










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.17 n.52 Murcia Oct. 2018 Epub Oct 01, 2018
https://dx.doi.org/10.6018/eglobal.17.4.307301
Reviews
The stressors factors in adult patients interned to an intensive care unit
1 Doctoranda en Enfermería por la Universidad Federal do Rio Grande do Sul, RS-l. Docente de la Universidad Federal do Pampa, Uruguaiana, Rio Grande do Sul, RS- Brasil. leticedl@hotmail.com
2 Enfermera del Hospital General de Novo Hamburgo, Rio Grande do Sul- RS Brasil
3 Enfermera Graduada por la Universidad Federal do Rio Grande do Sul-RS. Brasil..
4 Enfermera del Hospital Universitário de Canoas, Canoas, Rio Grande do Sul -RS. Brasil.
The present study is an integrative review of the literature that aims to analyze the available evidence in the literature about the stressors reported by patients hospitalized in an adult intensive care unit. The articles were searched in the databases LILACS, Scielo, PubMed and BDENF published during the period from 1997 to 2015. The articles about the theme at hand have been included in Portuguese and Spanish. The sample consisted of 13 articles, where 40 stressors were identified, categorized as environmental, physiological, emotional / psychological and social, divided into 16 subcategories: unfavorable situations, noise, ineffective thermoregulation, disturbed sleep patterns, impaired bed mobility, impaired verbal communication, pain, lack of attention / individuality, anxiety, fear, loss of autonomy, interrupted family process, impaired social interaction, impotence, feeling of impotence and compromised family coping. It has been verified that the theme is relevant, but still in early stages, considering the nursing care gaps to be implemented. It is evident that when stressors are identified, evaluated and diagnosed by nurses they can be transcribed as nursing care in a plan of individual care to the patient, enabling the recovery and rehabilitation process during hospitalization in the ICU.
Keywords: Nursing Care; Post-Traumatic Stress Disorders; Physiological Stress; Critical Care; Intensive Care Units; Psychological stress
INTRODUCTION
The high specialized and complex technology used in the intensive care units (ICU), when proportionate the continue monitoring of the patient’s health context1 , increases the chances of survivorship of patients under unstable and critical care2 . However, it favors factors that trigger distress among health professionals, hospitalized patients and family3 .
The patient or their relatives’ response to distress is related to the type, intensity and duration of triggering factors, for it leads to psychological chances, such as fear, anxiety, depression and post-traumatic syndrome, as well as physiological instabilities, for example, predisposition to infections and diminishment of wound healing4 . These distress factors get intensified when overage patients get hospitalized via emergency room, for at the most of times they are not prepared to getting ill nor hospitalized, which compromises the course of their lives with social isolation5 .
Among the factors cited by the patients, the structural aspects, such as quantity of technological equipment that the patient uses; organizational aspects of assistance, which demand rigorous control and attention from the patient; social aspects, caused by the family detachment, work and daily activities with the family in their habitual environment; and, finally, but not less important, the psychological factors, such as the risk for incapacity or death were highlighted6)(7)(8 .
Nursing, as part of the ICU, has as major role to diagnose, intervene and seek for resolutions towards distress factors, for one of its objectives is to provide humanized and holistic care, which boosts the establishment of affective bonding and minimize unpleasant feelings in hospitalized patients and their relatives3 . The nursing intervention is any treatment based on the professional judgment and clinical knowledge, which must be performed by a nurse in order to improve patient’s results9 .
Against the foregoing, there is the necessity to identify not only the stressors under the patient’s perspective, but the singularities that triggers the distress, in order to reveal the possible nursing care interventions that may help the patient out in the process of rehabilitation. For such purpose, the objective of this study is to analyze the evidences available on the literature on the distress factors in adult patients hospitalized in an intensive care unit for adults.
MATERIAL AND METHOD
This qualitative study aims to identify the scientific production on the distress factors that are mentioned by patients hospitalized in an ICU for adults. In order to attain the objectives, the RI based on Cooper10 was chosen. This method reunites results from other researched about the same topic, with the purpose to synthetize and analyze these data, developing a more approachable explanation on the studied phenomenon. In what concerns the study design, five steps described by Cooper10 were followed: problem formulation, data collection, data assessment and analysis, results interpretation, and presentation of results. Through the deepening of the thematic and definition of the relevant aspects of this study, the delimitation of the problem was possible, which began with the following question: What is/are the distress factor/s for adult patients in an intensive care unit for adults?
For data collection, the databases Literatura Latino-Americana e do Caribe em Ciências da Saúde (LILACS), Scientific Eletronic Library Online (Scielo), PubMed e Banco de Dados em Enfermagem (BDENF) were used. The descriptors for health sciences from DeCS were in Portuguese and Spanish, which were also separated by the Boolean operator AND. These were: nursing care, post-traumatic syndrome, physiological distress, critical care, intensive care unit, hospitalization, psychological distress, humanized care, psychological resilience, and hospitalized patients.
The inclusion criteria involved nursing articles that approached the topic in the Portuguese and Spanish languages, full-text online available, published from 1997 to 2015, such as annals, national articles on nursing, qualitative or quantitative, theoretical review, integrative review and systematic review. The Intensive Care Unit Environmental Stressor Scale - ICUESS defined the cutoff. This scale was traduced and adapted to the Brazilian context in 1997 by Novaes et al. (11 .
Articles that approached distress factors for children and newborns, or the ones carried out with animals, studies that aimed the professional or relatives’ perspective on distress factors, studies available in audio or video, and the ones that were not available online were excluded.
For the assessment and recording of data extracted from the scientific articles, a form was elaborated for individual assessment, which contained the following information: identification of the article (title, country, authors and their own titles, periodic, year, volume, number, descriptors/keywords); objective/question of the study; population; methodology, results (related to the problem question).
For data analysis and results interpretation, a general synoptic chart was elaborated, which enabled the grouping of distress factors by similarity.
Considering the ethical aspects, authorship and ideas, concepts and definitions of the authors of the analyzed productions were assured, which should be presented in a trustworthy way, described and quoted according to the precepts of Law no. 9610/98.
RESULTS AND DISCUSSION
The sample constituted in 973 articles, from which 960 were excluded because it did not contemplate the theme, the inclusion criteria, or it was repeated. After the profound reading of the publications, the selected sample was 13 articles, from which four were from LILACS, weight from BDENF, one from SciELO, and none of them from PUBMED. The accentuated number of excluded publications happened for the deficit of productions that discussed the subject under patient’s perspective.
Regarding the year of publication, articles from 2002 to 2015 were found. It was possible to notice a predominance of studies in 2007, 3 articles (23.07%), and the lack of publications from 1997 to 2005. Moreover, there was only one publication in 2015. This result demonstrates that the period of articles publication grouped itself mainly from 2007 to 2011, and did not present correlation with the publication and validation of ICUESS in 1997.
In what concerns the country of origin, it was possible to notice that the distress factors still are incipient among Brazilian articles, being found 12 publications, mainly among Spaniards, for only one scientific publication was found on the topic. This interference betakes the necessity to focus on the point of view of patients8 , taking as a premise the beliefs, values and expectations of their experience in an ICU.
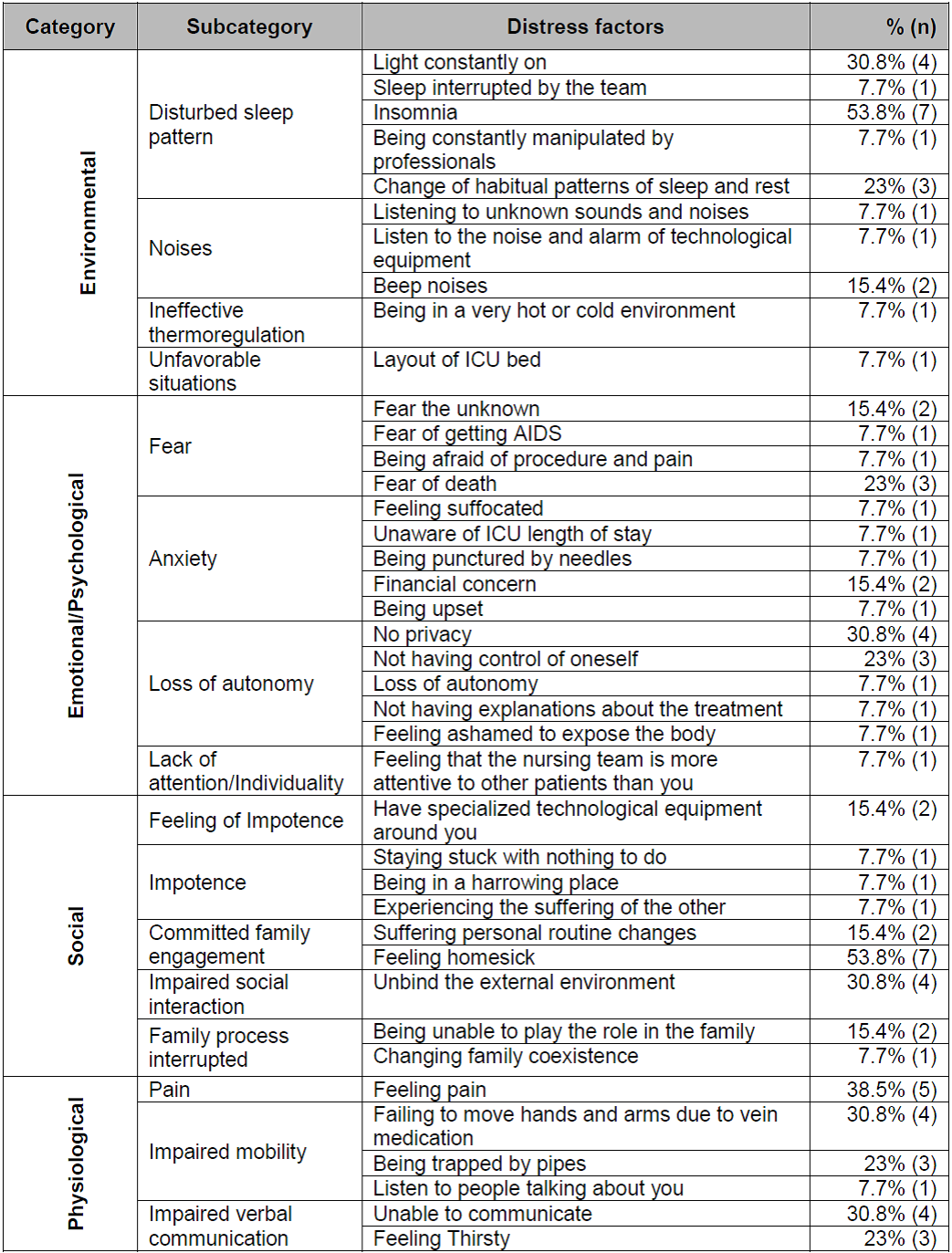
The analyzed articles stood out four considerable categories of distress factors under patients’ perspective, which were: environmental, physiological, emotional/psychological, and social. The categories presented a total of 16 subcategories, and 40 distress factors, as described in the chart 1 .
The method of integrative review enabled the comprehension of the problematic of stressors in adult patients hospitalized in an intensive care unit, and the identification of possible nursing care in the social, psychological, emotional, physiological and environmental scopes.
In the environmental category, the subcategory “disturbed sleep pattern” was influenced not only by the daily routine imposed by the ICU, but also by the characteristic of being a closed and high-complex unit, which brings along new coping situations7 . Therefore, we can infer that the period of hospitalization in the ICU may trigger distinct levels of stressors for the patients.
The environment triggers a higher difficulty to sleep, for patients’ reports focused on the unknown noises of the technological equipment that present different intensities, excessive and constant luminosity, the performance of procedures, staff movements, and the constant manipulation of professional besides the bed12)(13)(14)(15)(16 . The reports still affirm that the noises are accentuated when simultaneously occur the alarms triggered by technological equipment and when it is associated to the noise of the nursing team7 .
As during sleep different physiological and metabolic changes happen, which are connected to organic functions that help patient’s recovery16 , it concerns to the nursing team interventions that propitiate qualified sleep and rest patterns. In other words, nursing must transform the distress factors during nursing care, such as reducing the lights during the night, position the patient on the bed in a comforTable way for the patient, and diminish the noises and the unnecessary movement in the room.
Accordingly to a research developed at a teaching hospital in São Paulo, the disposition of the beds may influence the levels of patients’ distress, for the distance from the nursing station provides more privacy, less luminosity and noises16 . Thus, disposing the lucid and oriented patients in a way that they may feel comforTable in the ICU may help to diminish the intensity and duration of the exposition to the environmental stressor.
In the ICU, generally, the air conditioner temperature is extremely cold or hot. Because patients have some movement limitations due to the situation imposed by the environment they are inserted in, and their health status, they end up becoming more sensitive to the temperature, which makes them consider the environment as way too cold or too hot17 .
In the category “physiology”, patients affirmed that impaired mobility in the bed is a stressor, for they find themselves attached to invasive and non-invasive devices13 . They get this feeling of being stuck3 , besides having an impaired mobility, which triggers the feeling of being impotent8 , once they lose the control about their own situation18 . In order to diminish this feeling on patients and the impaired mobility, it is up to the nurses and other health professionals to periodically evaluate the quantity of devices and technological equipment used, for the long exposure to these stressors provoke discomfort at different levels of intensity and increases the risk for infections19 .
Other physiological factor associated to the already mentioned type regards the intensity and duration of these devices, which are described by patients as acute pain, which alters the respiratory, nervous, sensorial and cardiovascular systems15)(16)(17 . The triggering of the consequences generated by acute or chronic pain may compromise the emotional status of the patient, which induce to anxiety and psychomotor agitation, leading the patient to remove the equipment or devices needed for monitoring, which can cause even more harm to him/herself14 .
Considered the fifth vital sign, pain should not be ignored by the nursing team20 and other health providers, for it is a stressor that reverberates consequences that will compromise the psychological, emotional and physiological aspects of the patient. This, independently of the patient’s status, pain characteristics must be systematically assessed through verbal and numerical scales, or even so by face expressions21 .
Other distress factor that regards the physiological category is impaired verbal communication of patients that present some type of specific commitment or make use of orotraqueal tubes and/or enteral5)(6)(13)(17 . Under the perspective of relatives and professionals, impaired verbal communication is also perceived as a stressor, mainly when it implies the impossibility of making decisions for the patient, transferring such responsibilities to them22 . Therefore, it is up to the professionals to pay attention to signs and symptoms of patients, looking for the identification of methods for non-verbal communication.
As one of the stressors cited by the patient is the difficulty of expressing thirst, one of the nursing care is keeping the patient's lips and mouth moist, using water sprays along with lip moisturizer and frequently reassess the real necessity for the tubes or probes, providing greater well-being, improved bed mobility and, no less, quality of sleep17,23 . Another nursing care linked to communication is the use of notebooks or engravings to enable patients to express themselves in a nonverbal way6 .
Among the social aspects, we highlight the rupture of the patient with his family context and daily life, characterized as an interrupted and committed family coping5)(6)(8)(13)(15)(16)(17)(19)(24 . It is believed that this rupture can be generated by the physiological aspect, which impedes the decision making by the patient, as by the environmental aspect due to the physical space of the ICU.
A quantitative study, developed in two hospitals, one public and one private, located in the interior of the State of São Paulo, identified that the restructuring of the family, when viewed by the patient, is capable of generating psychological distress12 . Other authors affirm that the stressor is associated to the damaged home maintenance, for the most part of the individuals that composed the sample were active employees that provided to their homes and to the other family members12)(17 .
According to reports from lucid and oriented patients, with no communication difficulties, a stressor is the restriction of bedside visits because they cannot have enough time to obtain information from their family members and an understanding of the current routine of the patients without their physical presence17 . Thus, one of the strategies to be used by nurses is to flexibilize and extend the visiting times, since the presence of the relative is able to transmit tranquility and approximation between the family and the patient5)(7)(16)(23 .
Instability in the face of the health and illness process drives the patient to reflect on his/her current and future state of health, as well as on the life context of his family members. Regardless of the nature of these reflections, the patient eventually awakens emotional and psychological factors such as anxiety and fear, characterized as a reaction to a particular perceived threat that is consciously recognized as a danger18) that can still occur. Fear can come from known factors, such as pain and death8 , or unknown, such as noise from technological equipment unknown to patients, which they do not recognize as a priority or even the consequences of their health and disease process7)(8 .
Fear may also be associated to the risk of contracting Acquired Immunodeficiency Syndrome (AIDS), due to the manipulation of other patients in the same hospital environment17 . It is known that current care and the use of disposable devices and devices reduce the spread of AIDS, however, it is incumbent on nursing to guide patients about the safety of the procedures as well as the treatment performed, allowing an accepTable margin of confidence between the patient and health professionals.
The loss of autonomy in the ICU environment, categorized as a stressor of the emotional and psychological category, may be related to the level of dependence24 . It may also be associated to lack of privacy, body control or lack of information about the care to be performed8)(12)(14)(15)(17)(19 . The surveillance and control of the unsTable clinical picture by nursing and the use of technological equipment considered indispensable for the success of the therapy25 can lead to psychological, emotional and biological factors.
Psychological and emotional aspects can be awakened by the lack of recreational activities, which makes the patient more sensitive to his or her suffering and concern for other hospitalized patients5 . In addition, poor recreation activities coupled with disengagement from the outside environment distract the patient from the social environment, increasing the sense of detachment from the family23) and from society. This fact demonstrates that the stressors caused by the ICU environment lead to psychological, emotional and social consequences. Thus, nursing can enable actions of social interaction, such as access to radio or music, preventing the patient from being stressed by having to keep staring at the ceiling26 and experiencing their illness in a negative way.
The reduced quantitative of scientific productions focused on the inpatient perspective showed that some aspects were not highlighted, such as cognitive, spiritual and functional. However, the results suggest that nursing care should be presented in an individual plan that considers the factors that are generating stress in the patient, regardless of the type, duration and intensity of these stressors.
CONSIDERATIONS
In view of the results, it is evident that the stressors identified in this study can be transcribed as nursing care in a plan of individual care to the patient, making possible the recovery and rehabilitation process. Thus, it is up to the nursing to diagnose, intervene and evaluate the patients, preventing and minimizing the stressors during hospitalization in the ICU.
Among the environmental factors, disturbed sleep pattern, noise, ineffective thermoregulation and unfavorable situations were identified. The physiological factors were impaired mobility in bed, impaired verbal communication and pain. The emotional/psychological factors were lack of attention/individuality, anxiety, fear and loss of autonomy. Moreover, the social factors identified were interrupted family process, impaired social interaction, impotence, feelings of impotence and compromised family coping.
It is recommended clinical research to be developed on the subject in the perspective of the patient and new reviews that include new databases and languages. One of the limitations of this study is the variety of instruments used by researchers to identify stressors.
REFERENCIAS
1. Zardini R, Marineia A, De Resende C. valuation of stressor agents and resilience by patients admitted in the intensive care unit. Perspect em Psicol. 2014;18(181):194-213. [ Links ]
2. Rodrigues TDF. Stress factors in intensive care unit nursing. Rev Min Enferm [Internet] . 2012;16(3):454-62. Available from: http://search.ebscohost.com/login.aspx?direct=true&db=c8h&AN=2012011745&site=ehost-live [ Links ]
3. Veiga E, Vianna L, Melo G de. Stress and Technological Innovation in a Cardiac Intensive. Rev Enferm do Centro-Oeste Min [Internet] . 2013;16(3):65-77. Available from: http://www.seer.ufsj.edu.br/index.php/recom/article/view/343 [ Links ]
4. Ullman AJ, Aitken LM, Rattray J, Kenardy J, Brocque R Le, MacGillivray S, et al. Intensive care diaries to promote recovery for patients and families after critical illness: A Cochrane Systematic Review. J Crit Care [Internet] . 2015;52(7):1243-1253. Available from: http://www.journalofnursingstudies.com/article/S0020-7489(15)00100-5/abstract [ Links ]
5. Pina RZ, Lapchinsk LF, Pupulim JSL. Percepção de pacientes sobre o período de internação em unidade de terapia intensiva. Cienc Cuid Saude [Internet] . 2008;7(46):503-8. Available from: http://periodicos.uem.br/ojs/index.php/CiencCuidSaude/article/viewFile/6658/3916 [ Links ]
6. Dornelles C, Oliveira GB De, Schwonke CRGB, Silva R de S. Experiências de doentes críticos com a ventilação mecânica invasiva. Esc Anna Nery [Internet] . 2012;16(4):796-801. Available from: http://www.scielo.br/pdf/ean/v16n4/22.pdf [ Links ]
7. Lemos RCA, Rossi LA. O significado cultural atribuído ao centro de terapia intensiva por clientes e seus familiares: um elo entre a beira do abismo e a liberdade. Rev Latino-am Enferm [Internet] . 2002;10(3):345-57. Available from: http://www.scielo.br/pdf/rlae/v10n3/13344.pdf [ Links ]
8. Proença MDO, Agnolo CMD. Internação em unidade de terapia intensiva: percepção de pacientes. Rev Gaúcha Enferm [Internet] . 2011;32(2):279-86. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1983-14472011000200010&lng=en. http://dx.doi.org/10.1590/S1983-14472011000200010. [ Links ]
9. Bulechek GM, Butcher HK, Dochterman J, Wagner CM. NIC. Classificação das intervenções de enfermagem. 6th ed. Mosby Elsevier, editor. St. Louis; 2016. [ Links ]
10. Cooper HM. The Integrative Research Review: a systematic approach. Sage, editor. Beverly Hills; 1984. [ Links ]
11. Novaes MAFP, Aronovich A, Ferraz M B, Knobel E. Stressors in ICU: patients evaluation. Intensive Care Med [Internet] . 1997;23(12):1282-5. Available from: https://link.springer.com/article/10.1007/s001340050500 [ Links ]
12. Rosa BÂ, Matheus Rodrigues RC, Jayme Gallani MCB, Spana TM, da Silva Pereira CG. Estressores em unidade de terapia intensiva: Versão Brasileira do the Environmental stressor questionnaire. Rev da Esc Enferm. 2010;44(3):627-35. [ Links ]
13. Ayllón Garrido N, Álvarez González M, González García M. Factores ambientales estresantes percibidos por los pacientes de una Unidad de Cuidados Intensivos. Enferm Intensiva [Internet] . 2007;18(4):159-67. Available from: http://www.elsevier.es/es-revista-enfermeria-intensiva-142-resumen-factores-ambientales-estresantes-percibidos-por-13113135 [ Links ]
14. Linch GF da C, Guido L de A, Pitthan L de O, Lopes LFD. Stressors identified for the patient submitted to myocardial revascularization and percutaneous transluminal coronary angioplasty. quantitative study. Online Brazilian J Nurs [Internet] . 2008;7(2):23. Available from: http://search.ebscohost.com/login.aspx?direct=true&db=c8h&AN=2010171328&site=ehost-live [ Links ]
15. Heidemann AM, Cândido PL, Kosour C, Costa AR de O, Dragosavac D. Influência do nível de ruídos na percepção do estresse em pacientes cardíacos. Rev Bras Ter Intensiva [Internet] . 2011;23(1):62-7. Available from: http://dx.doi.org/10.1590/S0103-507X2011000100011. [ Links ]
16. Marosti C, Dantas S. Avaliação dos pacientes sobre os estressores em uma unidade coronariana. Acta Paul Enferm [Internet] . 2005;19(2):190-5. Available from: http://www.scielo.br/pdf/ape/v19n2/a10v19n2.pdf [ Links ]
17. Dias D de S, Resende MV, Diniz G do CLM. Patient stress in intensive care: Comparison between a coronary care unit and a general postoperative unit. Rev Bras Ter Intensiva [Internet] . 2015;27(1):18-25. Available from: http://www.scielo.br/pdf/rbti/v27n1/0103-507X-rbti-27-01-0018.pdf [ Links ]
18. Herdman SK. Diagnósticos de enfermagem da NANDA: definições e classificação 2015-2017. Artmed, editor. Porto Alegre; 2015. 468 p. [ Links ]
19. Bitencourt AGV, Neves FBCS, Dantas MP, Albuquerque LC, Melo RMV De, Almeida ADM, et al. Análise de estressores para o paciente em Unidade de Terapia Intensiva. Rev Bras Ter Intensiva [Internet] . 2007;19(1):53-9. Available from: http://www.scielo.br/pdf/rbti/v19n1/a07v19n1.pdf [ Links ]
20. Queiróz DTG, Carvalho MA de, Carvalho GDA de, Santos SR dos, Moreira A da S, Silveira M de F de A. Dor - 5o sinal vital: conhecimento de enfermeiros. Rev enferm UFPE line [Internet] . 2015;9(4):7186-92. Available from: http://www.revista.ufpe.br/revistaenfermagem/index.php/revista/article/viewFile/7275/pdf_7451 [ Links ]
21. Fortunato JGS, Furtado MS, Hirabae LF de A, Oliveira JA. Escalas de dor no paciente crítico: uma revisão integrativa. Rev Hosp Univ Pedro Ernesto [Internet] . 2013;12(3):110-7. Available from: http://www.e-publicacoes.uerj.br/index.php/revistahupe/article/view/7538 [ Links ]
22. Barth AA, Weigel BD, Dummer CD, Machado KC, Tisott TM. Stressors in the relatives of patients admitted to an intensive care unit. Rev Bras Ter Intensiva [Internet] . 2016;28(3):323-9. Available from: http://www.scielo.br/pdf/rbti/v28n3/en_0103-507X-rbti-28-03-0323.pdf [ Links ]
23. Piccini JD, Dummer CD, Fernandes RD, Arenhardt MP, Maraschim R, Paulo J, et al. Distanciamento dos familiares como principal fator estressor em uma Unidade de Terapia Intensiva. Rev da AMRIGS [Internet] . 2016;60(1):1-5. Available from: http://www.amrigs.org.br/revista/60-01/01.pdf [ Links ]
24. Faquinello P, Dióz M. A UTI na ótica de pacientes. Rev Min Enferm [Internet] . 2007;11(1):41-7. Available from: http://www.reme.org.br/artigo/detalhes/311 [ Links ]
25. Oliveira EB de, Souza NVM de. Stress and Technological Innovation in a Cardiac Intensive. Rev enferm UERJ [Internet] . 2012;20(4):457-62. Available from: http://www.e-publicacoes.uerj.br/index.php/enfermagemuerj/article/view/4768 [ Links ]
26. Prado APO, Bento D, Gardenghi G. Avaliação de possíveis fontes externas de estresse e o seu nível em duas unidades de terapia intensiva em pacientes pós-angioplastia coronariana. Rev Soc Cardiol Estado São Paulo [Internet] . 2012;22(3 Supl A):25-30. Available from: https://www.researchgate.net/publication/283341796 [ Links ]
Received: October 19, 2017; Accepted: December 07, 2017
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
