










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.15 no.43 Murcia jul. 2016
ADMINISTRACIÓN-GESTIÓN-CALIDAD
Indicators of care in a surgical clinic
Indicadores de asistencia en un clínica quirúrgica
Indicadores de assistência em uma clínica cirúrgica
Paranaguá, Thatianny Tanferri de Brito*; Bezerra, Ana Lúcia Queiroz**; Moreira, Isadora Alves***; Tobias, Gabriela Camargo**** and Silva, Ana Elisa Bauer de Camargo e*****
*Phd. Assistant Professor of Health Sciences of the University of Brasilia. E-mail: ttb.paranagua@gmail.com
**Phd. Associate Professor of Nursing School of the Federal University of Goiás.
***Nurse University Hospital of Brasilia.
**** Master in Nursing, Nursing School of the Federal University of Goiás.
*****Phd. Assistant Professor of Nursing School of the Federal University of Goiás. Brazil.
ABSTRACT
This study aimed to characterize the hospitalizations occurred in the Surgical Clinic of a university hospital in the Midwest of Brazil. Descriptive, retrospective, cross-sectional study, carried out based on medical records for a total of 750 admissions. Collection of data took place from January to May of 2011 with aid of a structured and validated instrument. Descriptive statistical analyses were carried out. It was found that most admissions were elective (82.1%), with length of stay between two and eight days for 82.2% admissions. At least one surgery was recorded in 85.9% of the hospitalizations and doctors were professionals with high participation in the evolution of the patient, while the nurse presented evaluation record in 19.2% of the admissions. This highlights the need for professionals to rethink their actions in the health care and for the institutions to perform the systematization of the process of evaluation of clinical indicators, searching for quality and safety of the patient in the clinical practice.
Key words: Quality Assessment Assistance; Process indicators, surgical patient care, nursing.
RESUMEN
Se objetivó caracterizar las hospitalizaciones ocurridas en la Clínica Quirúrgica de un hospital universitario del Centro Oeste de Brasil. Estudio descriptivo, retrospectivo, transversal, realizado a través de los registros en un total de 750 admisiones. La colecta fue de enero a mayo de 2011, con instrumento estructurado y validado. Se realizó análisis estadístico descriptivo. Se encontró que la mayoría de los ingresos fue electiva (82,1%), con duración de la estancia hospitalaria entre dos y ocho días para el 82,2% de los ingresos. Al menos una intervención quirúrgica se registró en 85,9% de las hospitalizaciones y los médicos fueron los profesionales con una mayor participación en la evolución del paciente, mientras que la enfermera presentó registro de evaluación en 19,2% de las hospitalizaciones. Destaca la necesidad de los profesionales de repensar sus acciones a través de la atención de la salud y que las instituciones realicen la sistematización del proceso de evaluación de los indicadores clínicos en busca de la calidad y seguridad del paciente en la práctica clínica.
Palabras clave: Evaluación de la calidad asistencial; Indicadores de proceso; atención al paciente quirúrgico; enfermería.
RESUMO
Este objetivou caracterizar as internações ocorridas na Clínica Cirúrgica de um hospital universitário do Centro Oeste do Brasil. Estudo descritivo, retrospectivo, de delineamento transversal, realizado por meio de prontuários em um total de 750 internações. A coleta foi de janeiro a maio do ano de 2011, com instrumento estruturado e validado. Realizada análise estatística descritiva. Constatou-se que a maioria das admissões foi eletiva (82,1%), com tempo de internação entre dois e oito dias para 82,2% das internações. Pelo menos uma intervenção cirúrgica foi registrada em 85,9% das internações e os médicos foram os profissionais com maior participação na evolução do paciente, enquanto que o enfermeiro apresentou registro de avaliação em 19,2% das internações. Evidencia-se a necessidade dos profissionais repensarem suas ações frente ao cuidado em saúde e que as instituições realizem a sistematização do processo de avaliação dos indicadores da assistência, em busca de qualidade e segurança do paciente na prática clínica.
Palavras chave: Avaliação da Qualidade da Assistência; Indicadores de processo, Assistência do paciente cirúrgico, Enfermagem.
Introduction
The quality of health services and safety of the patient has been a constant concern of the institutions that provide care and of the academia, as unplanned assistance may result in considerable damage.
This issue, specifically in Brazil, became relevant because of the increased volume of surgical admissions, with an estimated incidence of three million annual hospitalizations for this purpose(1). In turn, the World Health Organization (WHO) estimates that about 234 million surgeries are performed worldwide per year, and due to this high rate of surgeries, it is important to evaluate the care provided to the patient in the perioperative period(2).
In the context of surgical care, the study of the profile of admissions becomes relevant due to the complexity of care provided to various specialties of treatment, the need for specialized knowledge, the turnover of admissions and technological arsenal necessary for a safe and highly qualified intervention(3).
Study in a surgical clinic of a university hospital pointed to the occurrence of 6,981 incidents arising from health care, which were attributed to a poorly planned assistance and the processes that need to be reviewed and that should be based on the characteristics of the patients(4).
The evaluation of the hospitalized patient is the most accurate and effective way to diagnose, in early stages, aspects that may affect the outcome of the surgical procedure. Clinical examination should be as complete as possible through anamnesis, physical assessment and the results of preoperative tests that are always recommended, in order to support surgery, the anesthetic process, and to raise the patient's prognosis(4,5).
Currently, health services face many challenges to meet the demands of clients and their families with a view to excellence of quality of care. To achieve this excellence, health professionals must assume a work process focused on continuous improvement, encouraging the constant identification of intervening factors of care and the development of instruments that allow to systematically evaluate the quality levels provided(6).
In the theory proposed by Donabedian, it is possible to make a systematic assessment of care through the use of process indicators that allow quantitatively and qualitatively evaluate the results of the assistance provided, and thus evaluate the quality, productivity and the impact of services in population health, representing thus an important tool for management(7,8).
The indicators are the main flags of an organization, because they allow identifying the occurrence of possible deviations in processes that are considered normal, giving evidence of the need for revisions and preventing the continuation of the problem. Thus, interconnect strategies, resources and organizational processes of health care units(7).
An important point in the evaluation of the quality of care is the profile of assisted clients in inpatient units and the dynamics of activities because they provide information that support the organization and planning of assistance in accordance with customer requirements, the size of the nursing staff, the provision of material resources and the measurement of costs(6,7).
From this perspective, the importance of keeping the record of the assistance provided to the patient is evident. This gives ethical and legal support to the patient and the professional responsible for care, and establishes a more effective communication within the staff, which facilitates the evaluation of the quality of services provided. Sparse and inadequate records compromise the planning of actions for providing individualized care with quality and safety, in addition to posing a barrier to the measurement of results of the care provided(9).
Thus, in order to reduce the possible risks of surgery, care should be planned according to the individuality of each patient, based on scientific evidence and determined by the clinical condition of the patient (10), making it important to characterize these indicators.
Therefore, when considering the care and management activities of nurses, these assume an essential role in success of assessment of hospitalization unit where they work. Based on these results, strategic actions should be undertaken, as well as threats should be identified and plans of assistance, management, research, education must be developed in order to, finally, direct a decision-making aimed at the excellence of care to surgical patients(3,4).
In this context, the objective of this study is to characterize the hospitalizations occurred in surgical clinic of a hospital, once that learning and analyzing the factors related to admissions make possible to improve to facing of challenges that guide the quality and safety in health care.
Method
Retrospective, cross-sectional study conducted at the Surgical Clinic of a hospital in the municipality of Goiânia, Goiás.
The study population was composed of patients hospitalized between January and December 2010, with the medical records of 2,610 admissions that took place during this period used as data source. The sample consisted of 750 hospitalizations, considering precision of 2.5%, 1.5 drawing effect, 95% confidence interval, and prevalence of 10% of adverse events estimated by the WHO. Probabilistic and systematic sampling was used.
Data collection took place from January to May of 2011 in the Medical Information and Archive Service of the Health institution. Data collection was guided by a structured form with objective questions about patient characteristics and admissions. The form was built by the researchers themselves, subjected to evaluation by experts and subjected to a pilot test.
Data were structured in Software Statistical Package for Social Science version 20.0 for Windows. A descriptive analysis was performed, to show the difference of proportions for categorical variables and differences of means for continuous variables.
The study is linked to the project: "Analysis of occurrences of adverse events in a hospital of the Sentinel Network of the West Region", approved by the Research Ethics Committee under Protocol No 064/2008.
Results
A total of 750 admissions were analyzed corresponding to 28.7% of all hospitalizations in the Surgical Clinic of the institution during 2010. The characterization of hospitalized patients is presented in Table 1.

The female gender was predominant with 449 (59.9%) patients and the age varied from two to 96 years, with an average of 46.9 years. Among the patients, 312 (41.6%) had other pathology beyond the disease that resulted in hospitalization. It is noteworthy that in 22 (2.9%) records, the information on the presence of comorbidities were absent.
The total length of stay ranged from one to 97 days and elective hospitalizations occurred in 616 (82.1%) cases, particularly for the specialties of general surgery, with 138 cases (18.4%), urology with 101 (13.5%), otolaryngology with 100 (13.5%) and gynecology with 97 (12.9%).

A total of 680 surgeries without interventions were carried out in 644 (85.9%) patients, corresponding to a mean of 1.1 surgeries per hospitalization. During the perioperative period, the use of multiple devices was necessary, especially the catheter was installed in 680 (90.7%) patients.
The characteristics of surgeries performed during hospitalization, are presented in Table 3.
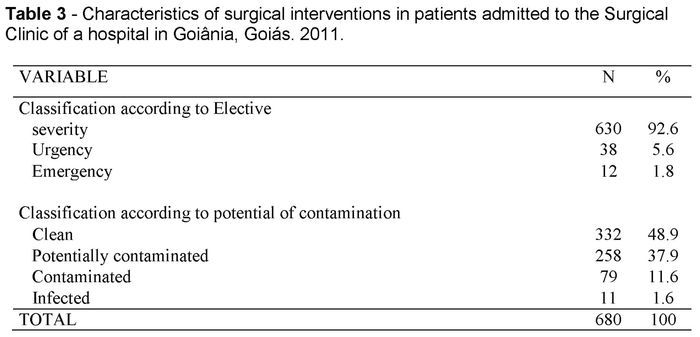
As for the severity, elective surgery was prevalent for 630 (92.6%) surgeries, and clean surgical interventions and potential contamination corresponded to 332 (48.9%) surgeries, followed by potentially contaminated surgery with 258 (37.9%).
The types of clinical assessments performed by the health staff and identified in the records during hospitalizations are described in Table 4.

Among the 750 admissions, 220 (29.3%) of them were lacking the daily evolution of the clinical frame of the patient, as the daily record of the evolution sheet of 530 (70.7%) admissions had at least one clinic assessment conducted by professional with superior level.
Medicine was the most participatory professional category in the record of the clinical evolution of the client, with 673 (89.7%) admissions showing at least one evaluation during the period of hospitalization in the surgical clinic.
With respect to the registration of the nursing team, the evaluation of the patient by the nurse was performed in only 144 (19.2%) hospitalizations. Among the remaining 606 hospitalizations, notes were recorded only in the admission date unit for 407 (67.2%) cases an these were related to the medical expertise. As for the care provided by nursing assistants and technicians, records were found in all admissions, but were limited to basic information and common to all patients.
It was found also that among the 644 (85.9%) admissions that underwent surgery, daily evolution of the wound was recorded in 184 (24.5%) cases.
Discussion
The evaluation of quality of care is a form of control of all health service processes aimed at meeting the needs of both patients and their families. For this, we need to set measurement parameters, deploy and establish indicators of quality(7).
The medical records are a form of multidisciplinary written communication, and although with underreporting, they are considered the gold standard method for this type of research because, they serve to keep the greater number of information possible on the health status of patients. They set base for the development of a care plan and, therefore, for the evaluation of the quality of services(3,9).
As the notes in the records are the result of the service offered to the patient during hospitalization, it is essential that this information be complete and able to disclose, clearly, the care provided, history, evolution and continuity of customer service(3,4,9).
According to the results, there are gaps in the records, calling attention to 29.3% hospitalizations that were not daily evolved for the patient's condition. This is a predisposing factor for the occurrence of errors. Some factors may influence the realization and the quality of nursing records. High demand for services, work overload, insufficient number of professionals, continuing education deficit, lack of motivation related to poor working conditions, low wages, low social educational level, complexity of language and ineffective communication within the team are some examples(11).
By the same token, the absence of information on comorbidities of patients in 2.9% of records makes it difficult to distinguish pre-existing conditions in the patient and this prompts the occurrence of complications during care(7).
The low rate of participation of nurses in direct patient care is a fact evidenced in other studies(12,13). It is important to note that during the evaluation of nursing, the nurse is the professional responsible for the process and coordination of patient care in an individualized and complete manner(14).
The quality of records is entitled to a number of functions determined by regulators of each profession, in addition to the institutional rules of each company, and especially the commitment and ethical responsibility of nurses with the professional practice (15) Another important aspect, because this is a surgical unit of a hospital, is the absence of surgical wound evolution in the records.
Alarming rates are shown in other studies. One study found that only 15.4% of surgical wounds were recorded by nursing staff, confirming the flaws in this issue, that is, appearance and evolution of skin lesions(16). This reality points to divergences between the theory and the practice of the care process to surgical patients. As a result, studies show that among the most frequent surgical adverse events are those related to surgical wounds, including infection(1).
The evaluation and record of wound evolution is an essential factor in determining the specific treatment for each case. Hence, this should be done systematically and thoroughly, from the onset of the injury until the resolution of it(16.17).
The results also showed that various procedures and devices have been used by patients to help and to continue the assistance.
Among the procedures, drug prescription occurred in 98% of admissions which is expected once that this is essential to the health recovery process, especially in the postoperative period. However, attention should be paid to the amount and administration of these drugs in order to avoid failures in the process, taking into account that surgical clinic is among the units with higher rates of error related to the care, particularly errors involving the medication process(11).
Surgery occurred in 85.9% hospitalizations and these were predominantly elective. This situation minimizes the risks of surgery, as favors the planning of individualized care in compliance with the particularities of each patient's health status, the surgery characteristics and with scientific basis(18).
Antibiotic prophylaxis is a common practice in the preoperative period, an important measure in the prevention against surgical site infection. However, this should be done properly using the guidelines, to ensure greater safety to the patient and, particularly, to prevent bacterial resistance(2).
Given this reality, the WHO introduced a campaign to control the indiscriminate use of antimicrobials in order to minimize the consequences of antimicrobial resistance. This campaign is driven by the World Alliance for Patient Safety, which guides the adherence to quality standards that ensure the reduction of risks of care, contributing to patient safety(19).
Regarding tubular devices, important technologies that aid the assistance, the number of patients using one or more devices is relevant, what increases the complexity of care.
The record of invasive procedures is essential for planning the assistance and also for directing the work in various sectors of the hospital environment that depend on this information, such as the Hospital Infection Control Commission, clinical research, audit services and audit of quality of care, among others(16).
The importance of the retrospective audit process of records as a resource to find out the problems of the care process is evident. Identifying weaknesses can help the development of actions that encourage the attitudinal change of professionals regarding the registration of care, improving the documentary part and, mainly, improving care(4,9).
When the quality of care is the goal to be achieved, this requires major control of the work process by the manager and the health team. Thus, the thorough note of actions taken toward the patient may guide changes in organizational structure, processes and therefore the results of the assistance. Adoption of training and in-service education are some strategies that result in improving the quality of the annotations, and the health care offered(7,10).
Conclusions
A total of 750 admissions were analyzed, with 59.9% of patients corresponding to the female gender and 40.1% to males, with mean age of 46.9 years. It was found that the majority of admissions to Surgical Clinic were elective (82.1%), with length of stay between two and eight days for 82.2% cases.
Drug prescription averaged two drugs per patient/day and was performed in 98% of all hospitalizations.
At least one surgery was recorded in 85.9% of hospitalizations, and antibiotic prophylaxis was performed in 63.1%.
The use of tubular devices was present in all hospitalizations, resulting, in average, in 1.3 devices per patient.
Doctors were professionals with greater participation in the evolution of the patient with record in 89.7% of admissions, while the nurse was present in the evaluation record of 19.2% admissions.
The study found divergences between what is expected for safe care to the patient and the practice in health institutions. The care indicators surveyed can set base for the planning of corrective actions of the health team working process in order to achieve excellence and safety in care.
It is expected that this study arouse self-reflection of healthcare professionals with respect to their actions and encourage health institutions to systematize the process of evaluation of clinical indicators in order to contribute to patient safety, reduce the negative results, and act upon the evidence of clinical practice.
Received: February 5, 2015
Aceppted: April 17, 2015
References
1. Moura MLO, Mendes W. Avaliação de eventos adversos cirúrgicos em hospitais do Rio de Janeiro. Rev. Bras. Epidemiol., 2012;15(3): 523-35. [ Links ]
2. World Health Organization. World alliance for patient safety. Taxonomy. The conceptual framework for the international classification for patient safety. Genève: WHO, 2009. [ Links ]
3. Paranaguá TTB, Bezerra ALQ, Santos ALM, Silva AEBC. Prevalence and factorsassociated with incidents related to medication in surgical patients. Rev Esc Enferm USP, 2014;48(1):41-7. [ Links ]
4. Paranaguá TTB. Análise dos incidentes ocorridos na Clínica Cirúrgica de um hospital universitário da região Centro-Oeste (dissertation). Goiânia: Faculdade de Enfermagem/UFG; 2012. 149p. [ Links ]
5. Santos JS, Kemp R. Fundamentos básicos para a cirurgia e cuidados perioperatórios. Medicina, 2011; 44( 1): 2-17. [ Links ]
6. Sobrinho FM, Ribeiro HCTC, Alves M, Manzo BF, Nunes SMV. Performance em processo de acreditação de hospitais públicos de Minas Gerais/Brasil: influências para a qualidade da assistência. Enfermería Global, 2015; 37: 01-06. [ Links ]
7. Dias AO, Martins EAP, Haddad MCL. Instrumento para avaliação da qualidade do Time de Resposta Rápida em um hospital universitário público. Rev Bras Enferm. 2014;67(5):700-7. [ Links ]
8. Donabedian A. The definition of quality and approaches to its assessment: explorations in quality assessment and monitoring. Chicago: Health Administration Press, 1980. [ Links ]
9. Novaretti MCZ, Santos EV, Quitério LM, Daud-Gallotti RM. Sobrecarga de Trabalho da Enfermagem e incidentes e eventos adversos em Pacientes internados em UTI. Rev. bras. enferm. (online). 2014;67(5):692-9. [ Links ]
10. Vituri DW, Évora YDm. Fidedignidade de indicadores de qualidade do cuidado de enfermagem: testando a concordância e confiabilidade interavaliadores. Rev. Latino-Am. Enfermagem mar.-abr. 2014;22(2):234-40. [ Links ]
11. Magalhães AMM., Dall'agnol CM, Marck PB. Carga de trabalho da equipe de enfermagem e segurança do paciente-estudo com método misto na abordagem ecológica restaurativa. Rev. Latino-Am. Enfermagem, 2013;21(9): 82-9. [ Links ]
12. Penedo RM, Spiri WC. Significado da Sistematização da Assistência de Enfermagem para enfermeiros gerentes. Acta Paul Enferm. 2014;27(1):86-92. [ Links ]
13. Amestoy SC, Backes VMS, Thofehrn MB, Martini JG, Meirelles BHS, Trindade LL. Gerenciamento de conflitos: desafios vivenciados pelos enfermeiros-líderes no ambiente hospitalar. Rev Gaúcha Enferm. 2014;35(2):79-85. [ Links ]
14. Conselho Federal de Enfermagem (COFEN). Resolução COFEn n. 311/2007: código de ética dos profissionais de enfermagem. Rio de Janeiro: COFEN 2007. [ Links ]
15. Barbosa SF, Sportello EF, Mira VL, Melleiro MM, Tronchin DMA. Qualidade dos registros de enfermagem: análise dos prontuários de usuários do programa de assistência domiciliária de um hospital universitário. O mundo da saúde, v. 35, n. 4, p.395-400, 2011. [ Links ]
16. Tavares TS, Castro AS, Figueiredo ARFF, Reis DC. Evaluation of the implementation of the systematic organization of nursing care in a pediatric ward. Rev Min Enferm. 2013;17(2): 287-95. [ Links ]
17. Borsato FG, Rossaneis MA, Haddad MCFL, Vannuchi MTO, Vituri DW. Avaliação da qualidade das anotações de enfermagem em um Hospital Universitário. Acta Paul. Enferm., 2011;24(4): 527-33. [ Links ]
18. Sena AC, Nascimento ERP, Maia ARCR. Prática do enfermeiro no cuidado ao paciente no pré-operatório imediato de cirurgia eletiva. Rev Gaúcha Enferm. 2013;34(3):132-7. [ Links ]
19. World Health Organization. World alliance for patient safety. Guideline safe Surgery. Genève: WHO, 2008. [ Links ]

