










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.16 no.48 Murcia oct. 2017 Epub 14-Dic-2020
https://dx.doi.org/10.6018/eglobal.16.4.262831
Revisiones
Instruments and Assessment Tools to Evaluate Knowledge on Tuberculosis
1Nurse, Faculty of Nursing, Universidad Nacional de Colombia. Bogotá. Colombia.
2PhD in Nursing. Full Professor, Faculty of Nursing, Universidad Nacional de Colombia. Bogotá. Colombia.
Introduction
Insufficient knowledge about tuberculosis (TB) attempts against programs to control this disease and lead to mistaken behaviors in caring for the patient’s health, the care provided by TB control programs, and caring for the patient’s family and the community.
Objective
The work sought to describe the scientific production of instruments and assessment tools on knowledge about TB, available for the health staff, patients, the community, and families.
Methodology
An integrative search was carried out in four databases (Embase, Science Direct, Redalyc, and Biblioteca Virtual de la Salud-BVS), with the following inclusion criteria: full-text articles (in English, Spanish, or Portuguese), published between August 2010 and August 2015.
Results
The study included 42 articles, systematized in Excel for each of the study populations. Systematization permitted evidencing greater scientific production in Latin America and Africa and research aimed at assessing knowledge by the health staff and the community. Of the 42 articles selected, only five used instruments with some type of validation and were subjected to reliability tests through Cronbach’s alpha coefficient.
Conclusions
The results permitted identifying the need to conduct research that includes the design and validation of instruments, as well as the evaluation of knowledge by patients and the families.
Keywords Tuberculosis; Knowledge; Instruments for the Management of the Scientific Activity; Review (DeCS)
INTRODUCTION
Tuberculosis (TB) is an infectious disease of global distribution; its easy transmission, favored by the precarious living conditions of individuals exposed to it, make TB one of the principal diseases of interest in public health, placing it as the second cause of death globally due to infectious diseases 1. In addition, the goal established to reduce to 50% the prevalence and mortality due to TB globally has not been reached 2.
According to the Global Tuberculosis Report 2016, in 2015, 10.4-million people contracted TB and 1.4-million died because of it 1. In Colombia, for 2015, the National System of Public Health Surveillance (SIVIGILA, for the term in Spanish) was notified, during week 52, of 12,918 cases of TB in all forms, which represented a 2.0% increase in notifications with respect to week 52 for 2014 3. For epidemiological week 03 of 2016, 577 cases of TB were reported in all its forms, with pulmonary TB having the highest presence, with 85.6% of the total number of cases 4. Bogotá, for 2015, reported an incidence of 12.6 TB cases per 100,000 inhabitants 3.
Hence, to achieve compliance with the Sustainable Development Objectives (SDO), which stipulate the eradication of TB by 2030 5, it was established that programmatic actions must continually be strengthened to prevent and control TB globally 6 starting with education to enhance knowledge about TB by all the population. Thus, identifying knowledge about TB by health workers, patients, families, and the community is indispensable, given that a high level of knowledge reveals a favorable process in health education that contributes in the global management of the disease, diminishes the disease’s active transmission and favors early and timely diagnosis, as well as early onset of treatment and adherence to such 7)(8.
Conversely, scientific literature evidences that lack of knowledge can determine mistaken and wrong behaviors in health care, leading to stigmatizing and isolating the patient, delaying diagnosis and treatment of TB, and favoring poor adherence to treatment 9, which is why the disease is still transmitted 10. Consequently, it is fundamental for the health staff, patients, the community, and families to have adequate knowledge about TB.
Regarding knowledge by the health staff, literature indicates that they must be suitable, adequate 11, and solid 12) to ensure success of TB prevention, diagnosis, surveillance, and control. Sufficient knowledge by the health staff guarantees adequate training and guidance to individuals with the disease, their families, and communities, which permits ensuring success of the anti-tuberculosis treatment 13.
With respect to knowledge by patients with TB, literature shows that poor knowledge promotes transmission and infection of the disease to their relatives and their community 13 because false beliefs are raised about it and because of their fear of being stigmatized. This causes patients with TB to hide their disease, self-medicate, and generate drug-resistant TB due to their abandoning or suspending treatment 14. Knowledge by families of patients with TB permit placing this disease in the first place in health care and in the most significant microstructure in decision making in relation to the health/disease process of the person with TB, which is why knowledge by the family is indispensable to provide adequate care and acquire prevention measures against the transmission of the disease 15)(16.
Similarly, studies on the community state that it is important to assess its knowledge, given that it is a decisive factor to mitigate TB infection 17)(18. In spite of sufficient scientific evidence on knowledge about TB, Yukselturk & Dinc 19) highlight the importance of validating measurement instruments to evaluate knowledge about TB, given that in literature no reliable instruments are found that can be replicated and used for other studies. Due to the aforementioned, this study sought to describe the scientific production of instruments and assessment tools on knowledge by patients, health staff, families, and the community on TB, during the period from August 2010 to August 2015, to report the most recent scientific literature on the theme.
It is important to highlight that this study will bear in mind some concepts, like: 1) assessment instruments: those with psychometric characteristics that give them support, reliability, and validity 20, which lets them be culturally relevant, within a given historical place and moment 21; 2) assessment tools: those surveys and questionnaires, among others, that permit developing activities like scoring, measuring, correcting, classifying, certifying, and examining the level of appropriation of new knowledge 22.
METHODOLOGY
An integrative review was conducted with the following phases: 1) definition of the objective; 2) definition of inclusion criteria; 3) search for studies in databases and selection of studies according to the inclusion criteria; 4) critical evaluation of the studies; 5) categorization of the studies selected, and 6) data analysis 23.
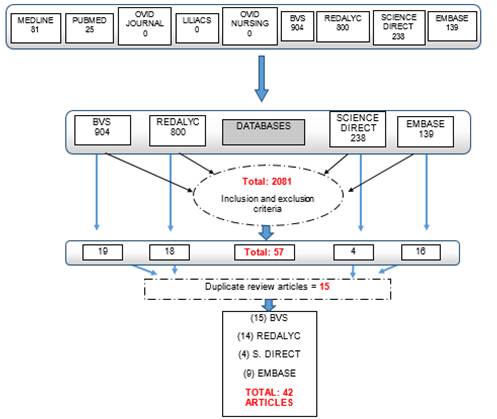
The search was conducted in nine databases; however, four providing the highest number of articles were selected: BVS (Virtual Library on Health), Embase, Science Direct, and Redalyc (Figure 1). In the databases mentioned, the study used the Health Sciences Descriptors (DeCS) and Medical Subject Headings (MeSH) to form the search strategies according to the database: 1) Tuberculosis AND knowledge AND Questionnaires (Embase, Science Direct, and BVS) and 2) Tuberculosis AND knowledge AND Instruments for Management of Scientific Activity (Redalyc).
Article selection was carried out according to the following inclusion criteria: year of publication comprised between August 2010 and August 2015; articles in Spanish, English, and Portuguese; articles from primary research in full text, and studies that included instruments or tools to assess knowledge about TB in any of the four populations object of study (person with TB, family, community, health staff).
Upon identifying and selecting the articles, these were subjected to evaluation, a phase that used the Scottish Intercollegiate Guidelines Network (SIGN) evidence levels of classification in independent manner to determine the methodological quality of the articles 24.
After the critical evaluation of the articles, a second reading was performed to categorize the dimensions assessed on knowledge in the instruments or tools found in relatives, health staff, patients, or community. For this purpose, a database was constructed in Microsoft Excel for each study population, which permitted the respective description of the scientific production of instruments or assessment tools of knowledge about TB by each of them.
RESULTS
The search in nine databases produced 57 articles, which were reduced to 42 after excluding 15 articles that did not comply with the inclusion criteria: one had no exact description of an instrument or tool to assess knowledge, another was not within the period stipulated, and 13 were in two databases at the same time. Figure 1 presents the results of the search in the number of articles found (Figure 1).
The Integrative Review included 42 articles, which are listed in Table 4, Table 5, Table 6, and Table 7, grouping the principal data of the studies: name of the article, year, authors, type of study, country, instrument or tool used to assess knowledge, variables of the instrument or too, and type of validity and reliability in each of the articles.
Table 4 Scientific production of instruments and assessment tools on knowledge of TB by patients

Source: Elaborated by the authors
Table 5 Scientific production of instruments and assessment tools on knowledge of TB by the health staff
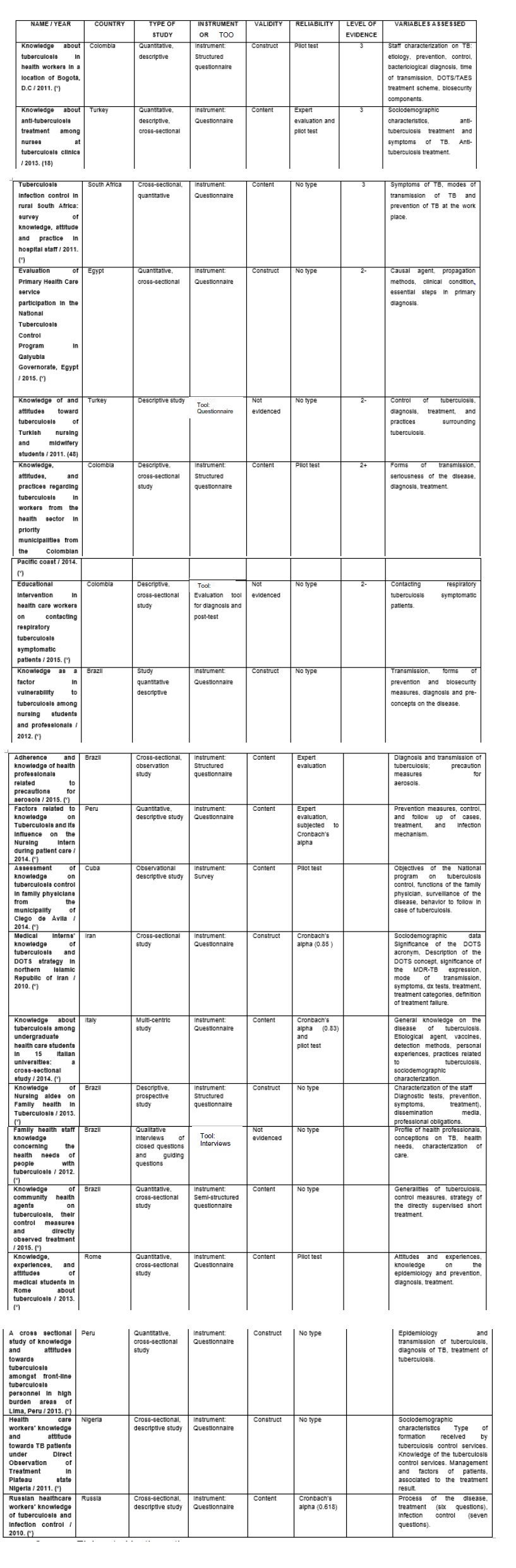
Source: Elaborated by the authors
Table 6 Scientific production of instruments and assessment tools on knowledge of TB in the community
| NAME | COUNTRY | TYPE OF STUDY | INSTRUMENT OR TOOL | VALIDITY | RELIABILITY | LEVEL OF EVIDENCE | VARIABLES ASSESSED |
|---|---|---|---|---|---|---|---|
| Knowledge and perception about tuberculosis in the municipality of Habana Vieja / 2012. (52) | Cuba | Quantitative, cross-sectional study | Instrument: Structured survey | Content | No type | 3 | Etiology, symptoms and modes of transmission. |
| Assessment of Knowledge towards Tuberculosis among general population in North East Libya / 2012. ( ) | Libya | Quantitative, cross-sectional study | Instrument: Pre-validated questionnaire | Content | Expert evaluation | 3 | Sociodemographic characterization, causes, symptoms, transmission, factors that contribute to transmission, diagnosis, treatment and prevention of TB. |
| A public-private partnership model to reduce tuberculosis burden in Akwa Ibom State - Nigeria / 2015. ( ) | Nigeria | Descriptive study | Instrument: Questionnaire | Not evidenced | Pilot test | 2- | Sociodemographic characterization, transmission, diagnosis and treatment, prevention measures. |
| Tuberculosis-related knowledge is associated with patient outcomes in shantytown residents; results from a cohort study, Peru / 2015. (51) | Peru | Observational descriptive study | Instrument: Questionnaire | Construct | No type | 2- | Sociodemographic characterization, generality of the disease, transmission and treatment. |
| Evaluation of knowledge of cattle breeders on bovine tuberculosis and implications for its control / 2014. ( ) | Portugal | Descriptive study | Instrument: Questionnaire | Construct | No type | 3 | Transmission, clinical manifestations, control measures. |
| Knowledge about tuberculosis in community health agents in Tacna, Peru / 2012. ( ) | Peru | Descriptive, non-probabilistic study | Instrument: Survey | Construct | No type | 3 | Definition of the disease, diagnosis, treatment, prevention measures. |
| Knowledge, attitudes, and practices on tuberculosis Zenú indigenous people and inhabitants of a Colombian rural zone / 2013. ( ) | Colombia | Cross-sectional, descriptive study | Instrument: Survey | Content | Expert evaluation via Cronbach’s alpha. | 2+ | Generalities of the infection, organs affected transmission, factors and risk groups, signs and symptoms. |
| Community knowledge, attitude, and practices towards tuberculosis in Shinile town, Somali regional state, eastern Ethiopia: a cross-sectional study / 2014. ( ) | Ethiopia | Cross-sectional study | Instrument: Standardized questionnaire | Construct | Pilot test | 3 | Sociodemographic characterization, signs, symptoms, mode of transmission, prevention methods. |
| Knowledge and attitude of key community members towards tuberculosis: mixed method study from BRAC TB control areas in Bangladesh / 2015. ( ) | Bangladesh | Mixed method. Qualitative and quantitative | Instrument: Questionnaire of the quantitative survey | Not evidenced | Pilot test | 3 | Signs and symptoms, transmission, prevention and treatment of tuberculosis. |
| Community’s knowledge, attitudes and practices about tuberculosis in Itang Special District, Gambella Region, South Western Ethiopia / 2013.(50) | Ethiopia | Cross-sectional study | Instrument: Structured questionnaires | Construct | Expert evaluation | 3 | Cause of tuberculosis, symptoms, mode of transmission of tuberculosis, risk factors, identification of individuals with high risk of TB. |
| Knowledge, Attitudes, and Practice of Tuberculosis among Maasai in Simanjiro District, Tanzania / 2010. ( ) | Tanzania | Mixed exploratory-descriptive study | Tool: Structured test-type questionnaire | Not evidenced | Pilot test | 3 | What is tuberculosis, signs and symptoms, causes, treatment, prevention, and transmission |
Source: Elaborated by the authors
Table 7 Scientific production of instruments and assessment tools on knowledge of TB by the family
| Author/Year | Country | Type of study | Instrument or Tool | Validity | Reliability | Level of Evidence (sign) | Variables Assessed |
|---|---|---|---|---|---|---|---|
| Moreira et al.,(2012) | Brazil | Descriptive, Cross-sectional study | Tool: Questionnaire | Not Evidenced | Pilot test | 2+ | Transmissibility period after the onset of treatment, appropriate treatment period (duration), the concern of contracting TB |
Source: Elaborated by the authors
The following show the most significant percentages in the characterization of the scientific production found:
Table 1 evidences that the highest scientific production was found in the health staff on the assessment of knowledge about TB through instruments or assessment tools.
Table 1 Percentage of production by categories
| Category | Percentage |
|---|---|
| Health staff | 52.3% |
| Community | 26.1% |
| Patients | 19.4% |
| Family | 2.3% |
Source: Elaborated by the authors
Table 2 identifies Latin America as the continent with the most scientific production on knowledge about TB.
Table 2 Production by continents
| Country | Percentage |
|---|---|
| Latin America | 47.6% |
| Africa | 26.10% |
| Asia | 14.20% |
| Europe | 9.5% |
| Oceania | 2.3% |
Source: Elaborated by the authors
Table 3 shows that of the Latin American countries, Brazil is the country with the most scientific production on assessment of knowledge about TB.
Table 3 Production in Latin America
| Country | Percentage |
|---|---|
| Brazil | 38.10% |
| Colombia | 23.80% |
| Peru | 23.80% |
| Cuba | 10% |
Source: Elaborated by the authors
With respect to the type of study used in the research reviewed, 90.5% is quantitative-type research (92.1% are cross-sectional descriptive studies, 5.3% are prospective studies, and 2.6% are quantitative studies of cases and controls), 7.1% are mixed studies, given their qualitative and quantitative characteristics, and only 2.3% are qualitative studies.
With regard to the strategies to assess the reliability of the instruments used to measure the level of knowledge, these are divided into three parameters: articles that base their reliability on a pilot test (26.2%), articles using expert evaluation to test their reliability (9.5%), and research that apply Cronbach’s alpha coefficient (7.1%). Some of the scientific research used more than one parameter to provide reliability to the instrument or method; 2.4% used the pilot test and expert evaluation, 2.4% were based on the three parameters (expert evaluation, pilot test, and Cronbach’s alpha coefficient), and 4.8% did so through expert evaluation and Cronbach’s alpha coefficient. Finally, it is worth highlighting that 47.6% of the studies do not specify the development of the methodological procedures of reliability used in the instruments or assessment tools.
Another important aspect was the type of validity assigned to the instruments and assessment tools. For this purpose, two forms of validation were used 20: the first is the construct validation, seen in 33.3% of the articles; the second is the content validity, which corresponds to 40.5% of the articles. In 28.2%, no validity of any type is noted.
The dimensions of the instruments or tools in common in the scientific production selected are sociodemographic characteristics of the study population (age of participants, gender, occupation, etc.), causes, diagnosis, signs and symptoms, prevention, treatment, and transmission of the disease.
The following present information compiled with respect to the instruments and tools used to assess knowledge on tuberculosis, discriminated by the different categories of patients, family, health staff, and communities.
Instruments and assessment tools on knowledge of TB by patients
Quantitative-type studies are prevalent in the patient category with an evidence level of 3, according to the SIGN classification 24. Most studies had no strategy to measure reliability and content validity is the most-often used in all the articles found. Finally, among the dimensions used in the instruments or tools to assess knowledge, there is the mode of TB transmission, and most consider that knowledge about TB by patients is low (Table 4).
Instruments and assessment tools on knowledge of TB in the health staff
The health staff had the highest scientific production, with mostly quantitative-type studies and 2+ level of evidence prevailing, according to the SIGN classification 24. To evaluate reliability, it was found that the majority of the studies (18 of 22) do not use any strategy to measure such; however, it must be highlighted that four of the instruments used Cronbach’s alpha coefficient and content validity content, which is the type of validity used in most studies from this category. With respect to the dimensions used in the instruments or tools to assess knowledge, we find the treatment. It was noted that the level of knowledge by the health staff about TB was low (Table 5).
Instruments and assessment tools on knowledge of TB by the community
For this category, the results revealed that all the studies are quantitative type with 2+ level of evidence prevailing, according to the SIGN classification 24. Only one article, conducted in Colombia in Zenú communities, had an instrument with content validity and Cronbach’s alpha coefficient as reliability method. Even so, construct validation prevailed in most of the articles using the pilot test and expert evaluation as reliability method. Mode of transmission was found as the most-assessed dimension, and it is noted that the level of knowledge about TB by this population is low (Table 6).
Instruments and assessment tools on knowledge of TB by the family
In this case, we found the lowest scientific production, given that only one qualitative-type article was found, which has no validated evaluation instrument, but does have an evaluation tool. The dimensions assessed in this case are the mode of transmission, treatment, and control of the disease, and knowledge was considered high in this study for this population (Table 7).
DISCUSSION AND APPLICATIONS IN HEALTH
This study evidenced the existence of a large amount of scientific production in Latin America and Africa, which agrees with the presence of the high prevalence and incidence of TB in these parts of the world. In light of the aforementioned, the WHO 25) mentions the need to conduct studies regarding knowledge about TB to achieve control of the disease through educational actions.
The vast majority of the studies found are from the health staff category, representing 52.3% of the total; nevertheless, it became important to detail the results reported by research, given that although this population mostly evaluates knowledge, these prove to be deficient to identify the pathology. This same result was evidenced by Laurenti et al.,26 by mentioning that low levels of knowledge by the health staff exist due to the poor academic preparation on TB (27. This permits reflecting upon the importance of continuing to enhance knowledge in the health staff 28)(29 with constant training processes in health care institutions and undergraduate academic formation about TB 30.
Assessment of knowledge in the community occupies an intermediate level in scientific production; however, scientific evidence states that communities (especially indigenous and rural communities) are not populations of interest in research on TB, although they are highly vulnerable groups for continuous and early transmission of the disease 31.
Although most studies are related to the health staff, it is worth emphasizing another aspect noted, given that it was found that not many research works encompass knowledge about TB assessed in patients and families, representing 19.4% and 2.3%, respectively, of the total number of articles. Due to the scarce research knowledge by patients and families, it is possible to overlook the importance of correct knowledge they have about TB, to generate adherence to treatment and control transmission of the disease in the family and the community 32)(33)). Added to the poor scientific production to assess knowledge about TB in patients, the articles revealed a low level of knowledge in this population, which generates a factor that negatively affects health interventions aimed at controlling TB34. The aforementioned poses a challenge for the different health disciplines to carry out new research that permit creating health care interventions that raise awareness in patients about their disease 28, and implementing educational processes as important aspects to prevent and control the disease 35.
Measuring knowledge about TB through instruments or assessment tools sets big challenges, given that not many of the studies found clearly reveal the validation processes of the instruments or the psychometric parameters assessed, and very few evidence some type of validation. Much lower still is the number of instruments (5 instruments) with Cronbach’s alpha coefficient as reliability test, as a test that provides the instrument with greater reliability upon evaluating the correlations existing between each of the items 36) and, hence, Cronbach’s alpha coefficient must be a tool that offers precision to the instruments 37. Thereby, lack of validation and of psychometric parameters are aspects that question the reliability of the results, given that it is indispensable that these be validated instruments to truly test the hypotheses proposed 38, measure what needs to be measured with trustworthy results 39 and without probability of bias 40)(41.
The lack of clarity of the validation process of the instruments is because the studies found assessed knowledge about TB, but none introduced the design of a completely validated and reliable instrument that complies with all the psychometric parameters, as stated by Yukselturk et al.,19 who indicated that no validated instruments exist that permit replicability of the instrument to other research.
With respect to the level of evidence of the scientific production found, it was noted that most of the studies belong to a level of evidence of 2+ and 3, according to the SIGN scale 24. This showed that, although these are investigations that contribute to the development of knowledge about TB, studies with greater reach are needed that permit unveiling the creation and design of a validated instrument to assess knowledge about TB that provides reliable results verifiable with other studies42. The design of instruments aimed at the four study populations creates a challenge for future researchers, especially instruments for patients and families, given that they are the two populations with the least scientific production found and with no instrument validated.
Finally, the instruments must be validated and reliable for the results obtained, after the assessment of knowledge from the population, to guide in decision making in health and, thus, permit enhancing strategies and actions to improve the health conditions of patients and of the global population, managing to end TB, to be in agreement with the new SDO 5.
FINAL CONCLUSIONS
Tuberculosis is an easily transmitted disease associated to the precarious living conditions of people exposed to it and to poor knowledge about it. The comprehensive review evidenced the wealth of scientific production on TB, with knowledge being one of the most important themes to investigate. However, a rigorous search of the instruments and assessment tools on knowledge patients, health staff, the community, and families of patients have about TB indicated scarce scientific production, given that most studies on knowledge about TB have no type of instrument used or developed, and those that have it do not clearly evidence a validation process with psychometric parameters. The most frequently evaluated dimensions in the instruments were cause, prevention, mode of transmission, signs and symptoms, and treatment, which are themes that must be further enhanced in educational interventions.
Scientific production on instruments and assessment tools on knowledge of TB is mostly found among the health staff; thereby, identifying the need to carry out subsequent research that design an evaluation instrument on knowledge about TB to apply with patients and families. Lastly, research must be continually enhanced to assess knowledge about TB that permits making decisions in health to prevent, control, and eradicate TB.
REFERENCIAS
1. World Health Organization. Global tuberculosis Report 2016. Suiza. Disponible en: http://reliefweb.int/sites/reliefweb.int/files/resources/gtbr2016_main_text.pdf [ Links ]
2. Organización Panamericana de la Salud (OPS) [Internet]. Situación del control de la TB en las Américas. Programa regional de control de la TB. Washington D.C. [Consultado el 25 de agosto del 2015]. Disponible en: http://www.paho.org/hq/index.php?option=com_docman&task=doc_view&gid=24581&Itemid [ Links ]
3. Instituto Nacional de Salud [Internet]. Boletín Epidemiológico Semanal (Semana 52 del 2015). Colombia. 2015. [Consultado el 12 de enero del 2016]. Disponible en: http://www.ins.gov.co/boletin-epidemiologico/Boletn%20Epidemiolgico/2015%20Boletin%20epidemiologico%20Semana%2052.pdf [ Links ]
4. Instituto Nacional de Salud [Internet]. Boletín Epidemiológico Semanal (Semana 03 del 2016). Colombia. 2016. [Consultado el 01 de febrero del 2016]. Disponible en: http://www.ins.gov.co/boletin-epidemiologico/Boletn%20Epidemiolgico/2016%20Boletin%20epidemiologico%20semana%203.pdf [ Links ]
5. Naciones Unidas [Internet]. Objetivos del Desarrollo Sostenible, Meta 3. 2015. [Consultado el 20 de noviembre del 2015]. Disponible en: http://www.un.org/sustainabledevelopment/es/health/ [ Links ]
6. Naciones Unidas [Internet]. Objetivos de desarrollo del Milenio, Informe de 2015. New York. Editora. Catharine Way. 2015. [Consultado el 24 de agosto del 2015]. Disponible en: http://www.un.org/es/millenniumgoals/pdf/2015/mdg-report-2015_spanish.pdf [ Links ]
7. Ladino LE. Creencias y prácticas sobre la tuberculosis en un grupo de pacientes y sus familiares de la ciudad de Bogotá, D. C. Una aproximación cualitativa. Tesis de maestría. Universidad Nacional de Colombia. [Internet]. Colombia. 2011. [Consultado el 25 de agosto del 2015]. Disponible en: http://www.bdigital.unal.edu.co/4325/1/598589.2011.pdf [ Links ]
8. Antón R, Mezones E. Bajo nivel de conocimientos y actitud de rechazo hacia el tratamiento de tuberculosis. Rv Peru Med Exp Salud Pública. 2009; 26 (4): 582-590. [ Links ]
9. Zarzuelo R. Conocimientos sobre Tuberculosis en Pacientes que concurren al Hospital SMCO Dr. Reynaldo Barrionuevo de la ciudad de Capitán Bermúdez. [Internet]. Argentina. 2012. [Consultado el 25 de agosto del 2015]. Disponible en: http://imgbiblio.vaneduc.edu.ar/fulltext/files/TC111941.pdf [ Links ]
10. Ladino LE. Creencias y prácticas sobre la tuberculosis en un grupo de pacientes y sus familiares de la ciudad de Bogotá, D. C. Una aproximación cualitativa. Tesis de maestría. Universidad Nacional de Colombia. [Internet]. Colombia. 2011. [Consultado el 25 de agosto del 2015]. Disponible en: http://www.bdigital.unal.edu.co/4325/1/598589.2011.pdf [ Links ]
11. Abreu G, González JA, Muñoz R, Solar LA. La preparación del estudiante de Medicina para la eliminación de la tuberculosis. Educación Médica Superior. La Habana, Cuba. 2013; 27(1):38-45. [ Links ]
12. Ministerio de Salud y la Protección Social [Internet]. Lineamientos 2014, para la prevención, vigilancia y control en salud pública Instituto nacional de salud. Colombia. 2014. [ Links ]
13. Kerri V, Penelope J, Markleen T, Saen F, Nguyen L, Paul K, et al. Tuberculosis patients' knowledge and beliefs about tuberculosis: a mixed methods study from the Pacific Island nation of Vanuatu. BMC Public Health. 2014; 1 (14): 467-471. [ Links ]
14. Ahmed E, Ibrahim A, Mulualem A, Adinew D, Zelalem Y, Kassu D. Assessment of Patients' Knowledge, Attitude, and Practice Regarding Pulmonary Tuberculosis in Eastern Amhara Regional State, Ethiopia: Cross-Sectional Study. Am. J. Trop. Med. Hyg. 2013; 88 (4): 785-788. [ Links ]
15. Moreira I, Almeida J, Carvalho I, Scatena TC, Firmino ME, Porto PF, Alexandre R. Conocimiento y percepción de las familias sobre Tuberculosis en pacientes bajo tratamiento directamente observado en un servicio de salud de ribeirão preto-sp, Brasil. Text Context Nursing, Florianópolis. 2012; 21(3): 642-649. [ Links ]
16. Monteiro S, Mendoza RA, Pereira T, do Amaral V, Cézar MR. Conhecimento dos clientes com tuberculose pulmonar e seus familiares sobre adesão ao tratamento e fatores associados, no município do Rio Grande (RS). Ciênc. Saúde Coletiva. 2011; 16 (1): 1427-1435. DOI: 10.1590/S1413-81232011000700078. [ Links ]
17. Delgado V, Cadena LP, Tarazona G, Lozano CE, Rueda EA. Nivel de los conocimientos sobre tuberculosis en dos comunidades del Área Metropolitana de Bucaramanga, Santander. Revista CES Salud Pública. 2015; 6 (1): 40-51. [ Links ]
18. Cramm JM, Finkenflugel HJ, Moller V, Nieboer AP. TB treatment initiation and adherence in a South African community influenced more by perceptions by knowledge of tuberculosis. BMC Public Health. 2010; 10: 72. DOI: 10.1186/1471-2458-10-72. PMID: 20163702. PMCID: PMC2828408. [ Links ]
19. Yukselturk N, Dinc L. Knowledge about anti-tuberculosis treatment among nurses at tuberculosis clinics. International Journal of Nursing Practice. 2013; 19 (1): 47-53. [ Links ]
20. Carvajal A, Centeno C, Watson R, Martínez M, Rubiales A. Cómo validar un instrumento de medida de la salud. Anales Sistemas Sanitarios Navarra. 2011; 34 (1). [ Links ]
21. Alonso J, Prieto L, Antó J. Un instrumento para la medida de los resultados clínicos. Instituto Municipal de Investigación Médica (IMIM). 1995; 104 (20): 1-8. [ Links ]
22. Méndez JM. Evaluar para conocer, examinar para excluir. Morata. 2000. [ Links ]
23. Tavares M, Días M, De Carvalho R. Revisão integrativa: o que é e como fazer. Einstein. 2010; 8 (1): 102-106 [ Links ]
24. Mazo M, Viana C. Calidad de la evidencia y grado de recomendación. Guías Clínicas. 2007; 7 (1): 1-6. [ Links ]
25. Organización Mundial de la Salud [Internet]. Tuberculosis. 2014. [Consultado el 24 de agosto del 2015]. Disponible en: http://www.who.int/mediacentre/factsheets/fs104/es/ [ Links ]
26. Laurenti P, Federico B, Raponi M, Furia G, Ricciardi W, Damiani G. Knowledge, experiences, and attitudes of medical students in Rome about tuberculosis. Med Sci Monit. 2013; (19): 865-874. [ Links ]
27. Galdino JH, Oliveira LK, Lopes M, Vieira L, Ferreira A. Adesão e conhecimento de profissionais da saúde em relação às precauções para Aerossóis. Revista da Rede de Enfermagem do Nordeste. 2015; 16 (4): 514-522. [ Links ]
28. Mangveep L, Suleiman I, Nguku P, Endie N, Obiemen M, Petrobas P. Health care workers' knowledge and attitude towards TB patients under Direct Observation of Treatment in Plateau state Nigeria, 2011. Pan African Medical Journal. 2014; 18 (1):1-4. [ Links ]
29. Souto GS, Guimaraes M, Moreira JL, Crepalde K, Braga M, Da Silva Q, Silveira M. El conocimiento de los trabajadores sanitarios de la comunidad sobre Tuberculosis, las medidas de control y tratamiento bajo observación directa. Cad. Saúde Pública. 2015; 31 (7):1483-1496. [ Links ]
30. Ortega GL, Rodríguez PA, Jiménez EC, Muñoz AI. Conocimientos sobre tuberculosis en estudiantes de enfermería de una universidad colombiana. Rev. Univ. Ind. Santander. Salud. 2015; 43 (3): 261-270. [ Links ]
31. Cardona JA, Hernández AM. Conocimientos, actitudes y prácticas sobre tuberculosis en indígenas zenúes y habitantes de una zona rural colombiana. Revista Ciencias de la Salud. 2013; 11 (2): 159-173. [ Links ]
32. Laurente J, Remuzgo F, Gllardo J, Taype L, Huapaya J, Carrillo J. et al. Conocimientos y actitudes acerca de la transmisión y prevención de la tuberculosis en pacientes con tuberculosis multidrogorresistente. Revista Peruana de Epidemiología. 2010; 14 (1): 1-7. [ Links ]
33. Antón R, Mezones E. Bajo nivel de conocimientos y actitudes de rechazo hacia el tratamiento de Tuberculosis. Rev Peru Med Exp Salud Pública. 2009; 26 (4): 558-590. [ Links ]
34. Gonzáles Y, Geldenhuys H, Van D, Buckerfield N, Shea J, Mahomed H, Hanekom W, Hatherill M. Knowledge and acceptability of patient-specific infection control measures for pulmonary tuberculosis. American Journal of Infection Control. 2013; 41 (2013): 717-722. [ Links ]
35. Musayon FY, Loncharich N, Salazar ME, Leal HM, Silva I, Velásquez D. Función d la enfermería en el control de la tuberculosis: una discusión desde la perspectiva de la equidad. Revista Latino Americana de Enfermería. 2010; 18 (1): 130-138. [ Links ]
36. George D, Mallery P. SPSS for Windows step by step: A Simple Guide and Reference. 11.0 Update (4ª ed.). Boston: Allyn & Bacon. 2003. [ Links ]
37. Soler SF, Soler L. Usos del coeficiente alfa de Cronbach en el análisis de instrumentos escritos. Rev. Med. Electrón. 2012; 34 (1): 1-6. [ Links ]
38. Mercado A, Gil PR. Características psicométricas del Cuestionario para la evaluación del síndrome de quemarse por el trabajo en maestros mexicanos. Revista de Educación. 2012; 1 (1): 260-273. [ Links ]
39. Duarte M, De Morais R, Marziale MH. Instrumentos y factores impactantes en el conocimiento de medidas de precaución estándar entre trabajadores de la salud. Enfermería Global. 2016; 15 (1): 272-288. [ Links ]
40. Carvajal R, Varela MT, Hoyos PA, Angulo ES, Duarte C. Conocimientos, actitudes y prácticas frente a la tuberculosis en trabajadores del sector salud en municipios prioritarios de la Costa Pacífica Colombiana. Rev. Cienc. Salud. 2014; 12 (3): 339-352. [ Links ]
41. Gonzales Y, Geldenhuys H, Van As D, Buckerfield N, Shea J, Mahomed H, Hanekon W, Hatherill M. Knowledge and acceptability of patient-specific infection control measures for pulmonary tuberculosis. American Journal of Infection Control. 2013; 41: 717-722. [ Links ]
42. González VP, Madrigal SD, Treviño FE, Aguilar A. Propuesta y validez de un instrumento para el manejo de tecnologías de información en la investigación. Ponencia. 2005. México. [ Links ]
Received: July 06, 2016; Accepted: November 18, 2016
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
