










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.16 n.45 Murcia Jan. 2017 Epub Dec 14, 2020
https://dx.doi.org/10.6018/eglobal.16.1.238811
Originales
Evaluation of the patient safety culture within the hospital organization of a university hospital
*Nurse, Master Degree in Nursing by “Escola de Enfermagem Alfredo Pinto/UNIRIO, Responsible for the Permanent and Continuous Education of Hospital Universitário Gaffrée e Guinle/UNIRIO. E-mail: mapepinheiro@gmail.com
**Master in Collective Health IMS/UERJ, Doctor in Nursing/UFRJ, Professor of the Post-Graduation Professional Program of Health and Technology of the Hospital Space/ Universidade Federal do Estado do Rio de Janeiro/UNIRIO. Brazil.
This article has the objective of addressing the assessment of nurse caretakers about the patient safety culture within the hospital organization of a university hospital. It was adopted the descriptive method with quantitative approach with data collected from September to November 2014. The study sample consisted of 203 nurse caretakers who responded to the questionnaire Hospital Survey on Patient Safety Culture (HSOPSC) available at Proqualis, translated into Portuguese. The questionnaire consists of 12 dimensions to evaluate the Safety Culture, the degree of agreement is scored by the scale Likert whose responses vary from "totally agree" to "strongly disagree". In the herein manuscript, we used 3 (three) dimensions of safety culture within an organization. The data indicate that the manager and leaders of the institution need to demonstrate commitment and take concrete actions that favor and prioritize patient safety issues within the study hospital setting.
Keywords Organizational culture; Patient Safety Culture; Risks; Nurse Team
Introduction
Hospital organization is the most complex of the humane organizations. Within the same environment, an array of caretakers of multiple areas, with various bonds, dealing with health and life related issues gather and a slight lapse may trigger a serious damage to the individual under care. Thus, a hospital is a serious daily challenge for all the caretakers working in there (1.
Organizational Culture is a set of objectives, norms, rituals and forms of resolving problems shared by its participants. It is essential for an institution to clearly state what it is expected from their employees, what are the values, policies and rules of the institution. If this is not clear, each individual will determine and follow its own rules 2.
Groups that share the same technological skills, develop the same activities, and socialize are able to develop its own culture. This is why different proprietary cultures from diverse groups interact within the same institution. It is a great challenge to deal with the working processes of these groups as each one is reluctant to accept the proprietary culture of another group as valid or normal 3.
Each member of an organization undergoes an ongoing transformation, interacting and modifying the reality where it acts. Thus, it is a tough task to assimilate the culture of an organization. When this specific universe is evaluated collectively, the culture of an organization, its processes and power relations is absorbed 3.
The primary conception of Safety Organization came up in the decade of 1980 in the wake of the Ukraine Chernobyl incident, later adjusted to conceptualize the Patient Safety Culture as: "the product of individual and group values, attitudes, perceptions, competencies and patterns of behavior that determine the commitment to and the style, and proficiency of an organizational health and safety management. Therefore, "it demands the comprehension of values, beliefs and norms about what is important within an Organization and which patient-related attitudes and beliefs are expected and appropriate"4.
The Agency for Healthcare Research and Quality Careers defines Safety Culture as "the product of individual and group values, attitudes, perceptions, competencies, and patterns of behavior that determine the commitment to, and the style and proficiency of, an organization's health and safety management to promote safety". However, the safety culture of Health Systems is a quite complex phenomenon and its implementation in these systems demands the understanding of seven other subcultures5:
Leadership: the leaders need to acknowledge the high risk that the health environment presents and pursue the alignment of vision, mission, team competence, legal and human resources of professionals that are in the front line of caretaking up to the Board;
Team work: relations should be open, accountable and flexible, and the spirit of camaraderie, cooperation and collaboration among every professional, facing the complexity of the health care should prevail;
Communication: must occur in a clear, structured manner with appropriate techniques of information that are essential to promote the patient safety culture;
Learn with errors: because it open the possibility of pursuing improved performance starting with the leaders and be valued by every professional. Learning culture creates the awareness about safety and promotes an environment that favors opportunities for growing. The process of education and training must emphasize what means to have a highly trustable institution, the worth of the safety culture and the continuous process of performance improvement;
Justice, based in the veracity, because it acknowledges the errors as system flaws in lieu of individual flaws and, at the same time, it does not fail in holding the individuals accountable for their actions;
Patient-driven healthcare that goes beyond the fact that the patient is an active player of its own care, but also a link between the health institution and the community.
Evidence-based practice with its standardized processes designed to reach high reliability and to avoid potential variations in every situation. Health institutions using evidence-based practices, "through protocols, standardized processes, checklist and guidelines show concern in developing safe practices" (5).
The safety patient movement started in the last decade of the twenty century after the publication of the Report (To Err is Human: Building a Safer Health Care System) of the Institute of Medicine (IOM), that presented results of several studies that revealed the critical condition of the healthcare in the United States of America with surprising findings. The report compared the number of deaths to the fall of one Jumbo plane per day, which most likely contributed to shock and draw the attention of the authorities and responsible for healthcare. 6
From then on, WHO adopted the safety patient issue as a high priority theme in the political agenda of its Country Members and launched the Global Alliance for the Patient Safety with the objective of socializing the knowledge and solutions encountered in 2002; international campaigns and programs were created with recommendations to warrant the safety of the patients worldwide. 7
Pursuant to the WHO International Classification for Patient Safety, patient safety "is the reduction of risk of unnecessary harm associated with healthcare to an acceptable minimum" and harm "is the impairment of the structure or body function and/or any deleterious impact arise there from, including the diseases". If this harm or incident is health related, it is an Adverse Event. Thus, Adverse Event is the unintentional injury or harm resulting in permanent or temporary impairment or dysfunction and/or extension of the length of stay or demise as a consequence of the care provided". 8-9
Risk is a world that reflects the relations of the individuals with future events. It is the odds of occurring an adverse event and is associated to the potential of losses and damages and the magnitude of the consequences. 10
The National Health Surveillance Agency (ANVISA) defines risk as "one or more conditions of one variable with potential to cause harm". These harms can be understood as injuries to individuals or are related to equipment, facilities, environment or yet, material losses in the process or reduction of production capacity. 5
In addition to the infinity of risks encountered in the hospital environment, we emphasize the "healthcare risks" or risks caused by health care that may impact the patients under care, their families, the health care professionals and the society as a whole, which justify the movement for the Patient Safety.
James Reason (1990), a British psychologist and important researcher, creator of the "Theory or Model of Swiss Cheese", advocates that the error belongs to the human being and thus we will never extinguish the possibility of making errors. But it is possible to change the environment where humans interact, turning it safer, with designs of systems and methods that hinder errors, avoiding them to cross the multiple and incomplete protection layers (slices of the Swiss cheese) and cause subjacent errors that induced or made the error possible or better, in their root-causes and not simply what happened in the end of the process 11-6.

The processes and systems of a hospital need permanently to adjust and prevent errors. The organization, its managers and leaders, mainly, must encourage and promote a safe environment for patients and healthcare professionals.
While developing their caring activities, the nurses are usually at the front line of care and most likely are the ultimate protective layer against errors, or metaphorically, "the last layer of the Swiss cheese"; it is essential to have an evaluation of nurses about the hospital where they perform their activities.
As aforementioned, the current study has the objective of evaluate the patient safety culture across the dimensions of the hospital organization of a university hospital. Additionally, the study will investigate the evaluation of the hospital organization by the nurse staff and other contributing factors within the organization that may potentially interfere with the patient safety. The Steering Questions were: How the nurse staff evaluates the safety culture within the organizational dimensions of a university hospital? Are there contributing factors within the hospital organization that jeopardize or may hamper the patient safety?
Methodology
Descriptive study with quantitative approach developed at a Public University Hospital located in the city of Rio de Janeiro focused to patients of "Sistema Único de Saúde (SUS)" - Health Single System with 233 beds after authorized by the hospital director. The Institutional Review Board approved the study on August 28, 2014, Report CEP/HUGG number769.099/CAAE 4355354.4.0000.5258, pursuant to the guidelines of Directive 466/2012 of the National Health Council; the participants signed an Informed Consent Form (ICF).
The sample consists of nurse professionals (nurses, residents, technicians and assistants), the inclusion criteria is to be a nurse staff member of the study hospital setting or of the Residence Program for more than six months, and presence in the working environment during the research. The calculation of the sample considered the probability of the event of 50%, with confidence interval of 95% and error type I < 5%; the estimated sample contained 203 subjects in an universe of 424 employees.
The data were collected from September to November 2014, 203 questionnaires have been selected from 300 applied, after reviewing and excluding the participants that did not meet the pre-determined criteria. The tool used was the questionnaire Survey on Patient Safety Culture (HSOPSC), translated into Portuguese available at Proqualis, version validated by Reis (2013) 12. The questionnaire has 12 Dimensions of Safety Culture, seven of which refer to work unit within the hospital, three to hospital organization and two, results measures. For the present article, we used only the seven unit dimensions of work within the hospital; with the calculation of the responses it is possible to identify the "strong areas" related to Patient Safety Culture (when positive responses are > 75%), and "fragile areas" (when responses are < 50%). In relation to the negative responses, if > 50 % for a certain area, more fragile it is.
To describe the sample and endpoints considered (knowledge and evaluation about patient safety culture; contributing factors that interfere with safer practices) univariate analyzes were conducted through simple frequency. The statistical package used was Statistical Package for Social Sciences (SPSS) for Windows, version 17.0.
Results
Tables I, IIand IIIshow the demographics and functions of the study subjects. The sample consists of 203 caretakers, 82.1% women, average age of 44.3 years old and average time in the profession of 14.8 years. About 29.5% work in the hospital from 1 to 5 years, 16.5% from 11 to 15 years and 13.0% less than 1 year. The majority (73.3%) dedicates from 20 to 39 hours in-site and 22.8% more than 40 hours; 27.2.% are nurses, 44.1% are nurse technicians and 26.6%, nurse assistants, about 88.6% state they have direct contact with the patients during care. A total of 35.8% completed high school and 32.9% concluded post-graduation level stricto or lato senso, and 72.2% stated they have joined some educational activity about patient safety.
Table I Distribution of variables: Gender, Age, Literacy or Function of the Research Subjects, Rio de Janeiro (RJ), 2015.
| Variable | Absolute figure | % | |
|---|---|---|---|
| Gender | 1- Female | 165 | 82.09 % |
| 2-Male | 36 | 17.91 % | |
| Edad | 1- 20 a 30 years | 27 | 13.8% |
| 2 -31a 40 years | 50 | 25.6% | |
| 3 -41 a 50 years | 52 | 26.6% | |
| 4 -51 a 60 years | 49 | 25.1% | |
| 5 - Above de 60 years | 17 | 8.7% | |
| Scolarity | 1--Post graduation, Master and Doctorate | 14 | 6.97% |
| 2-Post graduation - Specialization | 52 | 25.87% | |
| 3-College Complete | 27 | 13.43% | |
| 4-College Incomplete | 27 | 13.43% | |
| 5-High School Complete | 72 | 35.82% | |
| 6-High School Incomplete | 06 | 2.99 | |
| 7-Junior School Incomplete | 01 | 0.50% | |
| 8-Junior School Incomplete | 01 | 0.50% | |
| Role | 1-Nurse | 55 | 27.23% |
| 2-Nurse Technician | 89 | 44.06% | |
| 3-Nurse Assistant | 53 | 26.24% | |
| 4-Nurse Resident | 05 | 2.48% |
Table II Distribution of variables: Main Area or Unit in the Hospital and time of work in the institution of the research participants, Rio de Janeiro (RJ), 2015.
| Variable | Absolute figure | % | |
|---|---|---|---|
| Main area or unit in the hospital | 1-Various units/None specific | 14 | 6.9% |
| 2-Medical Clinic | 25 | 12.4% | |
| 3-Clinic - Surgery | 24 | 11.9% | |
| 4-Surgery | 23 | 11.4% | |
| 5-Obstetrics | 23 | 11.4% | |
| 6-Pediatrics | 10 | 4.9% | |
| 7-Neonatology Intensive Care Unit | 09 | 4.4% | |
| 8-Intesive Care Unit - adults | 12 | 5.9% | |
| 9-Ortopedics | 06 | 2.9% | |
| 10-Ward | 17 | 8.4% | |
| 11-Hemodialysis | 08 | 3.9% | |
| 12-Anestesiology | 01 | 0.4% | |
| 13-Other | 29 | 14.4% | |
| Time of work in the institution | 1- -Less than 01 year | 26 | 13.0% |
| 2-From 1 to 05 years | 59 | 29.5% | |
| 3-From 06 to 10 years | 26 | 13.0% | |
| 4 From 11 to 15 years | 33 | 16.5% | |
| 5-From 16 to 20 years | 28 | 14.0% | |
| 6-21 year or more | 28 | 14.0% |
Table III Distribution of variables: Duration of the job in the current area and week hours of the research subjects, Rio de Janeiro (RJ), 2015.
| Variable | Absolute figures | % | |
|---|---|---|---|
| Duration of the job in the current area or Hospital Unit | 1-Less than 01 year | 25 | 12.44% |
| 2-From 01 to 05 years | 87 | 43.28% | |
| 3-From 06 to 10 years | 42 | 20.90% | |
| 4-From 11 to 15 years | 18 | 8.96% | |
| 5-From 16 to 20 years | 19 | 9.45% | |
| 6-21 years or more | 10 | 4.98% | |
| Week hours in the job at the hospital | 1-Less than 20 hours/week | 06 | 2.97% |
| 2-20 hours to 39 hours/week | 148 | 73.27% | |
| 3-40 hours to 59 hours/week | 40 | 19.80% | |
| 4-60 hours to 79 hours/week | 06 | 2.97% | |
| 5-80 hours to 99 hours/week | 02 | 0.99% |
Source: Research Data.
Figure 2 shows that the data obtained from the Dimension support of the hospital management to the patient safety indicate there is a sensation that the directors do not favor a working environment, which is consistent with these issues. Also, the caretakers do not acknowledge actions taken by the Board that prioritize the patient safety, it is clear the lack of interest of the managers.

Figure 2 Distribution of frequencies in the Dimension Support from Hospital Management for the patient safety. Rio de Janeiro, 2015.
Figure 3 show data of the Dimension team work in the units. Apparently, there is not a good transit among the units, which may be conclusive of managerial or command flaws.
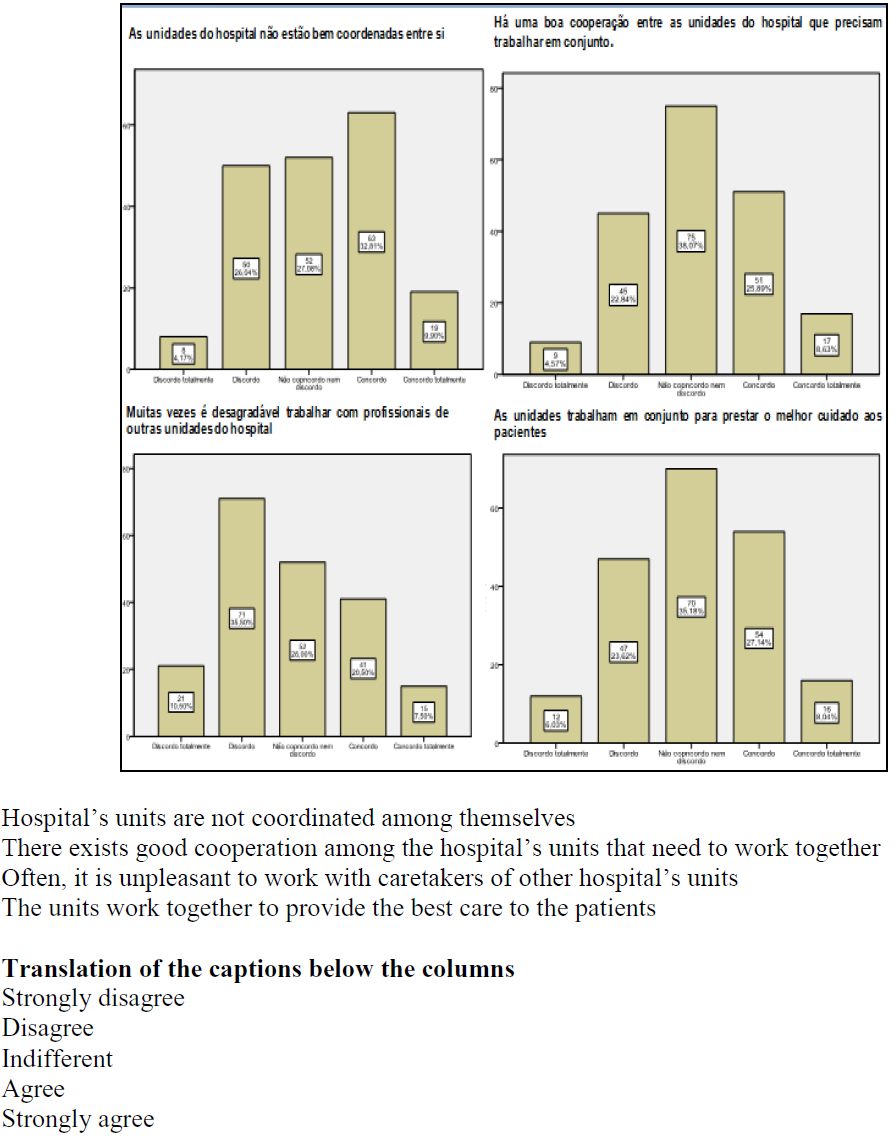
Figure 4 shows data from the Dimension handoffs and transitions within the units. The data point out that the caring process is tainted when patients are transitioned from one unit to another, which is consistent with the response of lack of coordination across units.
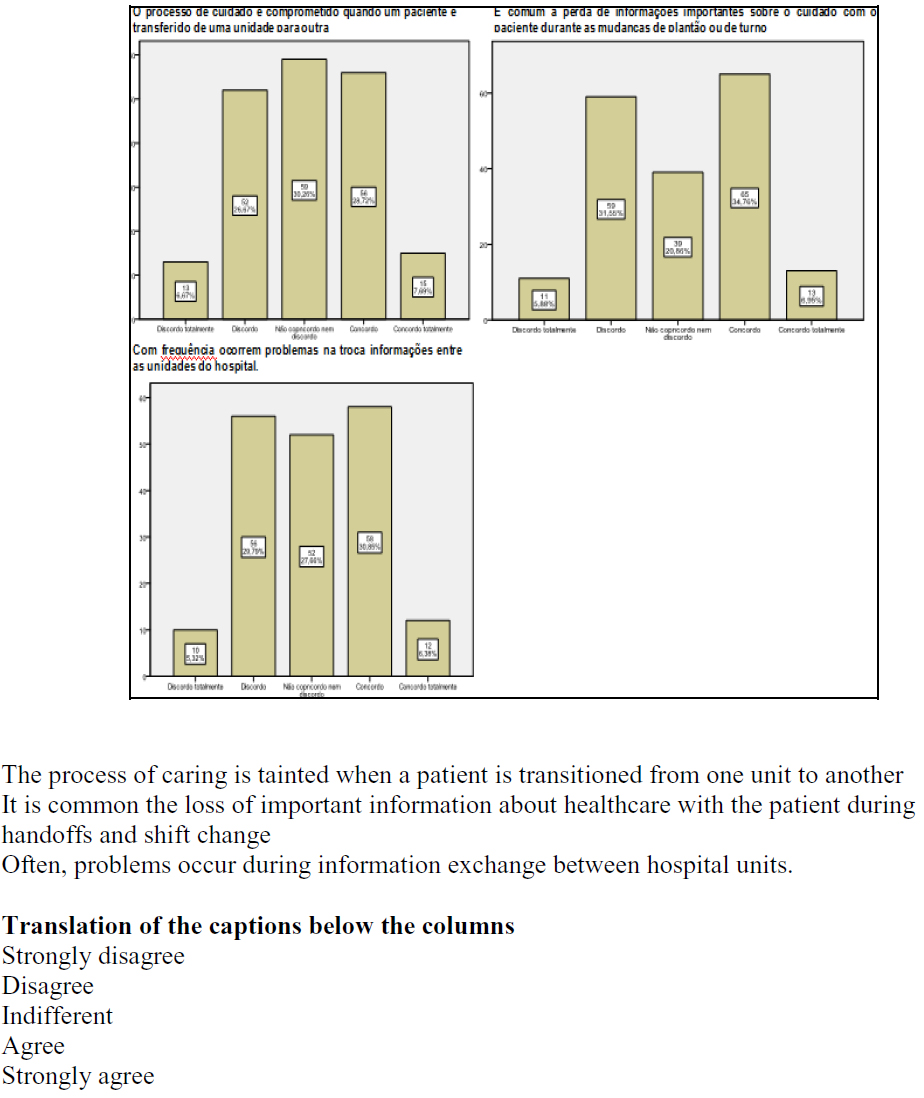
Figure 4 Distribution of frequencies in the Dimension Handoffs/shift change and transition within the units. Rio de Janeiro, 2015.
Table IV presents a comparison of the results of the evaluations with the respective percentage. Of the ten questions investigated, 4 had positive evaluations, even though they are not considered strong areas for the patient safety because the scores are < 50%. Negative evaluations were granted to 4 questions and 2 were neutral.
Table IV Distribution of the Evaluations - Level of Hospital Organization - Rio de Janeiro (RJ), 2015.
| Dimensions | Questões | Evaluation | % |
|---|---|---|---|
| Hospital management support for the patient safety | 1- The hospital Board favors a working environment that promotes the patient safety. | Negative | 34.68% |
| 2 - Actions from the hospital Board demonstrate that the patient safety is a major priority | Negative | 41.83% | |
| 3 - The hospital Board appears to be interested only in the patient safety when an adverse event occurs | Negative | 37.19% | |
| Team work among the teams | 1 -The hospital units are not well coordinated among them | Negative | 42.71% |
| 2 -There is a good cooperation between the units of the hospital that need to work together | Neutral | 34.52% | |
| 3 -Most of the times it is unpleasant to work with professionals of other hospital units | Positive | 46% | |
| 4 -The hospital units work well together to provide the best care to the patients | Neutral | 35.18% | |
| Shift change and transitions | 1 -The caring process shows commitment when a patient is transferred from one unit to other | Positive | 36.61% |
| 2 -It is common the loss of essential information about the care to the patient during shift change | Positive | 40.71% | |
| 3 -Problems often occur when the hospital units exchange information | Positive | 37.23% |
Discussion
The caretakers pointed out the lack of support and actions from managers towards patient safety that negatively interfere in the implementation of safety measures, changes or revisions of flows and processes, incorporation of new technologies, purchasing of new equipment or materials required for the implementation of the Patient Safety National Program according to Directive number 529, dated April 3, 2013.
Batalha (4, in a study developed with nurse caretakers in a university hospital in the state of São Paulo, encountered similar data with 53.6% of negative responses; he mentions a "critical node" in this issue, since the hospital administration could motivate and encourage a healthy working environment to favor patient safety.
These results are endorsed as well by the Massoco 13 study who found 56.8% of negative responses, indicating that in the institution researched, caretakers do not acknowledge effective actions that show that patient safety is a priority.
To create a safety culture it is mandatory that this goal becomes the "steering axle" of the institution. Also, its managers and leaders need to be involved in the daily chores of the institution to create an effective communication channel with the caretakers in charge of the direct care to know the problems and daily challenges 14. With this, trust relations are created, and errors and necessities are clearly exposed which facilitates the solutions and interventions in the work process and permanent training, "empowering" the caretakers to provide a safe care 14.
The research revealed as well that there is no satisfactory coordination across the units and that the staff do not work together to provide better care.
Intervention measures are necessary as well to promote the development of the tasks among the staff from different units for improved coordination, cooperation and communication of services and units and their staff.
Carrera 15, in a study developed in a Federal Oncology Hospital in the City of Rio de Janeiro, encountered similar results which led him to state that in this institution there is no team work organizational culture across the units, though the institution is accredited.
Problems of information exchange across the units occur as well during handoffs, transitions and shift change, which taints the caring process with loss of information that are essential for a safe patient care.
These data suggest the lack of an open and effective communication among professionals, teams, managers and between the units. Urgent interventions are mandatory across every level to ensure a safe and continuous care to the patients. Continuous and Permanent Education is an essential intervention to coach and prepare every caretaker for shift turn when an accurate and appropriate information about the patient is mandatory.
Conclusions
The study showed that the professionals do not recognize actions that favor or prioritize patients' safety issues within the organization and by its managers. Discussions across every tier with their leaders and managers further to other interventions must be deepened to create the setting and environment in favor of Patient Safety in the study subject hospital. The National Program of Safety Patient launched by the Brazilian Ministry of Health through Directive 529, dated April 1, 2013 has as overall objective to contribute to the qualification of the healthcare in every health facility in the entire national territory (16, in addition to compelling every healthcare institution, to review their processes and strategies to mitigate healthcare-related errors, damages and adverse events. Goals that can only be achieved with the involvement of the entire hospital organization from the front line professionals up to the board
Referencias
1. Drucker PF. O melhor de Peter Drucker. A administração. São Paulo:Nobel, 2002. [ Links ]
2. Massarollo MCKB, Fernandes M.F. P. Ética e Gerenciamento em Enfermagem. In: Kurcgant, P.(Coord) Gerenciamento em enfermagem. Editora: Guanabara Koogan, Rio de Janeiro, 2005. [ Links ]
3. Kurcgant P, Massarollo MCKB. Cultura e Poder nas Organizações de Saúde. In: Kurcgant, P.(Coord) Gerenciamento em enfermagem. Editora: Guanabara Koogan, Rio de Janeiro, 2005. [ Links ]
4. Batalha EMSS. A Cultura de Segurança do Paciente na Percepção de Profissionais de Enfermagem de um Hospital de Ensino. 2012.149 p. Dissertação (Mestrado em Ciências) - Escola de Enfermagem da Universidade de São Paulo. São Paulo, 2012. [ Links ]
5. Agencia Nacional De Vigilância Sanitária-Assistência Segura: Uma Reflexão Teórica Aplicada à Prática. Brasília - DF,2013. [ Links ]
6. Wachter RM. Compreendendo a Segurança do Paciente. Tradução de Laura Berquó - Porto Alegre: Artmed, 2010. [ Links ]
7. Ministério Da Saúde. Cria o Programa Nacional de Segurança do Paciente para monitoramento e prevenção de danos na assistência a saúde. Disponível em: http://portalsaude.saude.gov.br/portalsaude/.../PPT_COLETIVA_SEGURANCA...Acesso em: 02/07/2013. [ Links ]
8. Mendes W. Segurança do Paciente. Disponível em: http://www.epi2008.com.br/apresentações/PAINEIS. Acesso em: 23/06/2013. [ Links ]
9. Marques PM. Proqualis. Taxomia-Classificação Internacional para Segurança do Paciente. Disponível em: http://pesquisa.proqualis.net/resources/000000656. Acesso: 03/07/2013. [ Links ]
10. Oliveira MA et al. Gestão de Risco. In: Viana, DL; Leão, ER; Figueredo, NMA (Org). Especialidades em Enfermagem: atuação, intervenção, e cuidados de enfermagem. São Paulo: Yendis, 2010. [ Links ]
11. Gomes AQF. Iniciativas para a Segurança do Paciente difundidas na Internet por Organizações Internacionais: um estudo exploratório, 2008 2p. Dissertação (Mestrado em Ciências na área de Saúde Pública) Escola Nacional de Saúde Pública. Fiocruz, 2008. [ Links ]
12. Reis TC. A cultura de segurança do paciente: validação de um instrumento de mensuração para o contexto hospitalar brasileiro. 2013. Tese (Doutorado em Ciências na área de Saúde Pública) Escola Nacional de Saúde Pública. Fiocruz, 2013. [ Links ]
13. Massoco EPC. Percepções da equipe de enfermagem de um hospital de ensino acerca da segurança do paciente [dissertação]. São Paulo (SP): Universidade de São Paulo, Programa de Pós-Graduação em Gerenciamento em Enfermagem; 2012. [ Links ]
14. Paese F, Sasso GTMD.; Cultura da Segurança do Paciente na Atenção Primária à Saúde. Texto e Contexto Enferm, Florianópolis. 2013;22(2):302-10. [ Links ]
15. Carrera SA. Cultura de Segurança do paciente: A percepção do enfermeiro em um hospital oncológico [dissertação] Mestrado em Enfermagem. Rio de Janeiro (RJ): Universidade Federal do Estado do Rio de Janeiro, UNIRIO, 2012. 141fl [ Links ]
16. Diário Oficial da União de 24/04/2013; Portaria nº 529, de 1 de abril de 2013. [ Links ]
Received: September 29, 2015; Accepted: October 05, 2015
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
