










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.13 no.34 Murcia abr. 2014
DOCENCIA-INVESTIGACIÓN
ICT Knowledge and Access by Individuals with Chronic Illness and Family Caregivers in Colombia
Conocimiento y acceso a las TIC en personas con enfermedad crónica y cuidadores familiares en Colombia
Carrillo González, Gloria Mabel*; Chaparro Diaz, Lorena** and Sánchez Herrera, Beatriz***
*Master in Nursing. Associate Professor. E-mail: gmcarrillog@unal.edu.co
**PhD in Nursing. Associate Professor
***Master of Science of Nursing. Full Professor. Faculty of Nursing. Universidad Nacional de Colombia
ABSTRACT
Objective: This study seeks to discover the level of knowledge and access to information and communication technologies of individuals with chronic noncommunicable disease and family caregivers in Colombia.
Methodology: This was a national, cross-sectional descriptive study with a sample of 2432 individuals with chronic noncommunicable disease and family caregivers located in different regions of Colombia, in whom we determined the level of knowledge and access to information and communication technologies.
Results: In individuals with chronic noncommunicable disease and family caregivers low level of knowledge and insufficient access to information and communication technologies prevails.
Conclusions: Information and communication technologies are significant tools in caring for individuals with chronic noncommunicable disease and in supporting family caregivers. Knowing their level of access and knowledge in the different regions of the country evidences a heterogeneous panorama that must be considered if the General System of Social Security in Health seeks to provide universal coverage.
Keywords: Chronic disease; Caregivers; technological development.
RESUMEN
Objetivo: Describir el nivel de conocimiento y acceso a las tecnologías de información y comunicación (TIC) que tienen las personas con enfermedad crónica no trasmisible (ECNT) y los cuidadores familiares en Colombia.
Metodología: Estudio nacional descriptivo, transversal con una muestra de 2432 entre personas con ECNT y cuidadores familiares ubicados en diferentes regiones de Colombia, en quienes se determinó nivel de conocimiento y de acceso a las TIC.
Resultados: En las personas con ECNT y los cuidadores familiares predomina un nivel de conocimiento bajo y un acceso insuficiente a las TIC.
Conclusiones: Las TIC son herramientas significativas en el cuidado de las personas con ECNT y en el apoyo a cuidadores familiares. Conocer su nivel de acceso y conocimiento en las diferentes regiones del país, deja ver un panorama heterogéneo que debe ser tenido en cuenta si el Sistema General de Seguridad Social en Salud pretende dar una cobertura universal.
Palabras clave: Enfermedad crónica; Cuidadores; desarrollo tecnológico.
Introduction
It is well known that chronic noncommunicable disease (CNCD) is a public health problem in Colombia(1). Expert researchers have indicated that research in this field should be a priority(2). Having a CNCD generates an impact upon the lives of patients, their families, especially on those who fulfill the role of principal caregivers, professionals or formal caregivers, healthcare institutions, and on the General System of Social Security in Health (GSSSH, for the term in Spanish)(3). Several authors suggest exploring the use of information and communication technologies (ICTs) in caring for individuals with CNCD(4,5,6). Experiences are also reported of those who have successfully employed them in family caregivers of individuals with this condition(7,8,9). In Colombia, ICTs open the possibility of having greater communication with users of healthcare services to improve their information and with the generation of healthcare promotion strategies given that most workers from the Colombian healthcare sector show interest in their use to support the professional's daily exercise(10). Hence, it has been suggested that institutions review how to modernize their service offer, especially in the field of virtual education and services that facilitate remote out-of-hospital follow up, seeking cost-effectiveness and greater impact on public health(10).
Multiple and varied studies exist on the use of ICTs in healthcare in the world. We must recognize the possibilities these ICTs offer to connect continents to respond to the challenge of formation and development of different countries Their strategic importance as a tool has been highlighted, without overlooking that access can generate effects on social gaps(12). Likewise, the potential benefits of ICTs are highlighted in healthcare with transformation of conventional offers, as long as access is guaranteed to information inter-institutionally and ethical-legal aspects are addressed so that necessary and adequate conditions are achieved for their use(13). The impact of ICTs in administration has also been documented, which depends on the training and effectiveness of the human resource and on its ideological guidance, which is convenient to make explicit(14). Added to its benefits are knowledge and contribution to the economic and social development they can generate(15). However, it is urgently necessary to revise user expectations and operation of services to integrate the wellbeing, economic, and clinical information to respond user expectations(16). Similarly, it is mandatory to revise the relationship between access to information and equity in healthcare where ICTs must fulfill an essential function as a public good(17). That is, not merely having ICTs, but having the health of individuals and communities as the north without forgetting the latent risk of increasing the social gaps and permitting to waste a magnificent opportunity to improve the quality of life of users(18,19).
This study sought to evaluate knowledge and access of ICTs by individuals with CNCD and of family caregivers in Colombia, understanding that ICTs are -undoubtedly- a valuable tool to breach distances, facilitate and systematize processes, inform, educate, and support interdisciplinary healthcare required by these users in a SGSSSH that expects universal assurance. Knowing what happens on the use of ICT by individuals with CNCD and their family caregivers in the different regions of Colombia is fundamental to diminish the burden of caring for CNCD.
Methodology
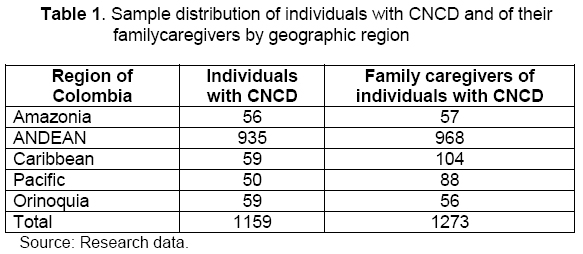
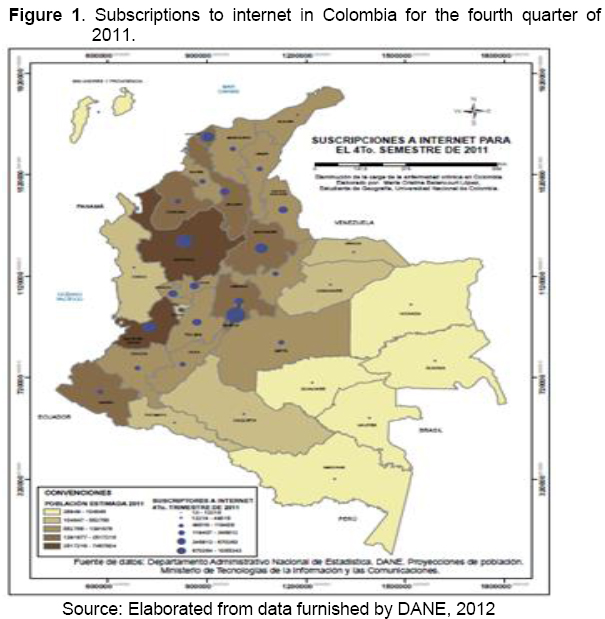
This was a cross-sectional, descriptive study conducted in different regions of Colombia during the second semester of 2012 as part of a broader project denominated "Program to diminish the burden of CNCD in Colombia". To know the relationship of individuals with CNCD and that of their family caregivers with ICTs in Colombia, we began by reviewing data on availability of access to internet in the national territory(20). Thereafter, and upon verifying that the whole territory has access to this resource, a reality described by Gutiérrez de Pineda(21) was reviewed on the diverse characteristics and cultural variations of the Colombian population according to the geographic regions, taking for this study the five big Colombian geographic regions that include: the Caribbean (insular and continental), Orinoquia, Amazon, the Pacific, and the Andean region. In each of them, interviews were conducted of individuals with CNCD and of their family caregivers to analyze their knowledge and access to ICTs. The following instruments were used in gathering the information: "GCC-UN-P" characterization of individuals with CNCD and the "GCC-UN-C" characterization of family caregivers of individuals with CNCD, which include, among others, information on access and knowledge about ICTs. The sample was comprised of 2432 individuals among those with a CNCD and those who perform the role of family caregiver, regionally distributed (Table 1).
Data were taken via direct interview by the researchers or research aides specially trained for this purpose and bearing in mind in each case the informed consent. The study considered the ethical aspects regulated by Resolution 8430 of 1993(22). The study adhered to the environmental policies of Universidad Nacional de Colombia, especially in the responsible use of resources (23). All the results were processed in the SPSS program (version 16.0) with permanent support of a statistics consultant.
Results
In Colombia, according to official data, eight of every ten individuals have access to internet(24). However, upon reviewing the real possibilities by regions, the panorama is totally heterogeneous (Figure 1).
Knowledge and access to ICTs en individuals with chronic disease
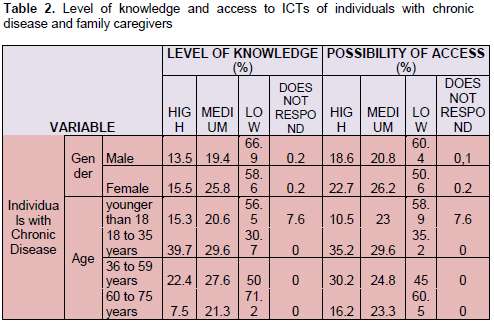
The revision of knowledge and access to ICTs of individuals with CNCD by gender revealed that men reported having optimal knowledge in 13% of the cases, while women did so in 15%. On access, the percentages reported of optimal access were 18.6% for men and 22.7% for women.
With respect to the ages of individuals with CNCD an optimal level of knowledge of ICTs was found in 15.3% of the individuals younger than 18 years of age; 39.7% in the group 18 to 35 years of age; 22.4% in adults from 36 to 59 years of age; 7.5% in elderly adults 60 to 75 years; and 6.3% in adults over 75 years of age. The possibility of access was scored as optimal by 10.2% of those younger than 18 years of age; 35.2% of the adults between 18 and 35 years of age; 30.2% in adults from 36 to 59 years of age; 16.2% in elderly adults between 60 and 75 years of age; and 12.5% in adults over 75 years of age.
Regarding the level of schooling, a clear association exists between the educational level reached by the person with CNCD and his/her knowledge of ICTs maintained with a small variation with respect to the level of access reported.
Knowledge and access to ICTs in family caregivers of individuals with CNCD
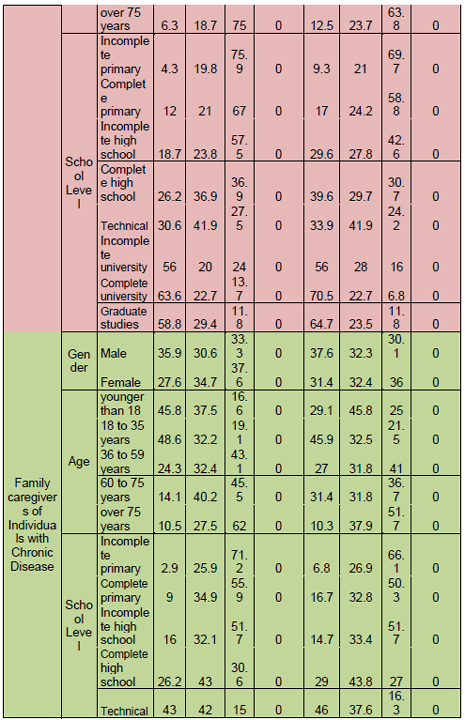
With respect to family caregivers of individuals with CNCD, upon revising their level of knowledge and access to ICTs by gender, an optimal level of knowledge was found in 35.9% of the men and in 27.6% of the women, while optimal access was seen at 37.6% in men and 31.4% in women.
According to age, family caregivers of individuals with CNCD showed better level of knowledge at younger ages, while for access, adults, especially young adults and elderly adults reported better access.
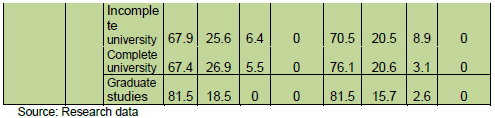
In terms of level of schooling, family caregivers revealed that higher educational levels indicated higher levels of iCt knowledge. This tendency was repeated including graduate studies in optimal access to ICT reported by these caregivers with some small fluctuation between the group with complete primary and the group with incomplete high school (Table 2).
Level of knowledge and general access to ICTs of individuals with CNCD and their family caregivers
Regarding the level of knowledge of individuals with CNCD, it may be noted that it was optimal in 14.9%, while 85.1% has medium or low knowledge, with 61.6% in low level. Regarding access to ICT of individuals with CNCD, it was found that it was optimal in 21.4% of the cases with the remaining 78.6% with insufficient access, being 54.2% the low level.
The case of family caregivers reflects that 29.4% has an optimal level of knowledge, while 70.6% lacks such. The majority group is that with the low level of knowledge with 36.7% of the caregivers. The case of family caregivers reflects that 32.8% has an optimal level of access, while 67.2% lacks such. The majority group is that with the low level of access with 34.7% of the caregivers.
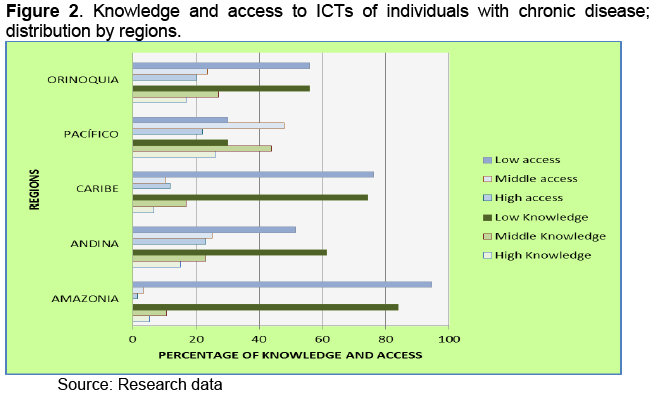
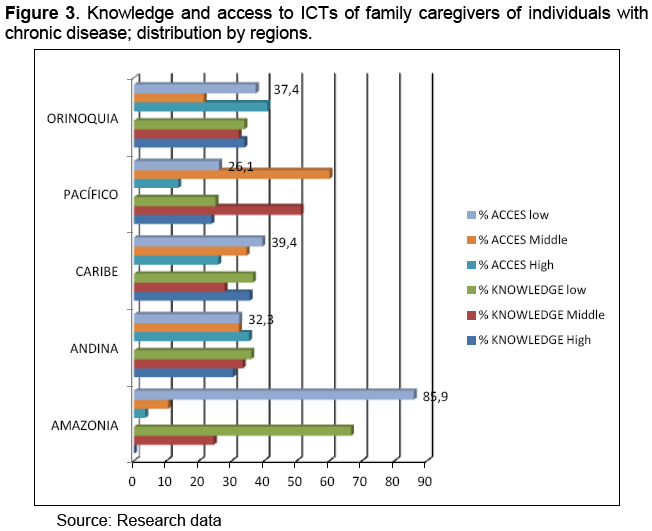
Knowledge and access to ICTs by region in individuals with CNCD and their family caregivers
Upon reviewing access to ICTs by region, it was found that the cultural and geographic diversity is accompanied by a real difference between the possibilities of individuals with CNCD and their family caregivers against knowledge and access to ICTs (Figures 2 and 3).
Discussion
In the revision by gender, in the case of individuals with CNCD, both men and women showed medium and low levels of knowledge and access with the female level being slightly higher in both cases. With respect to family caregivers of individuals with CNCD, upon revising their level of knowledge and access to ICTs by gender, we found better level of access and knowledge in men. In this respect, literature has indicated that ICTs that would support women permitting greater access to information in homes where most of these individuals spend more time than men while engaged in tasks identified with the female role, are not as used by women as they are by men(25). Studies carried out in Mexico, Chile, Panama, the Dominican Republic, and Uruguay indicate that except for Panama, the countries in the study show differences in internet use that favors men; differences that are accentuated when ICTs are restricted to using computers. According to the analysis of these studies, the indicators of internet use that are better for women in countries with low indices of ICT use, are not maintained in countries that have reached high levels of access and use of ICTs, suggesting foresight with public policies of equity(26, 27).
This study shows that upon analyzing the use of ICT with age, in all age groups of individuals with CNCD the low knowledge and low level of access to ICTs prevail, except for the group of young adults from 18 to 35 years of age where knowledge and high, medium, and low access are divided into close percentages.
The family caregivers of individuals with CNCD, in turn, revealed better levels of knowledge the younger they were, while regarding access, it was adults, especially those between 18 to 35 years of age who reported better access.
In the case of schooling, family caregivers, as well as individuals with CNCD show that the higher educational level will represent higher levels of knowledge of ICT, except in the group with graduate education. This tendency is repeated including graduate studies in optimal access to ICT that caregivers report with some small fluctuation between the group with complete primary education and the group with incomplete high school education. The educational level reached by individuals with CNCD and their relationship to their knowledge of and access to ICTs was previously documented in similar manner(28). These findings are also similar to those reported in prior studies of family caregivers of individuals with CNCD(9).
The low level of access and knowledge reported by individuals with CNCD and by their caregivers can reflect that individuals with CNCD can be excluded from using ICTs especially because of difficulties for displacement or because they require extremely costly adaptations that are not being met, as has been documented in the case of individuals with disabilities(29). Also, it could mean that if the peculiarities of individuals with illnesses were considered, ICTs could be fundamental support(30).
The findings of knowledge and access to ICT by regions in Colombia again evidence that although ICTs open possibilities, they pose an enormous risk of further broadening the gaps already existing in society. It is evident that, according to official data, the border regions on the Pacific, Caribbean, the Colombian Amazon and Orinoquia have less possibilities of access to internet than the Andean region. Although the data on the Pacific region should be revised in greater detail because they are higher than data from other border regions, it is fitting to indicate that it turns out attractive that the Frontiers for Prosperity Plan (Plan Fronteras para la Prosperidad) does not consider regions like the insular Caribbean or prioritizes connectivity as one of its central strategies if we consider that it can be a promising strategy for innovation and education in healthcare. In this regard, experiences have been vastly documented with health professionals for their training with internet(31,32), health technology programs(33), programs with ICT in dentistry(34), use of ICT in basic assignments(35) and e-learning, where the pedagogical, technological, and organizational aspects must be joined to achieve social transformation(36). Information and communication technologies have also been successfully employed to prevent sexually transmitted diseases(37), support diabetic patients(38), and for the willingness of health professionals to support patients with CNCD(39).
In administration where although these tools modify processes and open possibilities for more effective management, they are essential for both training and for follow up in their use(40).
We cannot forget the ethical problems this study evidenced and which are the motive for global controversy. For example, from innovation in ICTs and their greater use, emerge new dilemmas related to the individualist perspective like the misinterpretation of ethical and moral values at the global level that include a serious commitment to the management of knowledge and of the individual's creativity. Information and communication technologies have already created cultural barriers, distancing further the different social levels and the possibility of development according to the access to information(41). In case of individuals with CNCD and of their caregivers, preservation of the right to privacy that demands the revision and regulation of access to data bases that contain information that can compromise the lives of the individuals and, which until now, have not been sufficiently addressed, is obligatory(42). The lack of quality guarantees on the information available in internet is a first-line topic in the world() and although this study did not address it, the strategy to continue with this field should do so.
These findings again raise questions on the impact of ICTs with important risk against the principles of justice and beneficence and challenges to avoid inequality in the distribution of resources for healthcare of individuals with CNCD, their family caregivers, without forgetting, as mentioned previously, that the ultimate purpose of these services must be the wellbeing and quality of life of users(44, 45).
Conclusions
Information and communication technologies can be a significant tool in caring for individuals with CNCD and in supporting their family caregivers. Knowing their level of access and knowledge in the different regions of the country exposes a heterogeneous panorama that should be considered if the General System of Social Security in Health (SGSSSH) seeks to provide universal coverage. Identifying the levels of knowledge and access to ICTs by individuals with CNCD and of the family caregivers is fundamental to offer effective support in caring for these users.
References
1. Organización Mundial de la Salud. Estadísticas Sanitarias Mundiales 2012. Suiza: WHO graphics OMS; 2012. [ Links ]
2. Águdelo C, De La Hoz F, Mojica M, Eslava J, Robledo R, Cifuentes P, et al. Prioridades de Investigación en Salud en Colombia: Perspectiva de los Investigadores. Rev. salud pública. 2009; 11(2): 301-309. [ Links ]
3. Barrera L, Carrillo G, Chaparro L, Pinto N y Sánchez B. Cuidando a los cuidadores: familiares de personas con enfermedad crónica. Bogotá (Colombia): Editorial Universidad Nacional de Colombia; 2009. [ Links ]
4. Zanetti M. Las enfermedades crónicas no transmisibles y tecnologías en salud. Rev. Latino-Am. Enfermagem. 2011; 19(3): 1-2. [ Links ]
5. Carrillo G, Chaparro L, Barrera L, Pinto N y Sánchez B. El blog como herramienta de soporte social para personas con enfermedad crónica. Ciencia y Enfermería. 2011; 17(3): 137-149. [ Links ]
6. Romero E, Herrera A, Flórez I, Montalvo A. Las TIC y el apoyo social: una respuesta desde enfermería en Cartagena (Colombia). Salud Uninorte. 2010; 26(2): 325-338. [ Links ]
7. Carrillo G, Chaparro L, Barrera L, Pinto N, Sánchez B. Soporte social con el uso de las TIC's para cuidadores familiares de personas con enfermedad crónica. Revista de Salud Pública. 2011; 13(3): 446-457. [ Links ]
8. Romero E, Flórez I, Montalvo A. Soporte social con Tecnologías de la Información y la Comunicación a cuidadores: Una experiencia en Cartagena, Colombia. Invest. Educ. Enferm. 2012; 30(1): 55-65. [ Links ]
9. Cárdenas D, Melenge B, Pinilla J, Carrillo G, Chaparro L. Soporte social con el uso de las TIC para cuidadores de personas con enfermedad crónica: un estado del arte. Aquichán. 2010; 10(3): 204-213. [ Links ]
10. Valenzuela J, Camacho J, Argüello A, Cendales J, Fajardo R. Percepciones de los trabajadores del sector salud frente a Internet y las tecnologías móviles en Colombia. Rev. Panam Salud Pública. 2009; 25(4): 367-374. [ Links ]
11. San Miguel B. Las tecnologías de la información y la comunicación en el Espacio Europeo de Educación Superior. Salud Colectiva. 2011; 7(Supl 1): S5-S7. [ Links ]
12. Monteagudo J. Tecnologías de la Información y Comunicaciones. Educación Médica. 2004; 7(Supl 2): S15-S22. [ Links ]
13. Wanden C, Sabucedo L, Martínez I. Investigación virtual en salud: las tecnologías de la información y la comunicación como factor revolucionador en el modo de hacer ciencia. Salud Colectiva. 2011; 7(Supl 1): S29-S38. [ Links ]
14. Llanusa S, Rojo N, Caraballoso M, Capote R, Pérez J. Las tecnologías de información y comunicación y la gestión del conocimiento en el sector salud. Rev Cubana Salud Pública. 2005; 31(3): 223-232. [ Links ]
15. Schiavo E. Investigación científica y tecnológica en el campo de las TIC: ¿conocimientos técnicos, contextuales o transversales? Revista CTS. 2007; 3(9): 91-113. [ Links ]
16. Oddershede A, Carrasco R, Barham E. (2008). Multi-criteria Decision Model for Assessing Health Service Information Technology Network Support Using the Analytic Hierarchy Process. Computación y Sistemas. 2008; 12(2): 173-182. [ Links ]
17. Jardines J. Acceso a la información y equidad en salud. Rev Cubana Salud Pública. 2007; 33(3): 1-8. [ Links ]
18. Castiel L, Álvarez C. Las tecnologías de la información y la comunicación en salud pública: las precariedades del exceso. Rev. Esp. Salud Publica. 2005; 79(3): 331-337. [ Links ]
19. Castiel L, Sanz J. El acceso a la información como determinante social de la salud. Nutr Hosp. 2010; 25(Supl. 3): 26-30. [ Links ]
20. Departamento Administrativo Nacional De Estadística DANE. Tecnología de la información y las comunicaciones. Información 2011. (Citado el 9 de diciembre de 2011) Disponible en http://www.dane.gov.co/index.php?option=com content&view=article&id=10 5&Itemid=61. [ Links ]
21. Gutiérrez De Pineda V. Familia y cultura en Colombia. Tipologías, funciones y dinámica de la familia: Manifestaciones múltiples a través del mosaico cultural y sus estructuras sociales. Vol. 3. Bogotá (Colombia): Instituto Colombiano de Cultura de Biblioteca Básica Colombiana, 1975. [ Links ]
22. Normas científicas, técnicas y administrativas para la investigación en salud. Resolución 8430 de 1993. Ministerio De Salud. Colombia. (4 de Octubre 1993). [ Links ]
23. Política Ambiental de la Universidad Nacional de Colombia. Acuerdo 016 de 2011. Consejo Superior Universitario. (Acta 08 del 18 de octubre de 2011). [ Links ]
24. Ministerio De Comunicaciones. 8 de cada 10 colombianos acceden a internet. (Citado el 15 de febrero de 2013.) Disponible en http://www.mintic.gov.co/index.php/mn-sabia/1908-8-de-cada-10-colombianos-acceden-a-internet. [ Links ]
25. Gargallo A, Esteban L, Perez J. Impact of Gender in Adopting and Using ICTs in Spain. Journal of Technology Management & Innovation. 2010; 5(3): 120-128. [ Links ]
26. Sánchez M. Implicaciones de Género en la Sociedad de la Información: Un Análisis desde los Determinantes de Uso de Internet en Chile y México. Journal of Technology Management & Innovation. 2010; 5(1): 108-126. [ Links ]
27. Sánchez M. ¿Brecha digital, brecha de género? Mujeres y Hombres en América Latina: Panorama Regional de Difusión de Computadora e Internet. Mimeo. Documento del Observatorio de la Sociedad de la Información para Latinoamérica y el Caribe, de la División de Desarrollo Productivo y Empresarial. CEPAL. 2009. [ Links ]
28. Giraldo M, Patiño M. Acercamiento a las estrategias de apropiación de Medellín digital en cuatro comunas de la ciudad: Panorama conceptual y evidencias empíricas. Revista Q. 2009; 3(6): 1-24. [ Links ]
29. De la Fuente Y, Sotomayor E. Las Tecnologías de la Información y Comunicación (TIC) como Instrumento de ejercicio de derechos. Tabula Rasa. 2009: (10): 359-373. [ Links ]
30. Carrillo G, Chaparro L, Barrera L, Pinto N, Sánchez B. El Blog Como Herramienta De Soporte Social Para Personas Con Enfermedad Crónica. Cienc. enferm. 2011; 17(3): 137-149. [ Links ]
31. Weinert C. Social support in cyberspace for women with chronic illness. Rehabil Nurs. 2000;25(4):129-135. [ Links ]
32. Muñoz Serrano M., Cabieses Values B. Vías De Comunicación Preferidas Por Profesionales De La Salud Para Acceder A Programas De Formación Continua En Una Escuela De Enfermería Chilena. Cienc. enferm. 2007; 13(1): 59-68. [ Links ]
33. Rivera A, Viera L, Pulgarón R. La educación virtual, una visión para su implementación en la carrera de Tecnología de la Salud de Pinar del Río. Educ Med Super. 2010; 24(2): 146-154. [ Links ]
34. Ávila R., Samar M. Proyecto Histología Virtual: odontoweb. Int. J. Odontostomat. 2011; 5(1): 13-22. [ Links ]
35. Ramírez Fajardo K., Rivera Michelena N. Uso de las tecnologías de la información y las comunicaciones en la asignatura Morfofisiología Humana I, Programa Nacional de Medicina Integral Comunitaria. Educ Med Super. 2008; 22(3): 1-10. [ Links ]
36. Lupiáñez F. Aspectos claves relacionados con la gestión del eLearning. Educación Médica. 2006; 9(Supl 2): S20-S25. [ Links ]
37. Curioso W, Blas M, Kurth A, Klausner JD. Tecnologías de información y comunicación para la prevención y control de la infección por el VIH y otras ITS. Rev Peru Med Exp Salud Pública. 2007; 24(3):262-271. [ Links ]
38. Curioso W, Gozzer E, Valderrama M, Rodríguez J, Villena J, Villena A. Uso y percepciones hacia las tecnologías de información y comunicación en pacientes con diabetes, en un hospital público del Perú. Rev Peru Med Exp Salud Pública. 2009; 26(2): 161-167. [ Links ]
39. Curioso W, Gozzer E, Rodríguez J. Acceso y uso de las tecnologías de información y comunicación y percepciones hacia un sistema informático para mejorar la adherencia al tratamiento, en médicos endocrinólogos de un hospital público de Perú. Rev Med Hered. 2011; 22(1): 15-22. [ Links ]
40. Belloso N, Perozo M. Asimilación de tecnología de información y comunicación en las alcaldías de Venezuela. Revista de Ciencias Sociales. 2009; 15(1): 139-147. [ Links ]
41. Silva N, Espina J. Ética Informática en la Sociedad de la Información. Revista Venezolana de Gerencia. 2006; (36): 559-579. [ Links ]
42. Rovaletti ML. Derechos humanos, sociedad de la información y sociedad de riesgo. Acta Bioethica. 2010; 16(2): 174-179. [ Links ]
43. Blanco A, Gutiérrez Couto U. Legibilidad de las páginas web sobre salud dirigidas a pacientes y lectores de la población general. Rev Esp Salud Pública. 2002; 76: 321-331. [ Links ]
44. Otero P. Beneficios y riesgos relacionados con el uso de la historia clínica electrónica. Arch. argent. pediatr. 2011; 109(6): 476-477. [ Links ]
45. González M, Herrera O. Bioética y nuevas tecnologías: Telemedicina. Rev Cubana Enfermer. 2007; 23(1): 1-12. [ Links ]

