










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.17 no.52 Murcia oct. 2018 Epub 01-Oct-2018
https://dx.doi.org/10.6018/eglobal.17.4.309091
Originals
Predictors for moderate and serious pre-operatory anxiety in hospitalized surgical patients
1 Máster en Enfermería. Facultad de Enfermería de la Universidad Federal de Goiás (UFG). Brasil. lorena_melchior@hotmail.com
2 Doctora en Enfermería; Docente de la Facultad de Enfermería de la UFG. Brasil.
3 Residente de Enfermería del Hospital de las Clinicas-UFG. Brasil.
Main goal
Estimate the prevalence of anxiety and the predictors for moderate and serious pré-operatory hospitalized surgical patients.
Methods
cross-sectional analytical study. The population was constituted of surgical hospitalized patients, sample of 200 pacient, after the sample calculation. For analysis, the Pearson's Chi-square test and the Gross and Adjusted Poisson Regression were used.
Results
The prevalence os pré-operatory anxiety was 53,0% (n=106) (IC 95% 46,06/59,85), being that 33,0% (n=35) (IC 95% 24,5/42,3) of the pacients presented moderate and serious anxiety . Multivariate analysis, gender, occupation and fear of anesthesia remained significant, setting in predictors. Although the fear of anesthesia didn’t maintain, when assessing the categories separately, the fear of errors showed a significant relationship with moderate and severe anxiety in the adjusted model.
Conclusion
In the present study, the prevalence of anxiety is high. The gender, occupation, the fear of anesthesia and the fear of errors during anesthetic-surgical procedure are set in predictors for moderate and severe anxiety in the preoperative period. The profile of an anxious pacient at moderate and severe levels was male, age ranging from 50 to 69 years old, low education level, married, in unstable work situation (no signed or unemployed), residents in Goias and in homes where the sole provider of the home was the patient, submitted to previous surgeries and with preoperative hospitalization time of less than 24 hours.
Keywords: Nursing; Anxiety; Surgery; Perioperative nursing
INTRODUCTION
Anxiety is a vague and unpleasant feeling of fear, apprehension, characterized by tension or discomfort derived from anticipation of danger or something unknown. Such aspects of anxiety can be measured through the use of instruments such as the Hamilton anxiety scale, Beck’s inventory, the Hospital Anxiety and Depression Scale and others. These are intended to evaluate the patient's anxiety at certain moments, as well as in the preoperative period, contribute to delineate the anxiety levels of the surgical patient, classifying it in mild, moderate and severe levels 1)(2)(3 .
The measurement of the level of anxiety for many decades was considered complex, motivating several researchers to describe different methods for quantifying it, which is accomplished through various tools. Among the tools available, Hamilton's anxiety scale currently has consistent results. The Scale evaluates 14 items, the first seven items are related to the symptoms of anxious mood and the other seven to physical symptoms. A score is obtained by summing up resoective items, whose score can vary from 0 to 56, ranging from zero to 17, normal anxiety, from 18 to 24, mild anxiety, from 25 to 29 moderate anxiety and> 30, severe anxiety 4 .
Any state of anxiety in the preoperative patient is worrisome, and at moderate and severe levels, the impact on patient safety can be intensified, and make the moment propitious to unexpected events, impact the surgical outcome, or the possibility of suspending the surgery. Moreover, it can generate feelings and irrational attitudes about various situations and moments related to the procedures necessary to the anesthetic-surgical process2)(5)(6 ..
The anesthetic-surgical process is complex and critical, most often, a sudden and imposed reality, which causes profound changes in the life of the patient and his family. It has implications on the well-being and health, as well as the fundamental standards of life in individual and family level5)(6 .
In the perioperative period, the anxiety becomes recognized as worrying for the health team when presented in above normal levels, because reactions may be disproportionate to the stimulus and interfere with quality of life, emotional comfort, and daily performance. The patient becomes predisposed to difficult venous access, the rigidity of the jaw in anesthesia induction, autonomic and hemodynamic fluctuations, requiring larger doses of anesthetics and other drugs. In the postoperative period, anxiety has been related to pain, nausea and vomiting, delayed recovery and consequent increased risk of infection2)(7 .
Concern about patient safety in the perioperative period is currently a challenge. There are several worrying aspects related to this moment, one of them undoubtedly permeates the control of anxiety. To know the predictors, profile, characteristics, signs and symptoms of the anxious patient in the preoperative period, provide support for action planning and evidence-based nursing care. It is believed that the nursing action directed from this knowledge will contribute to reduce the anxiety levels, providing conditions for the patient to have cooperative behavior, and confident the coping of the perioperative process.
GOAL
Identify moderate and severe anxiety predictors and the anxious patient profile in the preoperative period of elective surgery.
MATERIALS AND METHODS
The research project was approved by the Research Ethics Committee of the Hospital das Clinicas, Federal University of Goiás (protocol number: 1685138) and ethical aspects were contemplated. Participants agreed to be part of the research after reading the Informed Consent Term and informed about the objectives and purposes of the research. No reward was offered to the subjects, but assured the confidentiality of their identity.
Design, place of study and period
Cross-sectional and analytical study, held in a large university hospital, of tertiary level and attendance of medium and high complexity, located in the center west region of Brazil, in the period June-September of 2016.
Population, inclusion and exclusion criteria
The reference population consisted of patients admitted to the surgical clinic of the hospital and with scheduled surgeries. The sample consisted of 200 patients obtained after the sample calculation in the software G.Power, considering the type of the study, 5% absolute error, design effect of 0.1 and test Power of 86%. It was considered as inclusion criteria, the age range from 18 years, is classified according to the American Society of Anesthesiologists (ASA) <IV, meet lucid, verbalizing and satisfactory clinical conditions for the interview; being in the preoperative period in advance of up to 36 hours of the scheduled surgery.
Study Protocol
Three instruments were used to collect data. A structured questionnaire containing socio-demographic, clinical and surgical variables prepared for the study and validated the form and relevance of the items; The Hamilton anxiety scale 4 , and the numerical scale of pain 8 . Hamilton Anxiety Scale consists of 14 items of four points (0 = none and 4 = maximum), has two groups with seven items each, the first related to the symptoms of anxious mood (1-7) and the second to physical symptoms of anxiety (8 to 14). The total score is obtained by summing the values (levels) given in items, the result of which can vary from 0 to 56, and from zero to 17, the normal anxiety; 18 to 24, mild anxiety; 25 to 29, moderate anxiety and 30 or more, severe anxiety 4 .
The numeric pain scale is a numbered ruler from 0 to 10, presented to the patient horizontally and vertically, which measures the intensity of the perceived pain, in which a zero value is "no pain" and 10 "Pain Maximum" 8
Eligible patients who agreed to participate were interviewed individually on average for 30 minutes in their own bed, with the prior authorization of Nursing Manager and presentation of the study objectives, highlighting the importance of the results for deepening and knowledge of the subject in that context.
Result Analysis and Statistics
All data were cataloged and organized into formatted Excel spreadsheet program. Statistical analysis was performed using SPSS software, version 20.0. The population characterization was done by calculating the absolute and percentage frequencies. The Pearson Chi-square test was performed to assess the association between the independent variables and the outcome. The level of significance was 5%. The prevalence ratio (PR) was evaluated by gross and adjusted Poisson regression. The variables with p≤0.20 in the crude analysis were used as the setting for the final model.
RESULTS
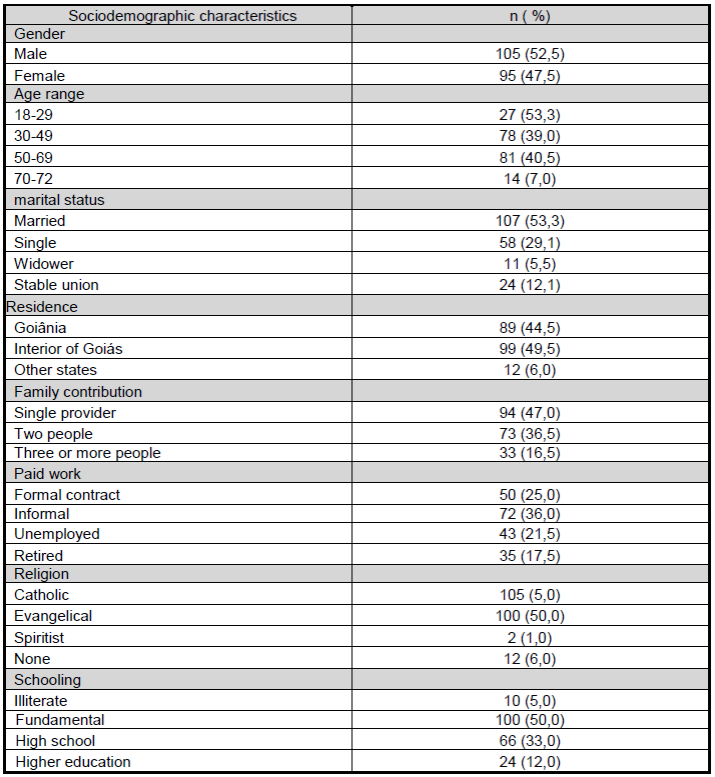
The study sample consisted of 200 preoperative patients. The ages ranged from 18 to 72 years, 40.5% (n = 81) had between 50 and 69 years, and nearly half, 49.5% (n = 99) resided in the state of Goias. As for education, 55.0% (n = 110) had less than nine years of study and, with regard to income, 47.0% (n = 94) were the only providers of home, of these 38.2% (n = 36 ) did not formally work (Table 1 ).
Table 1 Sociodemographic profile of preoperative patients in the surgical clinic of the hospital. Goiânia-GO, 2016.
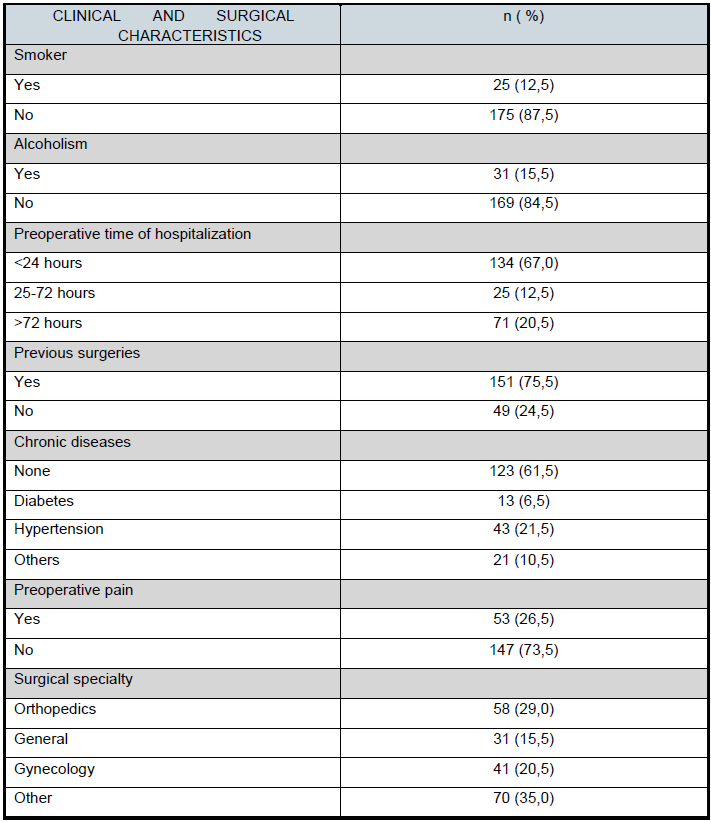
Regarding the clinical and surgical characteristics of the sample, 61.5% (n = 175) were non-smokers, 84.4% (n = 169) non-alcoholics and 75.5% (n = 151) had prior surgical experience. The three most frequent surgical specialties were orthopedics, gynecology, and general surgery, 29.0%, 20.5% and 15.5%, respectively. The preoperative time of hospitalization was less than 24 hours in 67% (n = 134) and 26.5% of cases (n = 53) reported the preoperative pain (Table 2 )
Table 2 Clinical and surgical profile of patients in the preoperative surgical clinico of the hospital. Goiânia-GO, 2016.
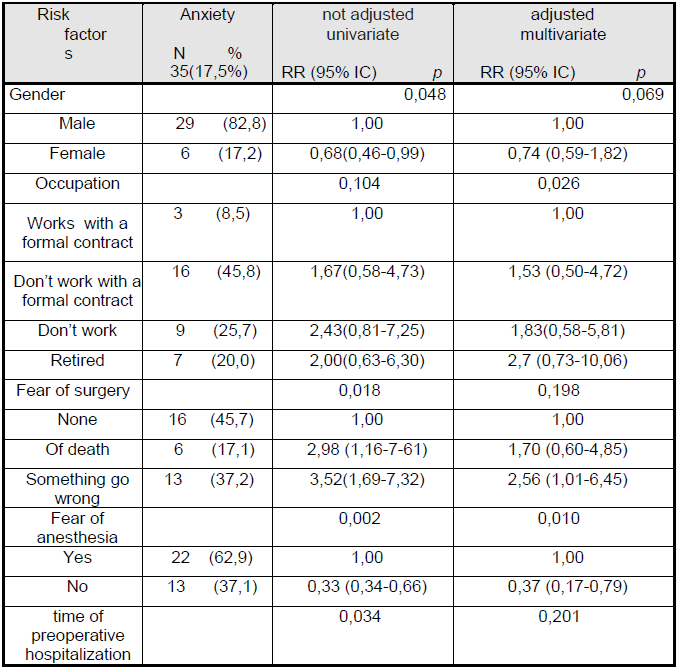
The prevalence of preoperative anxiety was 53.0% (n = 106) (95% CI 46.06 / 59.85), with 33.0% (n = 35) (95% CI 24.5 / 42 3) patients had moderate to severe anxiety. The bivariate analysis revealed a significant association between moderate and severe preoperative anxiety, and sex, occupation, fear of surgery (figure 1 ) fear of anesthesia and the time of preoperative hospitalization (table 3 )
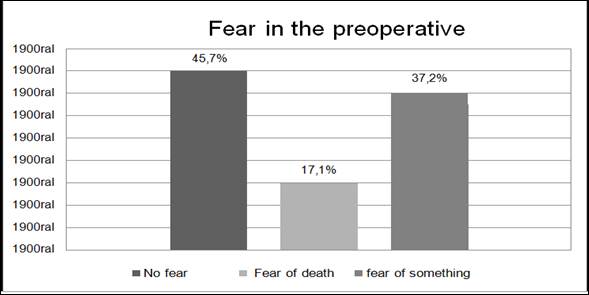
Figure 1 Fears reported by patients hospitalized in preoperative surgical clinic of the hospital. Goiânia-GO, 2016.
In the multivariate analysis, the sex, the occupation and the fear of the anesthesia, remained significant, being configured as predictors. Although the fear of surgery did not remain in the adjusted model, when evaluating the categories separately, the fear of errors in surgery, showed a significant relationship with moderate and severe anxiety. Thus, the prevalence of this type of anxiety is 2.56 (1.01 / 6.45) times higher than in those patients who did not report fears (Table 3 ).
The profile of patients who presented moderate and severe preoperative anxiety was individuals aged between 50 and 69 years (51.5% / n = 18); of low schooling (65.7% / n = 23); male (82.8% / n = 29), married (57.2% / n = 20). In unstable work situation (without a formal contract and / or unemployed) (71.5% / n = 25), in single home providers (63.0% / n = 22), residents of the interior of Goiás (74.6% / n = 26), submitted to previous surgeries (71.5% / n = 25) and preoperative time of hospitalization <24 hours (62.8% / n = 22) (Table 3 ).
DISCUSSION
Hospitalization constitutes a difficult experience to be faced by the individual and functions as a stressing agent, since it distances the person from their physical and social environment and introduces changes in daily life, eliminating privacy and intimacy. In addition, anxiety is also present in hospitalized patients, and the circumstance of being submitted to anesthesia-surgical procedure are even more striking, due to stigmatized changes in health status, uncertainties regarding recovery and fears related to that moment2)(9 .
The prevalence of pre-operative anxiety in the study was 53.0%, and the prevalence of moderate and severe anxiety was 33% among anxious patients, similar to the findings of a cross-sectional study in Pakistan 10 .
This study found in the regression analysis, as predictors for anxiety: sex, occupation, fear of anesthesia and fear of errors in the surgical anesthetic procedure. A cross-sectional study with a similar population conducted by Yilmaz in 2012 in Turkey showed correlations between preoperative anxiety level, sex, schooling, marital status, magnitude of operation and social support, however there were no references to the variables related to fears2 . The varibles: low level of schooling and social support, which evolves the approach with the family, were also present in the profile of patients anxious of this study, although it was not maintained in the regression analysis.
A cross-sectional study conducted in 2014 at a university hospital in Ethiopia raised the predictors for preoperative anxiety and identified as factors associated with fear: fear of death, fear of the unknown, being divorced, time to prepare for surgery, and income 11 . The data are similar to the findings of this study, because the fears of patients and income can influence in the onset of anxiety, and most anxious patients were unstable situation at work. On the other hand, the time of preoperative hospitalization for surgery was related to anxiety in the bivariate analysis.
Regarding the anxious patient profile of this study, the age range of 50-69 years, therefore includes the elderly, resembles the prospective two-year study, conducted from January 2011 to February 2013, at the University Urology Department of Ferrara, Italy. It was observed significant correlation between being old and present anxiety due to fear of cancellation or own cancellation of elective surgery12 .
Anxiety levels may be associated with the level of formal education, since a large part of the anxious at moderate and severe levels, as well as generally anxious of the study, were of low schooling. Another cross-sectional study also showed lower levels of anxiety among patients with more than 12 years of schooling. Individuals with a higher educational level can estimate surgery more accurately, and those with a lower level may be afraid of the unknown and generate such feelings of fear 2)(7 .
Several studies have estimated a higher prevalence of mild anxiety in female patients, as well as when analyzing the total anxiety rate of this study 2)(10)(11 . However, when moderate and severe anxiety are analyzed, the correlation occurs in males. It is believed that the concern with maintaining the home and family, as much of the sample was only providers of home and in informal work situations or unemployed, whose income depends on their autonomy and maintenance of good health.
The fact that the most anxious patients reside in surrounding municipalities to the place of hospitalization can be an obstacle to maintaining social relationships. Often the lack of support in coping with unstable health times, can exacerbate anxiety, making it moderate and severe. This requires an individualized and sensitive plan by the nursing team to provide subsidies that help these patients to go through the perioperative period with lower levels of anxiety 9)(13)(14 .
Regarding previous surgeries, the results are in agreement with the findings of the cohort study of Santos et al., which identified the most prevalent anxiety in the preoperative period of the patient when correlated with the history of previous surgeries. Similarly, the cross-sectional study by Ribeiro argues that patients with experience have more preoperative anxiety. Such association may be related to negative experiences such as complications, infections, unresolved fears, or even low trust with the team. Currently, several studies seek measures to know some mechanism that helps to minimize preoperative anxiety, for example, the application of interventions and learning measures that contribute to the mitigation of this impact9)(14)(15).
According to Ribeiro although hospitalization for scheduled surgeries is increasingly close to the day of surgery, it is necessary that the health team provide emotional support and previous guidelines for surgical preparation. The first hours of hospitalization represent an adjustment phase, in which the patient enters the hospital, and this time surrounded by feelings and fears. If unqualified, these feelings may stand out and the patient be referred to the operating room while remaining highly anxious.
Anxiety acts on the body, producing changes in vital signs and can cause cancellation or suspension of surgery which, in turn, can lead to increased anxiety and become a vicious cycle. The practice of nursing in the preoperative period regarding the emotional care of the surgical patient is of as relevant importance as the physical preparation. A prospective exploratory study at a large private hospital in the state of São Paulo identified the nursing diagnosis of anxiety in patients preoperatively below those who underwent the preoperative nursing visit 6)(16 .
The preoperative evaluation aims to reduce patient anxiety and improve postoperative surgical outcomes, being a vital part of the patient's general management plan. It ensures the ability to undergo elective surgery, including an emotionally prepared patient. Any conditions which may affect the operation may be recognized and treated prior to reducing the rates of unnecessary surgical suspensions. This will minimize unnecessary costs and reduce patients' stress and anxiety 17)(18 .
From this perspective, nursing care for the surgical patient with an emphasis on their emotional aspects should be conducted in an individualized way. It is necessary a sensitivity and knowledge of the staff, for patients who present moderate and severe anxiety levels, since they are more worrisome, due to the repercussion that may occur in the perioperative period. Therefore, it is necessary to plan actions and implement them from the patient's reception in the hospital until discharge, aiming at a safe and quality care 3)(14 .
CONCLUSION
In the present study, the prevalence of anxiety at moderate and severe levels were 33% among the anxious and 17.5% in the overall sample. Gender, occupation, fear of anesthesia and the fear of errors during anesthetic-surgical procedure are configured in predictors of anxiety at high levels in the preoperative period.
REFERENCIAS
1. Fioravanti ACM. Propriedades psicométricas do inventário de ansiedade traçoestado (IDATE) [dissertation]. Rio de Janeiro: Departamento de Psicologia/Pontifícia Universidade Católica do Rio de Janeiro; 2006. 66 p. [ Links ]
2. Yilmaz M, Sezer H, Gürler H, Bekar M. Predictors of preoperative anxiety in surgical inpatients. Journal of clinical nursing. 2012; 21(7-8): 956-64. [ Links ]
3. Renouf T, Leary A, Wiseman T. Do psychological interventions reduce preoperative anxiety?. British Journal of Nursing. 2014; 23(22): 1208-12. [ Links ]
4. Hamilton M. The assessment of anxiety states by rating. Br J Med Psychol.1959; 32(1): 50-5. [ Links ]
5. Ortiz J, Wangb S, MacArthur A, Elaydabe DT. Informação pré-operatória ao paciente: podemos melhorara satisfação e reduzir a ansiedade? Rev. Bras. Anestesiol. 2015; 65(1): 7-13. [ Links ]
6. Gonçalves TF, Medeiros VCC. A visita pré-operatória como fator atenuante da ansiedade em pacientes cirúrgicos. Revista SOBECC. 2016; 21(1): 22-7. [ Links ]
7. Caumo W, Schmidt AP, Schneider CN, Bergmann J, Iwamoto CW, Bandeira D et al. Risk factors for preoperative anxiety in adults. Acta Anaesthesiol Scand. 2001; 45(3): 298-307. [ Links ]
8. Sousa FF, Pereira LV, Cardoso R, Hortense P. Escala multidimensional de Avaliação de dor. Rev. Lat Amer Enferm [Internet]. 2010 [cited 2016 aug 22]; 18(1): (09 telas). Available from: http://www.scielo.br/pdf/rlae/v18n1/pt_02.pdf. [ Links ]
9. Machado JA, Silvia LF, Guedes MVC, Freitas MC, Ponte KMA, Silva AL.Autocontrole de ansiedade no pré-operatório cardíaco: resultado de uma intervenção de enfermagem. SANARE jul-dez 2015; 14(2):36-42. [ Links ]
10. Mohammad FJ, Fauzia AK. Frequency of preoperative anxiety in Pakistani surgical patients. J Pak Med Assocjune 2009; 59(6): 360-363. [ Links ]
11. Nigussie S, Belachew T, Wolancho W. Predictors of preoperative anxiety among surgical patients in Jimma University Specialized Teaching Hospital, South Western Ethiopia. BMC surgery. 2014; 14(1):1. [ Links ]
12. Dell'Atti, Lucio. The cancelling of elective surgical operations causes emotional trauma and a lack of confidence: study from a urological department.Urologia. 2014; 81(4): 242-5. [ Links ]
13. Santos MA, Rossi LA, Paiva L, Dantas RAS, Pompeo ECBM. Medida da ansiedade e depressão em pacientes no pré-operatório de cirurgias eletivas. Revista Eletrônica de Enfermagem [Internet]. 2012 [cited 2015 aug 06]; 14(4): 922-7. Availablefrom: https://www.fen.ufg.br/fen_revista/v14/n4/pdf/v14n4a21.pdf. [ Links ]
14. Santos MMBD, Martins JCA, Oliveira LMN. A ansiedade, depressão e estresse no pré-operatório do doente cirúrgico. Revista de Enfermagem Referência. 2014; serIV(3): 7-15. [ Links ]
15. Ribeiro, P. Pré-operatório: O universo da apreensão e desconhecimento: Estudo de factores que influenciam o nível de ansiedade estado do doente no pré-operatório. Revista Investigação em Enfermagem. 2010; 22. [ Links ]
16. Sampaio CEP, Ribeiro DAR, Marta CB, Seabra Júnior HC, Rose E, Francisco MTR. Determinant Factors of the Anxiety and Mechanisms of Coping on General Surgical 69 Procedures. Journal of Research: Fundamental Care Online [Internet]. 2013[cited 2016 nov 15]; 05 (4): 547-55. Available from: http://www.seer.unirio.br/index.php/cuidadofundamental/article/view/3070/pdf_922 [ Links ]
17. Pritchard MJ. Pre-operative assessment of elective surgical patients. Nursing Standard. 2012; 26(30): 51-56. [ Links ]
18. Santos AF, Santos LA, Melo DO, Alves Júnior A. Estresse pré-operatório: Comparação entre pacientes do SUS e convencionados. Psicologia Reflexão e Crítica. 2009; 22(2): 269-76. [ Links ]
Received: November 04, 2017; Accepted: December 07, 2017
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
