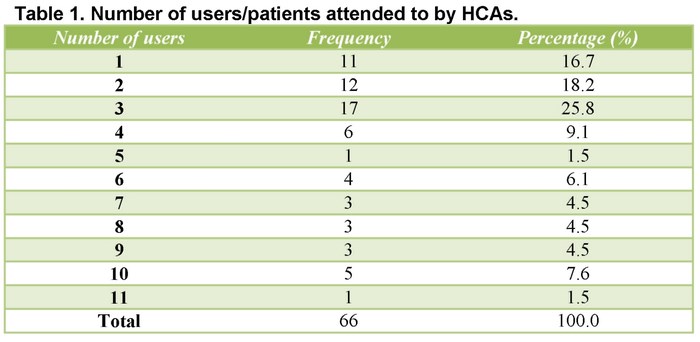
The average number of users/patients per HCA is four, with a typical deviation of 2.93, with a minimum of 1 user and a maximum of 11. (Table 1)
With regard to the educational attainment of the HCAs, our sample shows that 17% have no formal schooling; 54% finished primary education; 15.2% are nursing aides; 10.6% have vocational school training; and 3% either have attended college or are college degree holders.
It is interesting to note that 13.6% of HCAs working in Almería admitted not having done any course on Home Care Service when asked about what courses they had attended; 53% had done courses below 100 hours; 12.1% had done between 100 and 300 hours; and only 10.6% had done courses for more than 440 hours. Moreover, 89.4% of the courses were less than 440 hours.
Furthermore, we have to point out that 42.4% of these courses were exclusively theoretical in contrast with 45.5% which were about theory and practice.
It should also be noted that 90.9% of our sample agrees on the necessity of doing periodic training courses; 4.5% do not consider it advisable, and another 4.5% either do not know or do not answer.
With regard to the duration of HCA training, our sample thinks it should last an average of 4.3 months to obtain qualification to work for HCS. 15.4% think it should be one month or less; 18.2% from one to two months; 19.7% from two to three months; 15.2% from three to four months (a cumulative 69.2%); and 27.3%, a minimum of five months.
In response to the question on the purpose or reason why they need to have more knowledge about home assistance, 15.6% of the HCAs surveyed consider that it helps them in their job. 39.4% think that training helps them to feel more confident in their job, and 3% express that knowledge from training helps, but considers it unnecessary.
When asked to adequately define what planning is, only 33.3% did it adequately and the rest, 66.7%, did not define "planning" correctly.
On the question whether they usually plan what they are going to do in the homes they visit, 31.8% do not plan their work beforehand, whereas 66.7% do. In the case of the latter, 62.1% carry out their work independently; 21.2% do it together with the social worker; 3% with the nurse's or doctor's supervision; and 13.6% with several professionals.
More than half of the HCAs surveyed (66.7%), confess they never record what they do; 15.2% do it once in a while; and the rest, 18.2%, write down the activities they do with the users.
In response to whether the users are satisfied with the work done, 43.9% of HCAs do think so, but they want to spend more time in the user's home; 27.3% say they are totally satisfied; 18.2% think they do, even if they do not do what the users want them to do; and 1.5% do not think so because they do not do all the things they want to do.
When asked whether they appreciate their job as professionals, the HCAs surveyed think that HCS users welcome their job as professionals with 69.7% of approval against 22.7% who think otherwise. The rest do not know and do not answer.
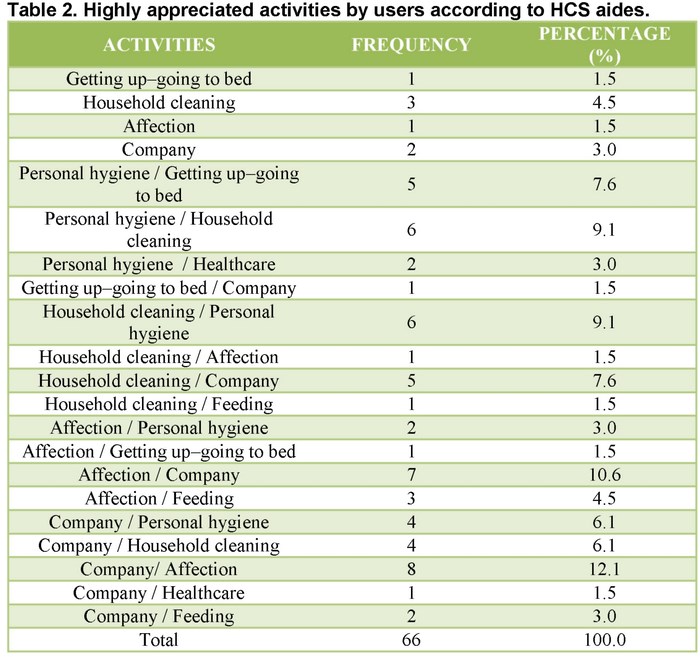
According to the HCAs, the activities users appreciate most are, in the first place, 32%, for keeping them company; 24% prefers household cleaning; 21% for affection showed; 20% for the personal hygiene; and 3% for helping them get up and go to bed. Secondly, the HCAs appreciated the following aspects: 21% company; 18% personal hygiene; 18% feeding; 15% household cleaning; 14% affection; 9% getting up-going to bed and 5% health care. (Table 2)
When asked about the activities they do daily in the users' homes, they respond in order of importance as follows: 73% personal hygiene; 7% feeding; 5% getting up-going to bed; 6% household cleaning; 3% company; 2% healthcare; 2% affection; and 2% medication. Secondly, 26% do household cleaning; 24% feeding; 15% medication; 11% helping to get up-go to bed; 6% health care; 6% personal hygiene; 6% company; 3% affection; and 3% errands. (Table 3)

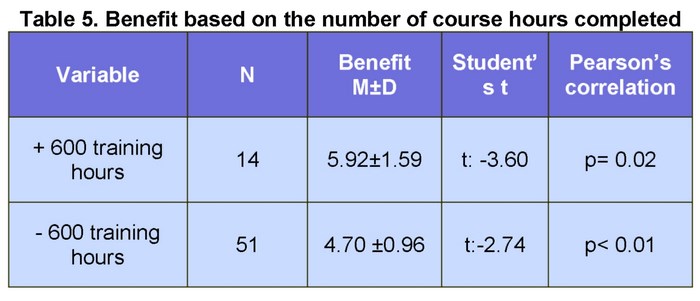
When we compare the averages between HCAs whose academic training is close to the requirements guaranteed by the Professional Certificate published in the BOE (more than 600 hours) and HCAs who do not meet this requirement (under 600 training hours or none at all), and after correlating this with the three variables (definition of planning, planning and recording) that refer to the actual planning HCS workers do in their job, that is, the benefit gained, we can observe that the average is higher with subjects with more than 600 hours' training with the resulting significant statistical difference of p < 0.015.
Discussion
The HCA sample that pertains to the province of Almería does not meet the minimum training requirement as published in the BOE, because more than 84% either do not have any related course done or have only done less than 600 hours. Following the current regulations found in the BOE supplement, the standard requirement is the so-called Professional Certificate equivalent to a minimum of 600 training hours16.
We can conclude that the HCS workers have no adequate training which will qualify them to act when faced with different situations. Citing the article provided by the State Employment Public Service23, the tasks that a home care aide are the following: carry out household tasks (doing the cleaning, the household shopping, the cooking, the washing, etc.) and personal attention (personal care, hygiene and health maintenance of bedridden persons, going to therapeutic visits, taking care of doctor's prescriptions, etc.).
According to Sánchez S and Mears R24, caregivers recognize the increased load task generates them is the bathroom / toilet and need more help multidisciplinary team24.
They are unable to determine the needs of the users and those related with health care, and set goals and meet them in the end. They have been chosen to work in this field with no training whatsoever, although some of them have later shown interest and have done something.
We can also say that the work done by the auxiliaries with the users lacks professionalism and therefore it resembles what is called as "informal care", which means that the benefit received by the user is reduced to a series of domestic-like activities insofar as the training requirement is minimal. This work is usually done by family members (women, in general), with no formal schooling, and whose main occupation is housekeeping. They do not have the adequate skills necessary to carry out the tasks of looking after the persons under their care. Formal care would mean help, not a substitution, in which the efforts of the family members complement those of other caregivers and wherein proper care is shown and learnt. At present, these care services are not well-known among the population due to bureaucratic hurdles, location inequalities, service costs, confidence in informal caregivers, etc25.
On the other hand, they themselves admit, 91%, that it is necessary to attend courses periodically, and 28% think that all HCAs should have a minimum of five months'specific training to carry out their work with HCS users; then they agree that minimum knowledge and skills are required to do the job properly. They recognize the fact that proper training will help them do their job better and will give them confidence when they attend to the user's needs.
A little less than half, 32%, admit that they do not plan at all and a little more than half, 67%, say that they usually plan what they do with the user. It is surprising to find out that almost 82% do not record or they do once in a while; 48% plan their tasks without relying on the help of other experts and only 13.6% plan with several professionals (a requirement that must be taken into account for any planning of this kind). These aspects are fundamental when planning assistance and therefore, in offering quality care, if not, there will be no sense behind the existence of HCS. It is important to evaluate and record available health care resources to carry out an adequate health care plan. Besides, recording will serve as a reference to monitor the patient's progress26.
We have found significant differences between HCS workers who have completed more than 600 hours of training and those with less training hours, concerning the benefits given to users/clients with a p<0.01. We can therefore assert that the low training level of homecare aides is converted into informal care of the clients availing of this service. It would be essential to do another study within this same context, but obtaining a bigger sample in which HCAs will have the minimum training level required to obtain the Professional Certificate with the nursing staff taking charge of the training, coordination and supervision of HCS.
The definition of Home Care Assistance, as we have already stated in the introduction, is as follows: "a complementary and transitory service, preferably in one's own family home, which provides, through qualified and supervised staff, a range of services to attend to the individuals' and their families' needs through protection, training, assistance and rehabilitation, especially those with difficulties in staying in their homes"27. And if this is not carried out, we are not actually achieving our objectives.
Conclusion
It is imperative on the part of the HCAs to provide quality health care and attention to actually benefit the users; it is really necessary for the nursing staff to train and supervise the HCA personnel for them to respond adequately to their job in accordance with the current regulation.
Works cited
1. Trigueros I, Mondragón J. Manual de ayuda a Domicilio. Formación teórico-práctica. 3aed. Madrid: Siglo XXI; 2008. [ Links ]
2. Martínez R, Ponce DE. Valoración de los conocimientos del cuidador principal sobre úlceras de presión. Enfermería Global 2011; 10(2): 60-84. [ Links ]
3. Fornés J. Enfermería en Salud Mental. Cómo cuidar al cuidador y a nosotros mismos. Enfermería Global 2003; 2 (1): 1-11. [ Links ]
4. Da Silva MJ, Braga M, Da Silva CT. Evaluación de la presencia del síndrome de Bournout en cuidadores de ancianos. Enfermería Global 2009; 8(2): 1-11. [ Links ]
5. Blanco R, Zapico F, Juanola MD, Aguas A. Entorno y necesidades de salud de la población mayores de 75 años no atendida en cuatro áreas de salud de Barcelona. Enfermería Global 2003; 2(2): 1-11. [ Links ]
6. Gobierno de La Rioja. Detección de Necesidades Formativas en Atención a la Dependencia. La Rioja: Altia Consultores; 2009. [ Links ]
7. Serrano P, De Tena-Dávila, MC. Criterios de fragilidad en los usuarios del servicio de ayuda social a domicilio. Rev Esp Geriatr Gerontol. 2004; 39: 9-18. [ Links ]
8. Ley 2/1998, de 4 de abril, de servicios sociales de Andalucía. (Citado: enero 2010). http://salud.discapnet.es/Castellano/Salud/Salud Mayores/Legislación/Documents/f560b98364ac47cb86613e13984967d4Ley21988andalucia.pdf [ Links ]
9. Boletín Oficial de la Junta de Andalucía (BOJA). Martes 3 de Abril de 2012, no65. [ Links ]
10. Moreira R, Teresa RN. Paciente oncológico terminal: sobrecarga del cuidador. Enfermería Global 2011; 10(2): 1-13. [ Links ]
11. Martínez FE. Recuperación de la Salud del cuidador principal, en proyecto sociocultural "Quisucuaba". Los sitios, Centro Habana. Enfermería Global 2012; 11(1): 92-103. [ Links ]
12. González J, Armengol J, Cuixart I, Manteca H, Carbonell M, Azcón MA. Cuidar a los cuidadores: atención familiar. Enfermería Global 2005; 4(1): 1-8. [ Links ]
13. Villarejo L, Zamora MA, Casado G. Sobrecarga y dolor percibido en cuidadoras de ancianos dependientes. Enfermería Global 2012; 11(3): 159-165. [ Links ]
14. Da Costa M, Karine A, Chaves SP, Peçanha TJ, Silva F. Programa para cuidadores de ancianos con demencia: un relato de experiencia. Enfermería Global 2011; 10(2): 1-9. [ Links ]
15. Medina ME. Evaluación de la calidad asistencial del servicio de ayuda a domicilio. Murcia: Publicaciones Universidad de Murcia; 2000. [ Links ]
16. Suplemento del Boletín Oficial del Estado (BOE). Martes 9 de marzo de 2004, no59 p 714. [ Links ]
17. Montalvo M, Díaz E. Programa de formación de auxiliares de ayuda a domicilio. Centro de salud 1999; 7(5): 315-316. [ Links ]
18. García M, Torres MP, Ballesteros E. Enfermería geriátrica. 2a Ed. Barcelona: Masson; 2000. [ Links ]
19. López AL, Guerrero S. Perspectiva internacional del uso de la teoría general de Orema. Invest. educ. enferm. 2006; (24)2: 90-100. [ Links ]
20. Antares Consulting. Modelo de futuro del servicio de atención a domicilio. España: Senda Editorial, S.A; 2007. [ Links ]
21. Real Academia Española. Diccionario de la lengua española. Madrid: Espasa Clape; 2005. [ Links ]
22. Roper N. Diccionario de Enfermería. 16a Ed. México: McGraw-Hill interamericana; 2000. [ Links ]
23. Servicio Público de Empleo Estatal (INEM). Aprendizaje a través de la experiencia como generador de competencias profesionales, en el ámbito de la Ley de Promoción de la Autonomía Personal y Atención a la Personas en Situación de Dependencia. (Internet) Ministerio de Trabajo y Asuntos Sociales. (Actualizado el 13 de Marzo de 2008, consultado el 26 de Marzo de 2012). Disponible en: http://www.fundaciontripartita.org/almacenV/doc/Estudios/130191331332008141145.pdf [ Links ]
24. Sánchez S, Mears R. Cuidador del enfermo de Alzheimer terminal. Enfermería Global 2005; 4(2): 1-26. [ Links ]
25. Mayte JAM, Abellán A. La atención formal e informal en España. Sancho M. (coord.) Las personas mayores en España. Informe 2000. Madrid: Ministerio de Trabajo y Asuntos Sociales; 2000. P.: 863-911. [ Links ]
26. Rodríguez P, Valdivieso C. Los servicios de ayuda a domicilio. 2a Ed. Madrid: Editorial Médica Panamericana; 2003. [ Links ]
27. Reglamento para la Gestión del Servicio de Ayuda a Domicilio. Boletín Oficial de la Provincia de Almería (BOP). Jueves 23 de Octubre de 2003, no 203. [ Links ]

