










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkEnfermería Global
versão On-line ISSN 1695-6141
Enferm. glob. vol.18 no.53 Murcia Jan. 2019 Epub 14-Out-2019
https://dx.doi.org/10.6018/eglobal.18.1.309061
Articles
Perception of the nursing team on climate organizational safety of a public hospital
1Registered Nurse. Master’s Student of the Graduate Program in Nursing, Federal University of Mato Grosso, Cuiabá, Mato Grosso, Brazil.
2PhD in Nursing. Associate Professor of the undergraduate Nursing course of the Federal University of Mato Grosso, Cuiabá, Mato Grosso, Brazil.
3PhD candidate in Collective Health of the Institute of Collective Health.
3Assistant Professor of the undergraduate Nursing course of the Federal University of Mato Grosso, Cuiabá, Mato Grosso, Brazil.
4Registered Nurse. BSc from the Federal University of Mato Grosso, Cuiabá, Mato Grosso, Brazil.
5Registered Nurse. PhD in Sciences. Associate Professor of the Faculty of Nursing of the Federal University of Mato Grosso, Cuiabá, Mato Grosso, Brazil.
Objective:
To evaluate the perception of the nursing team regarding the organizational safety climate in a referral hospital in the metropolitan region of the capital of Mato Grosso, Brazil, and to verify whether there were statistically significant differences in the perception of the organizational safety climate among the nursing assistant, nursing technician and nurse categories.
Method:
A descriptive, transversal study with nursing professionals, using the self-administered Safety Attitudes Questionnaire (SAQ), adapted and validated for Brazil.
Results:
the sample consisted of 139 nursing professionals. The mean of the SAQ domains ranged from 42.07 to 73.13 points, classified as a poor perception. The evaluation of the domains evidenced lower means for working conditions and perception of management of the unit and of the hospital, respectively.
Conclusion:
There was a low perception of the organizational safety climate in the institution, since a satisfactory score was not achieved in any of the domains investigated, with the exception of the job satisfaction domain, although, in a borderline manner. In this way, it was possible to perceive the distancing of the hospital and unit management from activities related to patient safety, which can directly influence adherence to safe behaviors by the professionals of the team and decrease the quality of the care.
Keywords: Patient Safety; Organizational culture; Health Professionals
INTRODUCTION
Since the times of Florence Nightingale, care directed to the health needs of the patient constitutes the fundamental element in the practice of the nurse. Florence1)prioritized, in addition to hygiene, five essential components for the ideal treatment: pure air, pure water, efficient drainage, cleanliness and light. These presuppositions of Nightingalean thinking are essential in the present context, considering the high rate of hospital infections, which are increasingly common, deadly and resistant to antimicrobials. Practices such as Hand Hygiene (HH) and catheter care are significant in the process of patient care and harm prevention. A multicenter study conducted in European ICUs showed that HH reduced the incidence of central venous catheter-associated bloodstream infection from 2.4/1,000 CVC-days to 0.9/1,000 CVC-days (p<0.0001)2. However, even today, this context is characterized by the occurrence of successive injuries resulting from care practice, leading to the emergence of a gap between the care that the patient should receive and that which is performed3.
In Brazil, in 2013, the Ministry of Health (MH) launched the National Patient Safety Program (NPSP) with the aim of improving the quality of the care provided to patients in all health facilities and promoting greater safety for the professionals, patients and services4. Among the actions recommended by the NPSP the implementation of the safety culture is highlighted. This is defined as a set of values, attitudes, skills and behaviors that determine the commitment to health and safety management, replacing fault and punishment with the opportunity to learn from mistakes and improve healthcare3.
There are two instruments that are used to measure the safety climate in health institutions: theCulture of Safety Survey -CSS and theSafety Attitudes Questionnaire - SAQ.Both questionnaires correlate the scores obtained with the results referring to the quality of care provided to the patients. In this context and through the application of these instruments, it was observed that higher perceptions of safety by the multidisciplinary team equated to shorter lengths of stay of the patients in the hospital environment and lower rate of occurrence of Healthcare-Associated Infections (HAIs)5)(6. Considering the relevance of this issue and the efforts that the Ministry of Health has been making to ensure the patient free from risks and harm to health, it is assumed that the organizational safety climate exerts an influence on the quality of the healthcare. Thus, this study considered the following research question: how do nursing professionals perceive the institutional safety climate in a public hospital in the capital of Mato Grosso state, Brazil? Based on this question, the aim of the present study was to evaluate the perception of the nursing team professionals regarding the organizational safety climate and to verify whether there was a statistically significant difference in the perception of the safety climate among the professional categories of nursing assistants, nursing technicians and nurses.
METHOD
This was a descriptive, cross-sectional, correlational and quantitative study. The population consisted of nursing professionals (assistants, technicians and nurses) working in a hospital in the capital of Mato Grosso state, Brazil, in the areas of surgery, infectology, internal medicine, orthopedics, pediatrics, Burn Treatment Center (BTC), isolation, blood bank, pediatric emergency room, suture room, adult emergency room and the adult and pediatric Intensive Care Unit (ICU). According to the human resources data, the study hospital is a referral center for orthopedics in the state of Mato Grosso, as well as for urgent and emergency care, treating spontaneous requirements and patients referred from other cities in the state. It has 271 registered (operational) beds and provides various types of medical specialty care, such as cardiology, infectology, plastic surgery, ophthalmology, hematology, orthopedics and pediatrics, among others.
The eligibility criteria for the study participants were: to have more than six months of professional experience in the institution, not to exclusively perform administrative functions and not to be doing training provided by the organization at the time of data collection. The sample (n) was calculated considering the proportion of 0.50 (p=0.50), since the prevalence of the outcome was unknown, and the following expression was used, as the population size(N) was known7

This corresponds to n = approximate sample size; N = number of units in the population; p = populational proportion of individuals to be estimated; d = limit for the estimation error (sampling error); α = significance level; zα/2= the value in the standard normal curve, obtained from the standardized normal distribution Table, appropriate for the confidence level used. The confidence interval of 95% (zα/2= 1.96), a 50% proportion for unknown prevalence and a sampling error of 5% were adopted. Thus, a sample of 170 professionals was obtained, which were selected randomly, by means of a draw. It should be noted that the sample selection tried to follow the ratio among nurses, nursing technicians and nursing assistants according to the Federal Nursing Council, which showed a quantity of 22,635 nursing professionals in the state of Mato Grosso, representing 27.80% nurses and 72.20% nursing technicians and assistants8.
The Safety Attitudes Questionnaire (SAQ) was used as the data collection instrument, adapted and culturally validated by Carvalho and Cassiani (2012)9for the Brazilian hospital reality. This instrument contains 41 questions, covering the perceptions regarding patient safety. The 41 items of the questionnaire are grouped into six domains:
Teamwork Climate (TWC): items 1 to 6 consider the quality of the relationship and collaboration among the members of a team.
Safety Climate (SC): items 7 to 13 investigate the professionals’ perception regarding the organizational commitment to patient safety.
Job satisfaction (JS): items 15 to 19 evaluate the positive view of the workplace.
Stress recognition (SR): items 20 to 23 refer to the recognition of how much stressor factors can influence the performance of the work.
Perception of Unit Management (PUM) and Perception of Hospital Management (PHM): items 24 to 29 correspond to the perception of the nursing team regarding the actions developed by the unit management, represented by the direct leadership of the sector, and the actions of the hospital management, developed by the professionals of the head of the hospital (director, superintendent, auditor, etc.).
Working Conditions (WC): items 30 to 33 correspond to the perception of the quality of the work environment. However, items 14, 34 to 36 are not part of any domain in the original instrument because no theoretical affinity was found10.
The SAQ is a self-administered questionnaire, with Likert-type response options on a five-point scale: option A- disagree strongly (0 points), B- disagree partially (25 points), C- neutral (50 points), D- agree partially (75 points) E- agree strongly (100 points) and X- does not apply (0 points). The final score of the instrument varies from 0 to 100 points, in which zero refers to the worst perception of safety attitudes by health professionals and 100, to the best perception. The instrument’s cutoff point for a favorable perception of the safety climate is 75 points, that is, positive values are considered when the total score is equal to or greater than 75 points.
For the data collection, the questionnaires were distributed in opaque and non-identifiable envelopes in the previously mentioned sectors. A pilot study was conducted with nursing professionals, including: 5 nursing assistants, 10 nursing technicians and 5 nurses, who fulfilled the inclusion criteria, in order to test the applicability of the instrument, with no doubts or problems related to the responses to the items of the instrument being identified. The average time of completion was 10 minutes and the professionals were included in the final sample.
The quantitative variables were analyzed through descriptive statistics, with the calculation of the mean and standard deviation. The data were entered into a spreadsheet (Microsoft® Excel Program), validated through double data entry, and exported to the Statistical Package for the Social Sciences (SPSS), version 19.0, program for processing and analysis. For the analysis of the scores among the different professional nursing categories, the Shapiro-Wilk test was used to verify normality, with Student’s t-test used if present and the Mann-Whitney test used if absent, considering a significance level of 0.05.
The study project was submitted to the Research Ethics Committee of the Federal University of Mato Grosso and was approved under authorization No. 1.653.171.
RESULTS
Of the 170 instruments delivered, there was a return of 139 (81.07%) duly completed questionnaires. Regarding the characterization of the sample, 125 of the 139 professionals (89.90%) were female. The mean age was 42.59 years (SD=9.42), with a minimum age of 26 and a maximum age of 68 years. Regarding the professional category, 96 participants (69.10%) were nursing technicians, 29 (20.90%) nurses and 14 (10.10%) nursing assistants. The participants’ time of working in the hospital ranged from 1 to 2 years, with 29 participants (21.60%), and ≥10 years, with 24 participants (17.90%).
Table 1presents the general mean of each domain of the evaluation of the institutional safety culture and the mean of each domain by professional category and work sector.
Table 1- General score of the nursing professionals by domain according to the professional category and work sector variables. Cuiabá - MT, Brazil, 2016.

*The scores for this domain correspond to a samplen=59.
According toTable 1, the domain that presented the highest score was “Job Satisfaction”, with the nursing assistants obtaining a mean of 82 points, followed by the nurses, with 80 points. The worst results were achieved in the analyses of the “Perceptions of the Unit and Hospital Management”, “Safety Climate” and “Working Conditions” domains. The fact should be highlighted that the “Perception of the Unit and Hospital Management” domain scored 47 and 42, respectively, in the overall score. It should also be highlighted that the analysis of the safety climate in the pediatric unit, ICU and clinical unit showed that the perception of the professionals was suboptimal for all domains investigated, with the exception of the “Job Satisfaction” domain in the pediatric unit, with a mean of 83 points, and in the ICU, with a mean of 79 points.
Table 2presents the frequency of the professionals’ responses to each item of the SAQ instrument referring to the Teamwork Climate (items 1 to 6) and Safety Climate (items 7 to 13) domains.
Table 2- Distribution of the nursing professionals’ responses by item of the Teamwork Climate and Safety Climate domains. Cuiabá - MT, Brazil, 2016.
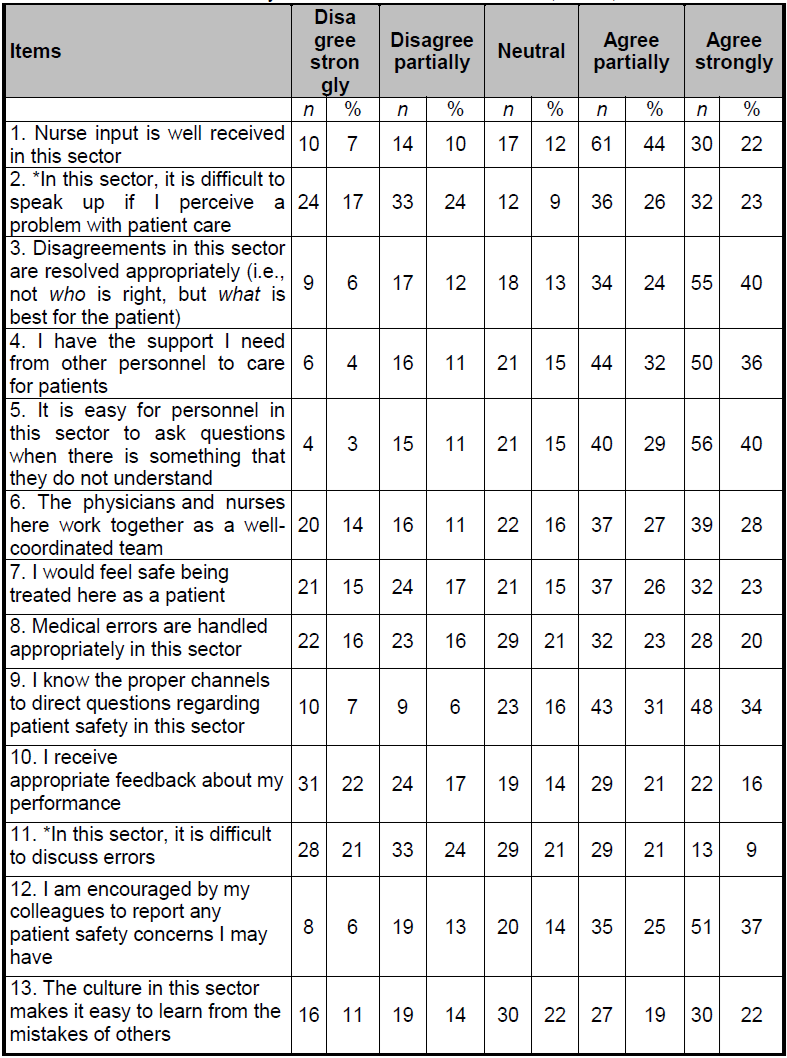
*reversed items.
It was verified that of the 139 professionals, 30 (21.6%) strongly agreed that the nurses’ input was well received and 32 (23.0%) responded that it was difficult to speak up when they perceived a problem with patient care.
Table 3corresponds to the frequency of the professionals’ responses for each item in the Job Satisfaction (items 15 to 19), Stress Recognition (items 20 to 23) and Working Conditions (items 30 to 33) domains. Item 14 does not belong to any domain.
Table 3- Distribution of the nursing professionals’ responses by item of the Job Satisfaction, Stress Recognition and Working Conditions domains. Cuiabá - MT, Brazil, 2016.

*reversed items.
A total of 89 participants (64.0%) said they liked their work and 77 professionals (55.0%) said they were proud of where they worked. Regarding the workload, 70 participants (50.0%) stated that when it is excessive their performance is impaired.
Table 4presents the frequency of responses regarding the perception of the nursing team regarding the management of the unit and the management of the hospital.
Table 4- Distribution of the nursing professionals’ responses by item of the perception of the unit management and hospital management. Cuiabá - MT, Brazil, 2016.

It should be highlighted that the domain of the SAQ regarding the perception of the nursing team about the unit management and the hospital management (items 24 to 29) was analyzed withn= 59 participants (34.7%), due to the losses from incomplete information related to this domain. The researchers believe that this fact occurred because this is the only domain that the participants have to respond to their perception and to indicate it in two moments, that is, to answer about the perception of the Unit Management and about the Institution Management, which is not visually favorable to the participant - a fact related to the face validity of the instrument. The same occurred and was described in the validation study of this instrument10.
Table 5shows the perception of the organizational safety climate by the nursing professional categories.
Table 5- Frequency and overall score by Teamwork Climate, Safety Climate, Job Satisfaction, Stress Recognition, Working Conditions, Perception of Unit Management and Perception of Hospital Management domains, according to the professional category. Cuiabá - MT, Brazil, 2016.

*Student’s t-test (mean scores); † Mann-Whitney test (median scores).
Statistical significance was observed in the comparison between the scores of the nursing technicians and the nursing assistants for the “Perception of the nursing team about the hospital management” domain, showing that the technicians had a lower perception of 33 points when compared to the 60 points of the nursing assistants (p=0.05). Furthermore, for all the domains, except Working conditions, the technicians showed a lower evaluation of perception when compared to the nursing assistants. The same was observed between the nurses and nursing assistants.
DISCUSSION
In the present study, it was observed that the perception of the safety climate varied according to each domain and professional category and, in general, satisfactory results were not obtained. The Safety Climate domain obtained an overall mean of 57 points and presented fragility in all the items evaluated, which demonstrates the concern of the professionals with the quality and safety of the patient. A study carried out in Brazil, in three health facilities in the state of Ceará, represented by a mental health referral hospital, an infectious disease referral hospital and a general hospital, obtained means for this domain of 65; 67 and 63 points, respectively11.
It should be noted that, scores below 60 points indicate an alert situation for organizations, demonstrating an urgent need for the institution to carry out actions that promote the safety climate of the patients and professionals9. This was the situation found in the present study, which showed a worrying perception of the organization’s safety climate. The analysis of this domain in the present study evidenced that the participants demonstrated difficulty in discussing, communicating and managing errors, as well as a lack of adequate feedback regarding their professional performance. In addition, few agreed that safety suggestions would be put into action by the hospital management. Therefore, in order for patient safety to be a reality, the safety culture must be structured in the institutions, which corresponds to establishing a safe environment in which the professional feels confident, motivated and committed to the learning and continuous improvement of the healthcare4. Corroborating these findings, the National Quality Forum (NQF) states that promoting a culture of safety in all healthcare settings involves awakening a collective consciousness related to values, attitudes, competencies and behaviors that determine the commitment to health and safety management. In addition, this means seeing safety incidents not as problems, but as opportunities to improve the care, avoiding blaming employees that commit unintentional errors12.
Although affected by the sample size, the lowest scores (47 and 42, respectively) were observed in the domain “Perception of Unit Management” and “Perception of Hospital Management”, which demonstrated the negative view of the study professionals regarding the positioning of the management considering the safety of the patients and professionals. Other Brazilian studies have also identified that participants do not feel safe or supported by the hospital administration, indicating the distance between the nursing team and the administrative staff in matters that refer to patient safety and requirements linked to the care13)(14. In this context, the importance of the implementation of a culture that assures the responsibility between the managers of the organization and managers of the unit is emphasized. With this, the professionals who act directly in the patient care feel safe and motivated in their work environment. Institutions that adopt this culture proactivity stimulate the work dynamics of the team, enabling them to manage the risks existing in the workplace through continuous monitoring, and facilitating the participation of these professionals in decision-making and improvement of the processes15)(16.
The “Stress Recognition” (SR) domain was also viewed by more than half of the participants as a negative construct in the work. It was noticed that, although stress is a variable attributed to the individual, it is also consolidated due to the management model and the way of organizing the work, which demonstrates the multifaceted analysis of the safety climate perception and the interrelationship and dependence among the constructs investigated. A study carried out in Ethiopia showed that one of the conditions that accentuated stress in the health providers was the insufficient number of workers during the shift17. Other sources of work stress have also been identified, such as an inadequate salary, lack of management support and absence of a career plan, which may result in higher rates of absenteeism and staff turnover18.
The results of the “Teamwork Climate” domain presented an overall mean of 66.02 points, which shows that there was not a good relationship among the professionals. Thus, it is believed that in order to reach satisfactory levels in staff relationships, it is necessary for the institution to promote motivational activities and to broaden the partnership relations among the professionals, thus establishing the involvement of all in the activities of the organization. In this context, some authors mention that when professionals of the health team work in a cohesive way, motivated by the continuous improvement of the care processes, patients feel safer and receive better quality care19.
In the evaluation of the “Working Conditions” domain, the participants of the present study highlighted poor communication and a lack of adequate monitoring when they were admitted to the institution. Some authors emphasize that when the professionals do not have access to the necessary patient information, equipment, logistical support and adequate supervision, they end up having their care practice impaired, which results in a loss of autonomy and an increased risk of adverse events20. Corroborating these findings, an integrative literature review showed that a lack or low investment in working conditions may expose professionals and patients to risks and generate dissatisfaction and demotivation in the work environment. These factors constitute important reasons for low or non-adherence to standard precautions with consequent harm to both the patient and the professional21. Thus, it is necessary to develop educational actions aimed at personal and professional training, including themes related to motivation and teamwork, among others. In addition, organizations should advocate shared management, teamwork and integral care, as well as valuing the needs of professionals and patients, comprehending the human element as the focus of the health actions22.
The analysis of the comparison of the perception of the safety climate among the professional categories showed that the nursing technicians had a lower perception for the “perception of the hospital management” domain when compared to the nursing assistants, which was statistically significant (33 and 60,p=0.05). It should be noted that, for all domains, except “Working conditions”, the nursing assistants showed a more positive perception of the safety climate when compared to the nursing technicians and nurses. It was noticed that the higher level professionals had a clearer view of the problems and vulnerabilities found in the work environment and the consequent risks to patient safety, therefore, their scores were lower in each domain. In this context, the fundamental level professionals presented higher scores, which shows that the perception of the safety climate was more positive and consequently, that they may not comprehend the existing problems. A recent study carried out in three public hospitals in the Northeastern region obtained a similar result, in which the higher level professionals had a better perception of stressors when compared to the mid-level professionals11. From this perspective, it is necessary to invest in training and education with continuous education in health as the reference, considering that it is a qualification strategy that incorporates learning into the daily life of organizations and provides spaces of exchange among professionals, which contributes to the qualification of the work and, consequently, of the care22. Thus, the development of continuous education is the task of nurses and must be implemented in order to improve the quality of the care provided to the client and, consequently, the institutional safety climate23.
The present study presented limitations. It was performed in only one hospital, thus limiting the generalization of the results found and hindering the representativeness of the nursing professionals. The sample size was also a limiting factor, as was the fact that the participants were reluctant to complete the items in the “Perception of the Unit and Hospital management” domain, even though their anonymity was guaranteed. Another important factor to consider is that although the respondents answered self-administered questionnaires based on their actual performance, overestimation exists as a questionable factor.
CONCLUSION
The results of this study allowed the conclusion that there was a low perception of safety in the institution, since a satisfactory score was not reached in any of the domains of the instrument used, with the exception of job satisfaction, however, in a borderline way. The hospital administration and the unit management were seen to be distant from activities related to patient safety, since the results show difficulties in communication and teamwork with perception of precarious working conditions and high stress. In the analysis of the perception of the professionals regarding the safety climate, it was verified that the nursing technicians had a lower perception regarding the “Perception of the hospital management” domain when compared to the nursing assistants, which was statistically significant. Furthermore, it was noticed that the higher level professionals more clearly perceived the problems and vulnerabilities found in the work environment and the consequent risks to the safety of the patient. In this context, the fundamental level professionals - nursing assistants, presented higher scores, which shows that their perception of the safety climate was more positive and, consequently, they may have had difficulty comprehending the existing problems.
It is concluded that the study and discussion of the domains involved in the organizational safety climate, through the application of the Safety Attitudes Questionnaire, allowed the reality of the hospital institution to be evaluated with reliability, since it is a validated and reliable instrument. This should enable and encourage the realization of new studies in the different scenarios of the Brazilian and international culture.
REFERENCIAS
1. Lee G, Clark AM, Thompson DR. Florence Nightingale - never more relevant than today. J Adv Nurs. 2013; 69(2): 245-6. [ Links ]
2. Van der Kooi T, Sax H, Pittet D, Van Dissel J, Van Benthem B, Walder B, et al. Prevention of hospital infections by intervention and training (PROHIBIT): results of a pan-European cluster-randomized multicentre study to reduce central venous catheter-related bloodstream infections. Intensive Care Med. 2018; 44(1). [ Links ]
3. Brasil. Ministério da Saúde. Documento de referência para o Programa Nacional de Segurança do Paciente - Brasília : Ministério da Saúde, 2014. [ Links ]
4. Ministério da Saúde (BR). Portaria n 529, de 1 de Abril 2013. Institui o Programa Nacional de Segurança do Paciente (PNSP). Brasília; 2013. [ Links ]
5. Sexton JB, Helmreich RL, Neilands TB, Rowan K, Vella K, Boyden J, et al. The Safety Attitudes Questionnaire: psychometric properties, benchmarking data, and emerging research. BMC Health Serv Res. 2006; 6(44). [ Links ]
6. Colla JB, Bracken AC, Kinney LM, Weeks WB. Measuring patient safety climate: a review of surveys. Qual Saf Health Care. 2005; 14(5). [ Links ]
7. Bolfarine H, Bussab WO. Elementos de amostragem. 1 ed. São Paulo: Editora Edgar Blücher LTDA; 2005. [ Links ]
8. Conselho Federal de Enfermagem (COFEN). Cofen lança perfil da Enfermagem no Mato Grosso. Mato Grosso (MT). 2015. [ Links ]
9. Carvalho REFL, Cassiani SHB. Cross-cultural adaptation of the Safety Attitudes Questionnaire - Short Form 2006 for Brazil. Rev Latino-Am. Enfermagem. 2012; 20(3): 575-82. [ Links ]
10. Rigobello MCG, Carvalho REFL, Cassiani SHB, Galon T, Capucho HC, Deus NN. The climate of patient safety: perception of nursing professionals. Acta Paul Enferm. 2012; 25(5). [ Links ]
11. Carvalho REFL, Arruda LP, Nascimento NKP, Sampaio RL, Cavalcante MLSN, Costa ACP. Assessment of the culture of safety in public hospitals in Brazil. Rev Latino-Am Enfermagem. 2017;25:e2849. [ Links ]
12. The National Quality Forum. Safe Practices for Better Healthcare 2010 update. Washington: The National Quality Forum: 2010. [ Links ]
13. Rigobello MCG et al. The perception of the patient safety climate by professionals of the emergency department. Int Emerg Nurs. 2017; 33:1-6. [ Links ]
14. Marinho MM, Radunz V, Barbosa FFS. Assessment of safety culture by surgical unit nursing teams. Texto & Contexto Enferm. 2014; 23(3): 581-90. [ Links ]
15. Boysen PG. Just culture: a foundation for balanced accountability and patient safety. Ochsner J. 2013; 13: 400-6. [ Links ]
16. Rocha FLR, Marziale MHP, Carvalho MC, Id SFC, Campos MCT. The organizational culture of a Brazilian public hospital. Rev Esc Enferm USP. 2014; 48(2): 308-14. [ Links ]
17. Dagget T, Molla A, Belachew T. Job related stress among nurses working in Jimma Zone public hospitals, South West Ethiopia: a cross sectional study. BMC Nurs. 2016; 39(15): 2-10. [ Links ]
18. Mosadeghrad AM. Occupational stress and turnover intention: implications for nursing management. Int J Health Polic Manag. 2013;1(2):169-76. [ Links ]
19. Weaver SJ, Sydney MD, Rosen MA. Team-training in healthcare: a narrative synthesis of the literature. BMJ Qual Saf. 2014; 23(5): 359-72. [ Links ]
20. Fermo VC, Radünz V, Rosa LMR, Marinho MM. Professional attitudes toward patient safety culture in a bone marrow transplant unit. Rev Gaúcha Enferm. 2016; 37(1): 1-9. [ Links ]
21. Porto JS, Marziale MHP. Motivos e consequências da baixa adesão às precauções padrão pela equipe de enfermagem. Rev Gaúcha Enferm. 2016; 37(2): 1-16. [ Links ]
22. Silva KL, Matos JAV, França BD. A construção da educação permanente no processo de trabalho em saúde no estado de Minas Gerais, Brasil. Esc Anna Nery. 2017; 21(4). [ Links ]
23. Miccas FL, Batista SHSS. Permanent education in health: a review. Rev Saúde Pública.2014; 48(1):170-185. [ Links ]
Received: November 03, 2017; Accepted: March 02, 2018
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
