










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkEnfermería Global
versão On-line ISSN 1695-6141
Enferm. glob. vol.17 no.49 Murcia Jan. 2018 Epub 14-Dez-2020
https://dx.doi.org/10.6018/eglobal.17.1.301041
Originales
Sociodemographic, individual and programming characteristics of women with cervical cáncer
1PhD, Nursing Department, Faculty of Medicine of Botucatu, Univ Estadual Paulista/UNESP, Botucatu, São Paulo, Brazil.
2RN, Nursing Department, Faculty of Medicine of Botucatu, Univ Estadual Paulista/UNESP, Botucatu, São Paulo, Brazil.
Introduction
cervical cancer is a serious public health problem throughout the world and often affects women of low socioeconomic level and of reproductive age.
Objective
to identify the set of sociodemographic, individual and programmatic characteristics present in the daily life of women that made them vulnerable to cervical cancer.
Method
descriptive and cross-sectional study addressing the various dimensions of vulnerability that had the participation of 99 women with a confirmed diagnosis of cervical cancer. To characterize the women, a structured questionnaire was used, composed of information directed to the sociodemographic aspects of the individual and related to the organization of the health services.
Results
the predominant age group was between 40 and 57 years. Most started sexual activity between 15 and 18 years old, had up to five sexual partners and had never used a condom. There was prevalence of married, white, Catholic women with primary education, family income between one and two minimum wages and having their own house. Before the diagnosis of cervical cancer, 45.5% performed the preventive examination once a year and after cytopathological collection, it occurred at least once a year. The majority sought the health service after symptoms of the disease.
Conclusion
it is necessary to develop effective interventions for women's health care based on the concept of comprehensiveness of care provided.
Keywords: Uterine Neoplasms; Women's Health; Vulnerability in Health
INTRODUCTION
Cervical cancer is a serious public health problem worldwide, with developing countries accounting for 80.0% of the cases. Adolescents are more exposed to human papillomavirus (HPV) infection, being the highly vulnerable population to develop precursor lesions for cervical neoplasia1)(2.
In Canada, due to accessibility of the preventive exam, it is the 11th most common type of cancer among women3. Finland has created the "Cancer Society of Finland" which is responsible for training and qualifying professionals to track precursor lesions and is currently one of the countries with the lowest incidence of cervical cancer4.
Other strategies for the prevention of cancer and HPV infection are immunization, changes in lifestyle and early detection through cervical cytology. Moreover, treatment of early-stage cervical cancer has reduced the incidence of invasive carcinoma in several countries of the world2.
The nurse, in this context, plays a crucial role in the control of cervical cancer incidence and mortality, since it is the professional who works in health education, clarifies the fears related to Pap smear, makes an active search of the women who are late in collecting the cytology and performs the screening through preventive examination5.
In contextualizing the health-disease process, health professionals should broaden their view beyond the biological and individual dimension and understand that women have an important social and historical role6. The early diagnosis and participation of women in prevention programs is important, specifically those belonging to vulnerable groups, and there should be investment in reducing barriers to access and use of programs.
In this sense, when investigating the potential of health problems and their relation to cervical cancer, we have been stimulated to understand in depth how these factors are becoming part of the daily life of women. Thus, the present study aims to raise the set of individual, social and programmatic characteristics that have made women vulnerable to cervical cancer.
METHODOLOGY
This is a descriptive and cross-sectional study carried out at the Oncology Gynecology Outpatient Clinic of the Hospital das Clínicas, School of Medicine of Botucatu, interior of São Paulo State, Brazil.
The sample was included for convenience and comprised of 99 women with cervical cancer in follow-up and treatment at the hospital where the study was performed. The data collection took place between November 2014 and July 2015 and was guided by the application of a questionnaire structured and elaborated by the researchers. In order to obtain the characterization of the women, this was composed by statements directed to the sociodemographic and individual aspects of the participants and the programmatic actions of the health services.
The inclusion criteria of the study were: women diagnosed with cervical cancer under follow-up and/or treatment at the Hospital das Clínicas of the School of Medicine of Botucatu, who attended on the day of the scheduled visit and consented to participate in the study and were in clinical conditions to answer the questionnaire about the perception of vulnerability to the disease, knowledge regarding cervical cancer and health actions aimed at the follow-up of the disease and care.
The Oncology Gynecology Outpatient Clinic works every Friday, from 8 to 12 a.m., and the data collection was performed on this day and time and in a room provided by the nursing team.
The data related to the characterization of the women were allocated in a Microsoft Excel 2010 spreadsheet and later the statistical analysis was performed. For the characterization of the sample, the descriptive statistics and the variables presented in tables containing the relative (%) and absolute (N) frequencies were used. Considering a margin of error of 10% and a reliability of 95%, the minimum sample size was 96 patients.
The study complied with the formal requirements contained in national and international regulatory standards for research involving human subjects. It was approved by the Research Ethics Committee of the Faculty of Medicine of Botucatu, under no. 607.268 on April 7, 2014.
RESULTS
Among the women participating in this study and having a confirmed diagnosis of cervical cancer, the age at diagnosis was between 21 and 78 years of age. The predominant age group (60.6%) was between 40 and 57 years and two women were under the age of 25.
Table 1 describes the sociodemographic characteristics of the women followed at the Gynecology Outpatient Clinic of the Hospital das Clínicas, School of Medicine of Botucatu. Regarding the origin by Regional Health Departments (RHD) and health regions, 92.2% (n = 92) of the study sample belonged to RHD VI (health regions: Pólo Cuesta and Vale do Jurumirim and Bauru ), for which the Hospital das Clínicas of Botucatu is a reference in the health service. It was also verified that seven women belonged to other RHDs: II (municipality of Guararapes, health region: Araçatuba/SP), VII (municipality of Holambra, region of Campinas/SP), IX (Marília/SP), XVI (municipalities of Cerquilho, Sorocaba and Tatuí, region of Sorocaba/SP). As for self-reported color, the majority (67.7%) said to be white. It was also observed that 74.7% had elementary education. In relation to religion, the majority (98.0%) declared to be religious and of these, 62.7% were Catholic. Marital status or a stable relationship was predominant (52.6%). Regarding family income, 69.7% reported receiving between one and two minimum wages. Regarding the place of residence, 67.7% lived in their own house. It was also observed that 70.7% of the women were economically active professionals before the diagnosis of cervical cancer and that after the discovery and treatment of the disease only 36.4% continued to perform paid professional activities. It is noteworthy that, after cancer, some women retired, were on sick leave or were discharged from their employment, and others changed their profession, becoming autonomous professionals.
Table 1: Sociodemographic characteristics of the women, Hospital das Clínicas, School of Medicine of Botucatu, 2015.

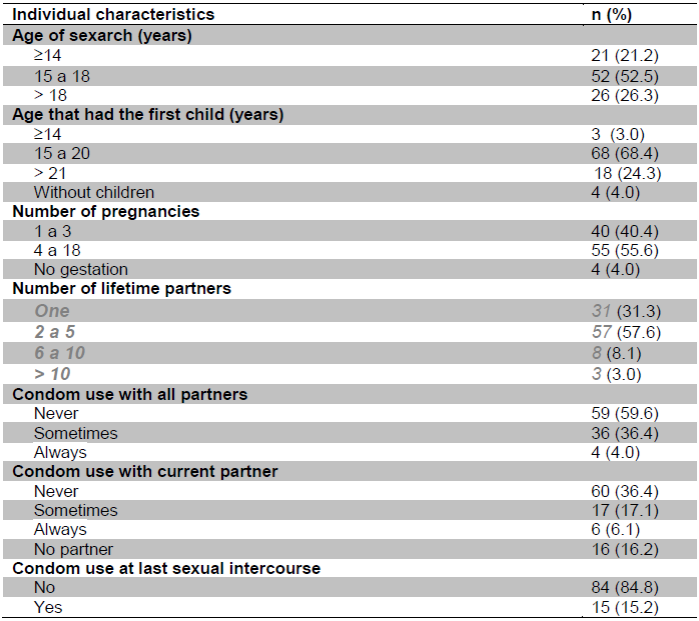
Regarding individual characteristics, most participants had their first sexual intercourse (52.5%) between 15 and 18 years, emphasizing that 21.2% initiated sexual activity with age less than or equal to 14 years. Regarding the age that they became mothers for the first time, it was observed that 68.7% were in the age range between 15 and 20 years. Still, a significant number of women (55.6%) had four or more pregnancies. As for the number of sexual partners during life, 31.3% had only one partner and 57.6% had two to five. Regarding the use of condoms with all partners, 59.6% never used it and only 4.0% have always used it. When questioned if they use a condom with their current partner, 60.6% had never use it and the majority (84.8%) reported that during the last sexual intercourse they did not use the condom. Data are reported as follows (Table 2).
Table 2: Individual characteristics of women, Hospital das Clínicas, School of Medicine of Botucatu, 2015.
Regarding the programmatic characteristics presented in Table 3, it was evidenced that, before being diagnosed with cervical cancer, 45.5% of the women reported performing the preventive examination once a year; however, 31.3% had never collected cytology. As they are still in follow-up, most (57.6%) started to take the exam once a year and the others every six months or four months or quarterly. When questioned about whether they had any difficulty in scheduling the Pap smear test, 97.0% confirmed that they did not, and those who presented difficulties, reported it was due to lack of professionals in the health unit to take the exam and for not having a date in the schedule to perform cytology collection. Regarding the reasons for seeking the health service, only 27.3% said they did not present any gynecological complaints and sought the health unit as a routine visit. Most of the women sought the health service after symptoms of the disease and the main complaints were: pelvic pain, bleeding between cycles or after sexual intercourse or after menopause, leucorrhoea, dyspareunia and hemorrhage. Regarding the interval between the search for the health service, the discovery of the disease and the beginning of treatment, in 79.8% of the women this period was equal to or less than one month.
Table 3: Programmatic characteristics of the health services, Hospital das Clínicas, School of Medicine of Botucatu, 2015.

*Data exceeded 100% because some women had more than one answer;
**Burning, painful urination, pain in the vagina, cystocele, low back pain, weakness, condyloma, weight loss.
According to women, surgical treatment (hysterectomy - 32.3%) predominated, but it was also shown that radiotherapy and brachytherapy were associated with other types of treatment, such as chemotherapy, hysterectomy and conization. Some women also stated that after treatment they started to present other comorbidities, such as intestinal changes (diarrhea and constipation), urinary incontinence and motor difficulty.
DISCUSSION
Potential aspects of illness and injuries to cervical cancer depend on social, environmental, political and economic conditions, that is, on biological and behavioral characteristics of the subjects. When identifying these aspects, we sought to find solutions for effective prevention of the health of women in situations of vulnerability.
Regarding the survey of individual characteristics, this study identified that the age of diagnosis corroborated with the National Cancer Institute. The appearance of invasive cervical cancer in women up to 24 years is very low and screening is not effective in detecting it. Treating these lesions before the age of 25 would lead to a significant increase in colposcopy, would increase the risk of obstetric and neonatal morbidity associated with future gestation, and at this age there is a high probability of the disease regressing. Still, women aged between 50 and 64 years and with normal cytopathological examination present an 84% reduction in the risk of developing an invasive carcinoma between 65 and 83 years old2.
In the majority of women, the first sexual intercourse and motherhood occurred during the adolescence phase. Also, the women of study had had more than one child. This study confirms that having the first sexual intercourse at early age is mainly associated with being black, daughter of adolescent mother and separated parents, having low educational and socioeconomic level, low self-esteem, lack of confidence, media influence, lack of knowledge about sexually transmitted infections, influence from the society and the environment in which they live, lack of dialogue with parents, insistence of the partner, lack of sex education at school, unemployment, use of drugs and alcohol, not practicing religion and influence of friends who have had sexual intercourse7.
Gestation was also a factor associated with infection due to the high prevalence of the virus in this population. It is believed that pregnancy may interfere with HPV infection due to immune and hormonal changes. It is known that high levels of steroid hormones produce decreased synthesis and activity of lymphocytes and macrophages. Thus, during pregnancy, there is transient and selective depression of cellular immunocompetence. Helper and suppressor T lymphocyte activity is decreased, as well as IgG and IgA activity in the cervical mucus8.
Gestation, due to maternal changes, such as hormonal and immune changes, is considered a risk factor for HPV infection, with cervical cancer being the most common among the other types associated with pregnancy. Pregnancy causes imbalance in the vaginal flora, increasing the vulnerability to contamination of infectious agents and HPV8.
Having had the first sexual intercourse under the age of 15, multiple partners and sexual intercourse without a condom was responsible for exposure to HPV infection and increased vulnerability to cervical cancer in institutionalized women in a female penitentiary9. Also, women with HPV and other infections are more susceptible to health problems and, in this case, to the faster development of invasive cervical carcinomas2.
With regard to social characteristics, there was a predominance of white color (self-declared color), complete or incomplete elementary education, Catholic, married, family income between one and two minimum wages and having their own house.
In the Ethiopian capital, a study showed that the majority of the patients were married (51%) and illiterate (52%). Also, socioeconomic aspects such as level of schooling, income and occupation influence women's decision-making because of their economic dependence on the spouse and they are more exposed to HPV infection because they have difficulty understanding cervical cancer vulnerability factors. These women also perform less frequently the preventive examination and are less conscious about the complications resulting from the disease, which increases the chance of late diagnosis10. Other research found that most women with cervical lesions were married (75%), white (31.82%), had low educational level and unfavorable socioeconomic status11.
It has been proven that religious practice influences women’s behavior, encouraging healthy habits. Many churches, especially those located in impoverished regions, have assumed an important social role and, through educational activities, have developed with their practitioners actions aimed at prevention and health promotion12.
Concerning the participation of women as an active professional before and after diagnosis and treatment, this study showed that most stopped working after the illness.
In England, a study addressed the negative effect of work on cancer patients and showed that 17% of post-treatment subjects are less likely to work or work an average of 5.6 hours less per week. It has also been shown that returning to work occurs at least one year after the end of treatment13.
The programmatic characteristics of the health services allowed us to identify that women were more concerned about their health after cervical cancer.
Poor adherence to Pap smear is an important barrier to early diagnosis, but it has been overcome by some women who attach cancer to a fatal disease and thus carry out the examination. However, when the woman has no symptoms of the disease or does not understand the importance of screening, noncompliance with the routine examination becomes more evident. Such behavior is significant for the increased incidence and mortality of late diagnosed women14-15. It has been reported that a quarter to a third of the female population does not feel the need to perform cytopathological examination due to the absence of symptoms16.
Periodic cytopathological examination has been, up to this date, the best way to screen for cervical cancer and reduce mortality among women who are vulnerable to the disease. However, screening is effective in an organized system to monitor and treat the female population, able to assist them comprehensively and provide quality care2.
Regarding the beginning of treatment after the diagnosis of cancer, it is up to the primary care services to refer patients immediately to specialized services, as primary care services are responsible for proposing actions to promote and protect health, prevent diseases, early diagnosis, rehabilitation and maintenance of health in the collective and individual dimensions. Therefore, primary care has the responsibility to organize reference and check counter-reference2.
Regarding the type of treatment, hysterectomy, radiotherapy and brachytherapy were the most frequent in this study. Compared to other types of cancers, it is the treatment that has the best response to invasive disease prevention and cure. If the disease is diagnosed early and the treatment is performed correctly, there are chances to regress, almost totally, the development of the disease, because its evolution is slow and gradual17.
CONCLUSION
The survey of sociodemographic, individual and programmatic characteristics allowed us to identify which risk factors for cervical cancer were predominant and contributed to the vulnerability to this disease, such as first sexual intercourse at early age, non-use of condoms, low educational level and family income and failure to perform the Pap smear test.
However, a possible limitation of this study is the fact that some women had been diagnosed with cervical cancer a few years ago. We believe that the period between diagnosis and data collection may have led to difficulties in remembering some characteristics in relation to their previous sexual life, but because they have still been followed up at the Oncology Gynecology Outpatient Clinic, they were certainly able to describe social aspects and those concerning the organization of health services and their participation in the treatment and tracking of other changes in their health status.
When considering women's perception on the characteristics that made them vulnerable to cervical cancer, it is necessary to develop effective care interventions guided by the concept of comprehensiveness of care. Investment in prevention through immunization and orientation on safe sexual practices is the best strategy and should be associated with early screening and treatment of precursor lesions for cervical cancer.
Therefore, this reinforces the importance of organizing screening programs, diagnosis and early treatment, health actions by a multidisciplinary team, ongoing education and qualified care planning.
REFERENCIAS
1. Silva MRB, Silva GP. O conhecimento, atitudes e prática na prevenção do câncer uterino de uma unidade da zona oeste Rio de Janeiro. Rev Pesqui Cuid Fundam. 2012;4(3):2483-92. [ Links ]
2. Instituto Nacional de Câncer José Alencar Gomes da Silva (BR). Coordenação de Prevenção e Vigilância. Divisão de Detecção Precoce e Apoio à Organização de Rede. Diretrizes brasileiras para o rastreamento do câncer do colo do útero. 2a ed. Rio de Janeiro: INCA; 2016. [ Links ]
3. Wiedmeyer ML, Lofters A, Rashid M. Cervical cancer screening among vulnerable women: factors affecting guideline adherence at a community health centre in Toronto, Ont. Can Fam Physician. 2012;58(9):e521-6. [ Links ]
4. Finnish Cancer Registry. Institute for Statistical and Epidemiological Cancer Research. Cervical cancer screening [Internet]. Helsinke: Finnish Cancer Registry; 2016 [citado 23 Nov 2016]. Disponível em: http://www.cancer.fi/syoparekisteri/en/mass-screening-registry/cervical_cancer_screening/ [ Links ]
5. Oliveira MAC, Pereira IC. Atributos essenciais da Atenção Primária e a Estratégia Saúde da Família. Rev Bras Enferm. 2013;66(esp):158-64. [ Links ]
6. Prestes CRS, Paiva VSF. Psychosocial approach and health of black women: vulnerabilities, rights and resilience. Saúde Soc. 2016;25(3):673-88. [ Links ]
7. Lara LA, Abdo CH. Aspectos da atividade sexual precoce. Rev Bras Ginecol Obstet. 2015;37(5):199-202. [ Links ]
8. Oliveira GR, Vieira VC, Barral MFM, Döwich V, Soares MA, Conçalves CV et al. Risk factors and prevalence of HPV infection in patients from Basic Health Units of an University Hospital in southern Brazil. Rev Bras Ginecol Obstet. 2013;35(5):226-32. [ Links ]
9. Anjos SJSB, Ribeiro SG, Lessa PRA, Nicolau AIO, Vasconcelos CTM, Pinheiro AKB. Fatores de risco para o câncer de colo do útero em mulheres reclusas. Rev Bras Enferm. 2013;66(4):508-13. [ Links ]
10. Tadesse SK. Socio-economic and cultural vulnerabilities to cervical cancer and challenges faced by patients attending care at Tikur Anbessa Hospital: a cross sectional and qualitative study. BMC Women´s Health. 2015;15(75):1-12. [ Links ]
11. Dias EG, Santos DDC, Dias ENF, Alves JCS, Soares LR. Perfil socioeconômico e prática do exame de prevenção do câncer do colo do útero de mulheres de uma unidade de saúde. Rev Saúde Desenvolv. 2015;7(4):135-46. [ Links ]
12. Ribeiro FML, Minayo MCDS. O papel da religião na promoção da saúde, na prevenção da violência e na reabilitação de pessoas envolvidas com a criminalidade: revisão de literatura. Cien Saúde Colet. 2014;19(6):1773-89. [ Links ]
13. Candon D. The effects of cancer on older workers in the English labour market. Econ Hum Biol. 2015;18:74-84. [ Links ]
14. Vrinten C, McGregor LM, Heinrich M, von Wagner C, Waller J, Wardle J, et al. What do people fear about cancer? A systematic review and meta-synthesis of cancer fears in the general population. Psycho-Oncology. 2016 Sep 19. doi: 10.1002/pon.4287.Review. [ Links ]
15. Carvalho ILN, Nunes RB, Sousa IDB, Batista RDC, Sousa ASJ, Sousa CS. Exame citopatológico: compreensão de mulheres rurais acerca da finalidade e do acesso. Rev Rene. 2016;17(5):610-7. [ Links ]
16. Wijkerslooth TR, Haan MC, Stoop EM, Bossuyt PM, Thomeer M, Leerdam ME, et al. Reasons for participation and nonparticipation in colorectal cancer screening: a randomized trial of colonoscopy and CT colonography. Am J Gastroenterol. 2012;107(12):1777-83. doi: 10.1038/ajg.2012.140. [ Links ]
17. Araújo AO, Lira ACB, Fortes CMMS, Ribeiro JF, Barros RGM. Perfil clínico e epidemiológico da mulher idosa com câncer de colo do útero em Teresina-PI, 2008-2012. Rev Multiprof Saúde Hosp São Marcos. 2013;1(2):4-13. [ Links ]
Received: July 27, 2017; Accepted: October 13, 2017
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
