










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.15 n.42 Murcia Apr. 2016
REVISIONES
Relation of the Glycemic Control, Cognitive Function and Executive Function in the Elderly with Type 2 Diabetes: Systematic Review
Relación del Control Glucémico, Función Cognitiva y las Funciones Ejecutivas en el Adulto Mayor con Diabetes Tipo 2: Revisión Sistemática
Miranda-Félix, Patricia Enedina; Valles-Ortiz, Patricia Magdalena and Ortiz-Félix, Rosario Edith
PhD student, College of Nursing Universidad Autónoma de Nuevo León. E-mail: dulcy84@hotmail.com
ABSTRACT
Objective: To evaluate the available evidence to demonstrate the relationship between glycemic control, cognitive function and executive functions in the Elderly with T2D.
Methods: Based on the model proposed by Cooper (2007) a literature review was conducted in English and Spanish, in 14 databases, Open Access, and the Google search engine. The validity of the studies was assessed through the CASPe a guide for case-control studies.
Results: 11 correlation studies were analyzed all of them demonstrated a relationship between glycemic control, cognitive impairment and executive function in the elderly with T2D. The studies coincide that the elderly with T2D evidence cognitive impairment, compared to the elderly without T2D, therefore that a deficit in the elderly exist to carry out executive functions.
Conclusions: Based on the available evidence there is a significant relationship in glycemic control and cognitive impairment in the AM with DT2, also a lower performance in functional mobility and verbal fluency.
Key words: Executive function; type 2 diabetes mellitus; aging; glycemic control; memory; cognition.
RESUMEN
Objetivo: Revisar la evidencia disponible que demuestre la relación que existe entre el control glucémico, función cognitiva y las funciones ejecutivas en el AM con DT2.
Métodos: La búsqueda de la literatura se realizó en idioma inglés y español, en 14 bases de datos, Open acces, y en el buscador Google. En base al modelo propuesto por Cooper (2007), para la síntesis de la literatura. Los estudios fueron evaluados para su validez, a través de la guía CASPe para estudios de casos y controles.
Resultados: Se analizaron 11 estudios de correlación, el 100% de los estudios mostró relación del control glucémico con el deterioro cognitivo y la función ejecutiva en AM con DT2. Los estudios concuerdan que los AM con DT2 presentan deterioro cognitivo, comparado con los AM sin DT2, por lo tanto existe déficit en el AM al realizar las funciones ejecutivas.
Conclusiones: Según la evidencia disponible existe una relación significativa en el control glucémico y el deterioro cognitivo en el AM con DT2, así mismo un menor desempeño en la movilidad funcional y la fluidez verbal.
Palabras clave: Función ejecutiva; diabetes mellitus tipo 2; Envejecimiento; Control glucémico; memoria; cognición.
Introduction
Type 2 diabetes (T2D) has become a public health problem for the Elderly due to the high prevalence, it is one of the most common diseases in this age group. In Mexico, affects the 19.2% of adults aged 60-69 years, its prevalence increases with age, at 75 years old, approximately 20% of the population suffers T2D and 44% are over 65 years (1). The T2D is a multiple etiology syndrome, produced by the lack of insulin and/or the inability of the hormone to perform its effects properly, which leads to the development of associated diseases and complications such as retinopathy, nephropathy, neuropathy, loss of joint mobility and muscle strength. In addition, cognitive function also seems to be involved in the elderly with T2D.
The evidence shows that the elderly with T2D, is more likely to have cognitive impairment due to structural and functional changes in the central nervous system (CNS), resulting from the aging process, cortical and subcortical structures can undergo additional changes due to changes in metabolism associated with T2D (3,4). It has been reported that cognitive impairment is inversely related to levels of type 1 insulin growth factor (IGF-1) in the elderly, an endogenous peptide with multiple effects on neuronal cells with neurotrophic responses, is involved in many processes that maintain brain homeostasis, so their presence at appropriate concentrations influences brain function (5,6).
There is evidence of their participation in neuronal maintenance, energy metabolism, neurogenesis and regulation of neurotransmitters; It is also involved in neuronal function processes as long-term memory and other cognitive activities (7,8).
The cognitive impairment probably limits the most complex processes, directly related to the frontal lobe, as executive function, which involves a set of cognitive skills, attention, working memory, monitoring, flexibility, inhibition, organization, decision making and knowledge, which controls the performance of complex activities, in the context of T2D this can influence to solve problems in the daily management of their condition, working memory, and planning (3,9). In addition, cognitive impairment can potentially present new obstacles to personal care and to achieve glycemic control.
In many daily life activities, people need to perform more than one task at the same time, like walking or to communicate with others. Cognitive impairment during the execution of a double task, can be an important indicator of the functional state of the elderly with T2D. When two tasks running simultaneously, the performance of one or both can be decreased. The double task often involves both verbal and visual information, the performance of simultaneous tasks is complex and this could lead to a deficit in the management of glycemic control (14,15).
For the above mentioned, the approach in this review are glycemic control, cognitive function and executive functions, with the purpose of reviewing the available evidence showing the relationship between glycemic control, cognitive function and executive functions in the elderly with T2D.
Methodology
A literature review was performed based on the seven steps of Cooper (16): 1) problem formulation, 2) literature search, 3) gather information studies, 4) evaluation of the quality of studies, 5) analyze and integrate the results, 6) interpret the evidence and 7) present the results.
In the first step the variables of the study were defined: executive function, cognitive function, glycemic control. Then a search to identify systematic reviews or assessment reports was conducted in the Cochrane Library, and the following databases Centre for Reviews and Dissemination, Anual review, Dialnet, DynaMed, Medic Latina, Medline Ovid, MEDLINE with Full Text, CINAHL with full text, Embase, Psyc artcicles, Elsevier, Global issues incontext, Academic search complete, Evidence-based Practice Centers, Medline Plus, PubMed, The Campbell Collaboration, Open acces, and Google.
Combinations of the keywords: executive function, diabetes, elderly, Blood Glucose Self-Monitoring, attention, memory, cognition according to the Medical Suject Headings (MeSH) were used, in English and Spanish. Also a manual search was performed based on the reference lists of the review articles and additional potentially eligible studies, from October to November 2012. Boolean operators (AND, OR and NOT) were used for MEDLINE and EMBASE bases, truncation and wildcards ($, ", *, #) according to the chapter 6.4 of Cochrane search strategy were used (17).
Were included in the review cross-sectional studies expressed glycemic control relationship with the executive functions in participants >65 years of age with T2D, and were excluded those studies in which participants were dementia-related diagnoses.
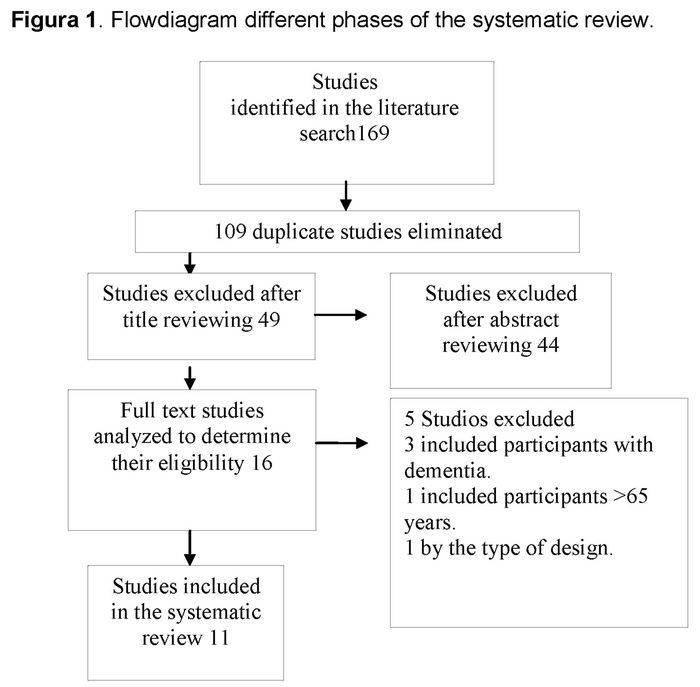
To select the articles to include in the review, at first the abstract was review to identify studies that met the criteria established. Then a full text reading was done, quality and risk of bias through its internal validity was assessed, it took into account the design type, sampling, sample size, reliability instruments, congruence of objective and the statistical used and results, a CASPe Guide (18) was also used to evaluate the study case and controls, which consists of 11 questions, the first two are for elimination, if the answer to those two questions was yes will continue with the remaining questions, otherwise the study was removed, the response options are: yes, no, I do not know.
The question number 3 of the CASPe (18) guide was removed because the evaluated studies do not have enough information to be answered, and it does not provide additional information about the quality of the studies evaluated at this stage, some studies were eliminated because of lack of methodological quality, that results reports little consistency with the proposed objectives. The following diagram shows the process of selection of studies during the phases of the review. (19)
Results
The studies analyzed (2,20-29) who met the inclusion criteria for this review was eleven, the characteristics are presented in Table 1. The number of participants with DT2 in the studies ranged from 1398 to 40 participants per study.


The results of this systematic review provide evidence of the transverse, longitudinal and case-control studies demonstrate relationship of glycemic control, cognitive function and executive functions in the elderly with T2D. Moreover, these results reveal the impact of cognitive impairment in development of the executive functions of the elderly with T2D. Studies evidence that glucose levels causes a cognitive impairment. In addition, the cognitive impairment is associated with a deficit in care activities which affects glycemic control (21). However, other studies showed that cognitive capacity affects the ability of individuals to carry out the glycemic control, and poor glycemic control in turn impairs cognitive function, especially in diet and exercise (21,22,24,28,29).
Also it was found that glucose levels are associated with cognitive function and impaired executive function, on the contrary, in people without T2D, there is not a clear association between baseline levels of fasting glucose, executive function and memory, there was no relationship at high levels of glucose (2,22,23,28). Similarly T2D is associated with performance in delayed recall but not immediate recall. T2D was associated with cognitive impairment and verbal fluency test, they found that poor glycemic control is associated with alterations in performance composite measures (double tasks) and activities of daily living of executive function (2,22,29). Table 1 shows the relationship of the variables of the studies analyzed in this review.
Discussion
The projected increase in T2D and the deterioration in cognitive function of the elderly represent a major public health problem to the society (30,31).
The results suggest a complex association between cognitive function and glycemic control in this population. This review of 11 studies demonstrate the idea that executive function will harm the T2D related to knowledge and later self-care behaviors, interfering with glycemic control. In addition, self-care is a central component to achieve glycemic control, current data suggest that impaired executive function may interfere with the ability of older adults to perform functions of daily living and related T2D care (31)
It has been demonstrated that executive function may endanger the care capacity to perform activities of daily living, develop complex tasks necessary for self-care, such as controlling blood glucose and insulin, medication, diet modification and physical activity (3,21).
Conclusion
Although executive function may be related to glycemic control, understanding the mechanisms of such an association it is limited. These results confirm previous observations, this review suggests continue examining the findings that explain the positive and negative relationship of executive function on glycemic control, it is considered necessary to conduct additional research to identify that at what period of time from the diagnosed in the elderly with T2D occurs deterioration in cognitive function, and develop interventions that allow to examine in greater depth if the age or the T2D is the cause of limiting to carry out the executive functions in the elderly.
Received: May 23, 2015;
Accepted: July 22, 2015
References
1. Encuesta Nacional de Salud (ENSANUT), (2006). Promoción de Estilos de vida Saludables. Recuperado en http://www.insp.mx/ensanut/ensanut2006.pdf. [ Links ]
2. Alvarenga P, Pereira D, Anjos D. Mobilidade funcional e função executiva em idosos diabéticos e não diabéticos. / Functional mobility and executive function in elderly diabetics and non-diabetics. Brazilian Journal Of Physical Therapy / Revista Brasileira De Fisioterapia (serial on the Internet). (2010, Nov), (cited November 18, 2012); 14(6): 491-496. [ Links ]
3. Papazian, O., Alfonso, I. & Luzondo, R. J. Trastornos de las funciones ejecutivas. Simposio de trastornos del desarrollo. Revista de Neurología, (2006), (cited Noviembre 28, 2012) (2006). 42(3), 45-50. [ Links ]
4. Unger JW, Livingston JN, Moss AM. Insulin receptors in the central nervous system: localization, signalling mechanisms and functional aspects. Prog Neurobiol 1991;36:343-362 [ Links ]
5. Isaksson O, Ohlsson C, Nilsson A, et al. Regulation of cartilage growth by growth hormone and insulin-like growth factor I. Pediatr. Nephrol. 1991; 5: 451-453. [ Links ]
6. Trejo J, Carro E, Lopez-Lopez C, Torres-Aleman I. Role of serum insulin-like growth factor I in mammalian brain aging, Growth Hormone & IGF Res 2004;14 (Suppl. A):S39-S43. [ Links ]
7. Craft S, Watson GS. Insulin and neurodegenerative disease: shared and specific mechanisms. Lancet Neurol 2004;3:169-178. [ Links ]
8. Carro E, Trejo JL, Gerber A, et al. Therapeutic actions of insulin-like growth factor I on APP/PS2 mice with severe brain amyloidosis. Neurobiol Aging 2006; 27:1250-1257. [ Links ]
9. Abbatecola AM, Paolisso G, Lamponi M, et al. Insulin resistance and executive dysfunction in older persons. Journal of the American Geriatrics Society 2004; 52:1713-1718. [ Links ]
10. Heisler, M., Vijan, S., Anderson, R. M., Ubel, P. A., Bernstein, S. J., & Hofer, T. P. (2003). When do patients and their physicians agree on diabetes treatment goals and strategies, and what difference does it make? Journal of General Internal Medicine, 18, 893-902. [ Links ]
11. Krapek, K., King, K., Warren, S. S., George, K. G., Caputo, D. A., Mihelich, K., et al. (2004). Medication adherence and associated hemoglobin A1c in type 2 diabetes. Annals of Pharmacotherapy, 38, 1357-1362. [ Links ]
12. Pladevall, M., Williams, L. K., Potts, L. A., Divine, G., Xi, H., & Lafata, J. E. (2004). Clinical outcomes and adherence to medications measured by claims data in patients with diabetes. Diabetes Care, 27, 2800-2805. [ Links ]
13. Skaer, T. L., Sclar, D. A., Markowski, D. J., & Won, J. K. (1993). Effect of value-added utilities on prescription refill compliance and Medicaid health care expenditures-a study of patients with non-insulin-dependent diabetes mellitus. Journal of Clinical Pharmacy Therapeutics, 18, 295-299. [ Links ]
14. Thabit H, Kennelly S, Bhagarva A, Ogunlewe M, McCormack P, Sreenan S, et al. Utilization of Frontal Assessment Battery and Executive Interview 25 in assessing for dysexecutive syndrome and its association with diabetes self-care in elderly patients with type 2 diabetes mellitus. Diabetes Research & Clinical Practice (serial on the Internet). (2009, Dec), (cited November 18, 2012); 86(3): 208-212. [ Links ]
15. Biessels GJ, ter Braak E, Erkelens D, Hijman R.Cognitive function in patients with type 2 diabetes mellitus. Neurosci Res Commun 2001;28:11-22. [ Links ]
16. Cooper H. Research Synthesis and Meta-Analysis. A Step- by -Step Approach. SAGE. 4th ed. Loa Angeles (2009). (Cited Noviembre 2012); 2, 115-144. [ Links ]
17. Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration, 2011. (cited November 18, 2012). Available from. www.cochrane-handbook.org. [ Links ]
18. Guías CASPe de Lectura Crítica de la Literatura Médica. CASPe, D.L.: A-516-2005, editors. Cuaderno I. 2008. [ Links ]
19. Urrútia G, Bonfill X. PRISMA declaration: a proposal to improve the publication of systematic reviews and meta-analyses. Medicina Clínica (serial on the Internet). (2010, Oct 9), (cited November 19, 2012); 135(11): 507-511. [ Links ]
20. Feil D, Zhu C, Sultzer D. The relationship between cognitive impairment and diabetes self-management in a population-based community sample of older adults with Type 2 diabetes. Journal Of Behavioral Medicine (serial on the Internet). (2012, Apr), (cited November 18, 2012); 35(2): 190-199. [ Links ]
21. Munshi M, Hayes M, Iwata I, Lee Y, Weinger K. Which aspects of executive dysfunction influence ability to manage diabetes in older adults? Diabetic Medicine (serial on the Internet). (2012, Sep), (cited November 18, 2012); 29(9): 1171-1177. [ Links ]
22. Anagawa M, Umegaki H, Uno T, Oyun K, Kawano N, Sato Y, et al. Association between improvements in insulin resistance and changes in cognitive function in elderly diabetic patients with normal cognitive function. Geriatrics & Gerontology International (serial on the Internet). (2011, July), (cited November 18, 2012); 11(3): 341-347. [ Links ]
23. Nguyen H, Grzywacz J, Arcury T, Chapman C, Kirk J, Quandt S, et al. Linking glycemic control and executive function in rural older adults with diabetes mellitus. Journal Of The American Geriatrics Society (serial on the Internet). (2010, June), (cited November 18, 2012); 58(6): 1123-1127. [ Links ]
24. Euser S, Sattar N, Witteman J, Bollen E, Sijbrands E, Westendorp R, et al. A prospective analysis of elevated fasting glucose levels and cognitive function in older people: results from PROSPER and the Rotterdam Study. Diabetes (serial on the Internet). (2010, July), (cited November 18, 2012); 59(7): 1601-1607. [ Links ]
25. Munshi M, Grande L, Hayes M, Ayres D, Suhl E, Weinger K, et al. Cognitive dysfunction is associated with poor diabetes control in older adults. Diabetes Care (serial on the Internet). (2006, Aug), (cited November 19, 2012); 29(8): 1794-1799. [ Links ]
26. Van Harten B, Oosterman J, Muslimmovic D, Van Loon B, Scheltens P, Weinstein H. Cognitive impairment and MRI correlates in the elderly patients with type 2 diabetes mellitus. Age & Ageing (serial on the Internet). (2007, Mar), (cited November 18, 2012); 36(2): 164-170. [ Links ]
27. Hagemann R, Sartory G, Hader C, Kobberling J. Mood and cognitive function in elderly diabetic patients living in care facilities. Dementia And Geriatric Cognitive Disorders (serial on the Internet). (2005), (cited November 18, 2012); 19(5-6): 369-375. [ Links ]
28. Debling D, Amelang M, Hasselbach P, Stürmer T. Diabetes and cognitive function in a population-based study of elderly women and men. Journal Of Diabetes And Its Complications (serial on the Internet). (2006, July), (cited November 18, 2012); 20(4): 238-245. [ Links ]
29. Mogi N, Umegaki H, Hattori A, Maeda N, Miura H, Iguchi A, et al. Cognitive function in Japanese elderly with type 2 diabetes mellitus. Journal Of Diabetes And Its Complications (serial on the Internet). (2004, Jan), (cited November 19, 2012); 18(1): 42-46. [ Links ]
30. María Fernandes-Lopes R, DE Lima-Argimon I. Idosos com diabetes mellitus tipo 2 e o desempenho cognitivo no teste Wisconsin de classificação de cartas (WCST). Universitas Psychologica (serial on the Internet). (2010, Sep), (cited November 18, 2012); 9(3): 697-713. [ Links ]
31. Bell RA, Smith SL, Arcury TA, et al. Prevalence and correlates of depressive symptoms among rural older African Americans, Native Americans, and whites with diabetes. Diabetes Care 2005; 28:823-829. [ Links ]
32. Glasgow RE, Fisher L, Skaff M, et al. Problem solving and diabetes self-management Investigation in a large, multiracial sample. Diabetes Care 2007; 30:33-37. [ Links ]

