










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.18 n.53 Murcia Jan. 2019 Epub Oct 14, 2019
https://dx.doi.org/10.6018/eglobal.18.1.303051
Articles
Comparative study analysing maternal recovery after childbirth according to Marjory Gordon’s Patterns
1University Nursing School of Cartagena, attached to the University of Murcia. Murcia. Spain.
2University Hospital of Torrevieja. Alicante.
2Faculty of Nursing, University of Murcia. Spain.
Objective:
Analyse if there is any difference in recovery rate according to their puerperium stage depending on perineal lesion.
Material and method:
Prospective longitudinal descriptive quantitative study, following the Marjory Gordon’s Functional Health Patterns. Data collection will be performed in three phases (immediate, clinical and remote puerperium), through semi-structured interview completed in first instance in a face-to-face interview and phone call interview at 10 and 30 days, respectively.
Results:
In Spain there is an episiotomy, induction and assisted delivery rate much higher than recommended. Episiotomy technique lead to significant tear (16,7%) in this study. During immediate puerperium, women who were practiced an episiotomy shown mobility difficulties (p=0,0005), elimination (p=0,0007), baby care (p=0,015), rest (p=0,15) and perceived pain (p=0,005), whereas in the clinical puerperium are affected only mobility (p=0,05), elimination (p=0,042) and perceived pain (p=0,006). After 30 days, remote puerperium, there is not statistical significant differences in both groups. More research is needed to confirm these facts as well as provide new knowledge.
Conclusions:
Episiotomy produce more negative effects than spontaneous tears at the immediate and clinical puerperium of women. Pain produced by this technique as a short, medium and long term limit many daily activities of women.
Keywords: episiotomy; tear; puerperium; pain; recovery
INTRODUCTION
Puerperium is the period of time from the end of birth to the complete anatomical and physiological recovery (especially hormonal and that of the reproductive system) of mothers. Their body must return to the pregestational conditions1. It is divided into three successive stages, namely: hospital or immediate puerperium, clinical or mediate puerperium and late or distant puerperium2.
Despite being a period without apparent complications, the development of technology and the medicalization of a process that should be as natural as possible have led to the use of excessive interventionism. For that reason, it can sometimes imply more complications than benefits. World Health Organization (WHO) reported on the damages caused by some of these interventions based on scientific evidence. In despite of health risks to women, such practices continue to be routinely carried out in many hospitals in Spain3, as the case of routine use of episiotomy4. Such a use was justified in preventing the appearance of perineal tears, pelvic floor problems, a potential urinary and faecal incontinence, and by saying that it provided benefits to the foetus by shortening the expulsive period and facilitating spontaneous delivery. However, scientific evidence has confirmed its adverse effects: major tears, anal sphincter dysfunction and pain in sexual relationships (dyspareunia)5. Recently, a research has been published stating that most severe perineal tears (III and IV degree) in the second birth were associated with the use of episiotomy in first delivery, with 4.8%, compared to 1.7% when it was not performed (p <0.001)6.
The rates of episiotomies in Europe are above from WHO recommendations (20%) in most of the countries of the European Union. Spain is around 43%, being the eighth country with the highest rates of the 29 that are compared in it. Following the recommendations of WHO, the Spanish Ministry of Health and Social Policy recommended the restrictive use of episiotomy3)(7)(8)(9)(10.
There is great variability in the rates of episiotomies among the Spanish Autonomous Communities8. In 2009, 33% of episiotomies were performed in our region on total deliveries, the lowest number of these interventions. The data, provided by Santa Lucía Hospital in Cartagena, indicates that the number of episiotomies between 2011 and 2014 has been gradually decreasing from 37.3% to 31.6%11.
There is a high level of interventionism in birth attendances in Spain in comparison with its European neighbours, because although the country did not exceed them in caesarean sections, the rates of instrumental deliveries, episiotomies and incitements are higher. On the other hand, better results in terms of perinatal or neonatal mortality were obtained8)(12.
Theobjectiveof this study is to analyse whether there are differences in the level of recovery in the different phases of the puerperium depending on the type of perineal lesion.
Thehypothesisproposed was that women in labour who have had an episiotomy have a greater number of Functional Health Patterns by Marjory Gordon altered, in each one of the puerperium stages, in relation to those who have suffered a natural tear of the perineum.
Themain objectivewas to analyse if there are differences in the level of recovery in the different phases of the puerperium depending on the type of perineal injury. Thespecific objectiveswere to describe the sociodemographic characteristics and birth data of the women participating in the study, to assess the status of the woman in the different phases of the puerperium according to the eleven Functional Patterns by Marjory Gordon, as well as to analyse if there is a relationship between the perineal lesion and the assessment according to the Functional Patterns by M. Gordon in the different puerperium phases.
MATERIAL AND METHOD
Population and sample
Women who had a vaginal delivery at the Santa Lucía General University Hospital in Cartagena during the study period. Women who had a vaginal delivery (normal or instrumental) and a lesion in the perineum (tear or episiotomy) participated in the research.
It was a convenience sample. A total of 36 women participated in the study, 18 of whom had different grades of tears while the other 18 episiotomies. There have been two losses, one in each group (5.56%).
The study was carried out during women's hospital stays.
inclusion criteria
- Women who had vaginal, normal or instrumental deliveries and a lesion in the perineum (tear or episiotomy) attended in the Obstetrics Service (Unit 33) at the Santa Lucía General University Hospital from Area II in the Region of Murcia.
- Women over 18 years old.
- Women who understood Spanish language.
- Women who agreed to sign the Informed Consent of the study.
Variables
The variables were divided into three major groups: sociodemographic characteristics, birth data and assessment based on the Functional Health Patterns by Marjory Gordon.
Instruments and data collection
The format of data collection was a semi-structured interview whose questions were completed with oral information from mothers. The same interview was conducted at two different moments. In this way, we were able to assess women's evolution in the postnatal period, depending on the perineal lesion. The initial interview was personal and was carried out at the maternity unit during the immediate puerperium (first 48 hours), and the second and third telephone interviews 10 and 30 postpartum days, respectively.
The validation of the employed questionnaire was not necessary, since the questions in it were extracted from the evaluation by original patterns, which was enough in the computerised histories to value our patients.
The recruitment of women was done at the same Obstetrics Service, through the visualisation of the Clinical Histories, to know the type of delivery they had had. Data were collected from clinical histories and partograms, both on paper and computerised, available on SELENE®computer program.
Limitations
The small size of the convenience sample chosen (n = 36) due to the limited time we had for the data collection, and not a random sample as it is considered to be ideal. This fact undoubtedly supposes a selection bias that could only be avoided with randomisation method. In addition, the questionnaire has not been passed in a multicentre manner, at the other hospitals, as it would be desirable.
However, we do not consider that this fact could affect too much the statistical values we obtained, but they would probably be very similar to the current ones. Yes it would be favourable to get additional information instead the one shown here.
Statistical analysis
The statistical analysis was carried out with the IBM®SPSS®Statistics version 23.0.0.0 program. Firstly, descriptive statistics of each of the variables were obtained, obtaining frequency distributions. The dependency or association among qualitative variables was approached with an analysis of contingency Tables with the Pearson Chi-square test supplemented with residue analysis to see the degree of dependence.
RESULTS
Sociodemographic data
Sociodemographic characteristics of the sample are shown inTable I, indicating the frequencies and percentages of the values for each of the variables. The mothers' age has been grouped in intervals for a better understanding. We can see that more than one third of the respondents have university studies (36.1%).

Delivery data
The birth data are reflected inTable IIbelow, showing the incidence of each variable. The duration of the delivery is grouped in hourly intervals for an easier understanding. It is interesting to note that 50% of births began with stimulation or induction. 50% of deliveries also had a duration of no more than five hours.

Condition of perineum
Figure 1shows the different types of perineal lesion which were found during the study. We highlight the fact that, despite the episiotomies, there are also tears in this group, with a 16.7% in the percentage of women suffering both injuries in their deliveries, a figure definitely not negligible.

Analysis of the relationship between the postpartum assessment, according to the functional health patterns by Marjory Gordon, and the type of perineal injury.
Immediate puerperium
Table IIIshows the value of the Pearson Chi-square of the Functional Patterns by Marjory Gordon. It is noted that practically all alterations occur in the group of episiotomies. And then, those patterns in which there were statistically significant differences between both studies were discussed.
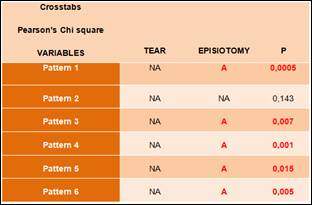
Pattern 1. Perception - Health Management
In the immediate puerperium it was observed that women who had suffered a tear did not have difficulties to perform daily activities, however, women who had had an episiotomy did have difficulties in the first 24-48 hours (p = 0.0005; expected count = 10.0 and corrected residue = 4.0) . In fact, after asking the question in which areas they had difficulty (sitting, getting up, walking, sleeping, stooping, feeding the baby, etc.) to answer yes or no, women with tear showed no problems (p = 0.042; expected count = 8.0 and corrected residue = 4.0).
Pattern 3. Elimination
In the immediate puerperium it was observed that women with episiotomy had to resort to the use of laxatives, unlike women with perineal tear, who had not needed them (p = 0.007; expected count = 15.0 and corrected residue = 2.7). By performing a unilateral p test, it can be confirmed that women with episiotomy suffered ache or difficulties when urinating, while women with tear did not so (p = 0.047; expected count = 8.5 and corrected residue = 1.7).
Pattern 4. Activity - Exercise
During the hospital puerperium, those women who had a tear did not have usually needed any help for the care of their baby, however, those with episiotomy had to resort to other people to do so (p = 0.015; expected count = 11.5 and corrected residue = 2.4). The independence for mobility, personal hygiene, use of toilet and dress is also clearly different in both groups, since it is observed that women with tear are totally independent in these activities 24-48 hours after giving birth (p = 0.001; expected count = 6.5 and corrected residue = 3.1).
Pattern 5. Dream - Rest
In the first stage of the puerperium we found that women with tear did not have rest periods throughout the day, while those with episiotomy as an intrapartum wound did (p = 0.015; expected count = 11.5 and corrected residue = 2.4).
Pattern 6. Cognitive - Perceptual
In the initial stage of the puerperium we see how women who have undergone an episiotomy have a severe level of pain, that is, evaluated with 6-7 points in the Visual Analog Scale EVA (p = 0.005; expected count = 5.0 and corrected residue = 3.0).
Clinical puerperium
Table IVshows the value of the Pearson Chi-square of the Functional Patterns by Marjory Gordon in relation to the second interview that was performed to women in labour in the clinical puerperium. Those patterns that are altered appear in bold and red. At this time of recovery, there are fewer alterations, being them in patterns 1, 3 and 6. And now, we comment on those patterns in which there are statistically significant differences between both study groups.

Pattern 1. Perception - Health Management
In the clinical puerperium, it was observed that women who presented perineal tear after delivery did not present difficulties to carry out daily activities, and when asked in which area they present difficulties the answer was none (p = 0.05; expected count = 12.5 and corrected residue = 2.1), while it is observed a tendency for those who presented episiotomies to have difficulty in mobility in general.
Pattern 2. Nutritional - Metabolic
In the clinical puerperium, women with tear did not suffer ache in the perineal area (p = 0.042; expected count =7.0 and corrected residue = 2.1), and they did not have problems when they feed their babies (p = 0.007; expected count = 14.0 and corrected residue = 2.7).
Pattern 3. Elimination
In the clinical puerperium we found that women with tear had a bowel movement (p <0.05; expected count = 9.5 and corrected residue = 2.4) and did not need to use laxatives (p = 0.015; expected count = 14.5 and corrected residue = 2.4). They did not present discomfort or pain during the process, but it did happen to those with episiotomy (p = 0.042; expected count = 6.0 and corrected residue = 2.2). Regarding the difficulty or discomfort to urinate, it was observed that women who presented episiotomies had difficulty, while none of the women with tear presented it (p = 0.024; expected count = 12.2 and corrected residue = 2.3).
Pattern 6. Cognitive - Perceptual
10 days after delivery, women who had a tear did not have pain in the area (p = 0.05; expected count = 9.0 and corrected residue = 2.7). They did not take analgesics, however women with episiotomy had the need of them (p = 0.006; expected count = 8.0 and corrected residue = 2.7), being the ibuprofen the most frequent (p = 0.011; expected count = 5.0 and corrected residue = 3.0).
DISCUSSION
This is an important study, because it is the first study which assessed postpartum women from a global nurse perspective based on the Functional Health Patterns by Marjory Gordon.
Regarding birth data, it was observed the fact that 30.6% were instrumental vaginal deliveries in the present study, being 15% the average in our country. This data reinforces the fact that there is great variability among different Autonomous Communities13.
The induction of childbirth is another of the practices on which both the WHO and the Spanish Ministry of Health and Social Policy warn, recommending not to exceed a rate of 10%9and, nevertheless, our data indicate that only 50 % of vaginal deliveries began spontaneously, with 11.1% stimulated and 38.9% induced8.
On the other hand, inFigure 1it was observed that episiotomies generate important tears to a 16.7% of women presenting both injuries8. Other studies describe that the most severe perineal tears, of III and IV degree, occurred due to the use of episiotomy10.
During the hospital puerperium, inPattern 1 Perception - Health Managementwe found that women with tears did not have difficulties in their daily activities but so did those with episiotomy (we refer to their mobility to walk, sit, get up and even feed their babies). The information provided by other studies confirmed that this practice generates pain during the first 24-48 hours and affects mobility, reducing it14. Women who did not have episiotomy showed better general well-being, the pain when walking is virtually non-existent and they felt more comforTable15.
In a study conducted among women with episiotomy in 2012 in Granada16it was found that the majority of participants reported some restriction of activities between 20 and 48 hours postpartum. When women were asked about the limitation of activities due to perineal pain, most of them frequently mentioned sitting, walking and sleeping.
Our results indicate that in the clinical puerperium women with tear had no problems in their daily activities and those with episiotomy had a tendency to difficulty in general mobility. No studies have been found that address this aspect 10 days after delivery.
As for thePattern 2 Metabolic Nutritional, in the clinical puerperium we verified that the women with tear did not present ache in the area of the perineum or problems to feed their children. However, other studies indicate that the alteration of Pattern 1 may affect this, due to an exacerbation of pain while walking, changing position and sitting, making breastfeeding difficult14)(15.
In the immediate and clinical puerperium, thePattern 3 Eliminationshows that women with episiotomy had constipation, which led them to the need of laxatives, in contrast to those with tear and who had a bowel movement daily and without problems or ache. A study conducted in 200417compared pain in a group of women with restrictive episiotomy and another with routine episiotomy, in four areas, one of them being defecation, concluding that in the first group there was less perineal pain, with a statistically significant p of 0.005 to 0.048. This pain was what causes them to have a difficulty in defecation, having to resort to the use of laxatives.
On the other hand, we found a systematic review published in 200518in which eight cohort studies were included and analysed, among others. In four of them, women were asked about rectal incontinence and none found that the episiotomy was associated with a statistically significant reduction of difficulty in retaining gas or faeces. However, by unifying data from two of the studies with comparable outcome measures, an increased risk associated with the use of episiotomy was observed. And in another study it was found that faecal incontinence is more likely when there is episiotomy, instrumental deliveries or anal sphincter injury.
Following recommendations from the Clinical Practice Guideline for Pregnancy and Puerperium Care19, it is advised that women with constipation during the puerperium reinforce the intake of natural and liquid fibres in their diet, and the administration of a laxative stimulant of the intestinal or osmotic motility in those in which it persists20.
In the present study, there was considerable difficulty or ache when urinating in the group of women with episiotomies. In contrast, this aspect was not affected in postpartum women with another type of perineal injury. This fact is influenced again by the level of pain, which also affects the basic needs of food and excretion, as well as taking care of the newborn and feeding them21.
This technique was a risk factor for urinary incontinence, along with the use of forceps or a prolonged expulsive, but did not influence the different types of urinary incontinence22. Other studies determine that the pain that it generates can affect the defecation, causing constipation and urination causing difficulty for it14)(15.
RegardingPattern 4 Activity - Exercise, we see that in the hospital puerperium the group of women with tears could care for their baby without needing the help from the others, unlike the group of episiotomies. The independence for mobility, personal hygiene, use of the toilet and dress is also absolute in the first group. In a study prepared in 2012 on the measurement and characteristics of pain after episiotomy and its relation with the limitation of activities, one of the obtained results was that more than a half of the participants complained of pain at rest, as indeed we also find ourselves. This fact reinforces the idea that pain can limit mothers in various functions. The presence of pain during movement in all of them in the initial puerperium can also limit some daily activities, which means that they have to resort to the help of other people, as we have seen in this pattern23.
24-48 hours after delivery, we discovered inPattern 5 Sleep - Restthat women with a tear did not have rest periods throughout the day, while those with episiotomy as an intrapartum wound did. It is likely that this fact is influenced by the presence of pain and / or discomfort, which made them need more rest, but studies confirming it with accuracy are needed. Yes, there is an evidence to ensure that the postpartum exhaustion and the care of the baby make the mother require more rest after delivery. However, the emotional state, the anxiety of taking care of the newborn, the hospital, the pain, the discomfort caused by the swelling, the bruises and the suture of the perineal trauma are factors that affect the sleep patterns of the puerperal women24.
Regarding thePattern 6 Cognitive - Perceptual, during the first 24 to 48 hours after delivery, those women with episiotomy had a severe level of pain (6-7 points) according to the EVA scale, being lower in those who suffered a tear. 10 days after delivery, the women who suffered a tear had no pain in the area nor took painkillers, however women with episiotomy still needed them, the most frequent being Ibuprofen.
If we refer to the available evidence, we found an author25who assessed postpartum pain in the first, second and tenth days, obtaining that less pain was obtained by women with intact perineum, followed by women with I and II degree tear, then women with episiotomies and finally women with III and IV degree tear as the biggest pain.
The pain is associated as a consequence of episiotomy. During the first 24 hours it reaches its maximum point, it causes pain to 85-95% of the women 48 hours later, and from the third day it begins to remit. This percentage drops to 32% after one week, and to 23% after 10 days. It can be influenced by other factors such as receiving the epidural14)(15.
Other researchers found that women with episiotomy had more pain in the perineal region to rest, sit, and move on the first day after vaginal delivery, compared to those with the intact perineum and with tears of I, II, and III degrees26. Pain complaint was reported in the first 24 hours after vaginal delivery with episiotomy16. A cohort study conducted in Africa compared the occurrence of perineal pain in women with and without episiotomy. He found that the 88 women who underwent the procedure (100%) felt pain in the perineum for 24 hours or more, compared to only 7 of the 159 women without episiotomy (27 with tear and 132 with intact perineum, total 4, 4%), with a statistically significant difference (p = <0.0001)27.
A study developed in Germany with women undergoing episiotomy found that they had perineal pain to sit, walk, lie down and in the pattern of elimination between 1 and 5 days after delivery; women included in the group of restrictive episiotomy policies had less pain compared to liberal use28.
A review of the available bibliography was made, finding a summary of evidence of UpToDate in which conflicting results appear; some studies found less pain in women with intact perineum and spontaneous tear immediately after delivery and three more months than in others with episiotomy. Others did not find significant differences in this aspect between both populations29.
Lastly,Pattern 9 Sexuality - Reproductionis not altered in the group of episiotomies based on the data collected in our study. However, two of the three women who had resumed sexual activity one month after giving birth had a tear (5.89%) and only one episiotomy, which leads us to believe that in the latter case it is decided to start later because of pain or fear to suffer it. However, studies with a larger sample obtained that dyspareunia is a quite common problem in women with episiotomy than in those with another type of injury30.
CONCLUSIONS
Spain is one of the countries with the highest rate of instrumental births, episiotomies, and inductions in Europe, with the negative consequences that this entails for women, both in short and long term.
There is a clearly negative influence of the performance of episiotomies in relation to tears in postpartum recovery, being a technique that produces significant pain and limits for many of the daily activities.
The fulfilment of the episiotomy generates clear problems in the puerperium, mainly focused on Pattern 1 (limitation of daily activities), Pattern 3 (ache when urinating and defecating and the need to use laxatives), Pattern 4 (help for the care of the newborn), Pattern 5 (rest periods during the day) and Pattern 6 (severe pain). Many of these alterations are interrelated with each other, being the point of encounter the pain produced by the perineal injury, so that an alteration in Pattern 6 causes others to be affected.
In the clinical puerperium, women with tears do not have altered the Functional Patterns.
It is considered necessary to carry out more studies to reaffirm the data obtained, especially in those patterns less studied in relation to the puerperium.
REFERENCIAS
1. Arriaza Romero PD, Granados León S, Martinez Atienza JF, Sánchez Jiménez C. Técnicas Básicas de Enfermería. 1ª ed. Madrid: Ediciones Paraninfo; 2013 [citado 07 May 2016]. 670 p. Disponible en: https://books.google.es/books?id=C_1RAgAAQBAJ&printsec=frontcover&hl=es&source=gbs_ge_summary_r&cad=0#v=onepage&q&f=false [ Links ]
2. Cabay Basantes MJ, Aguagallo T, Marina V. Principios bioéticos en el cuidado de Enfermería y la satisfacción en las necesidades de seguridad y autoestima en las pacientes con labor de parto y puerperio atendidas en el servicio de ginecología del Hospital Provincial General Docente Riobamba. Murcia [Tesis Doctoral en Internet]. Riobamba: Universidad Nacional de Chimborazo; 2013 [citado 07 May 2016]. 296 p. Disponible en: http://dspace.unach.edu.ec/bitstream/51000/1225/1/UNACH-EC-ENFER-2013-0021.pdf [ Links ]
3. Cruz Maroto E. Incidencia y prevalencia del dolor perineal tras parto vaginal [investigación para Tesis Doctoral]. Reduca [Internet]. 2009 [citado 07 May 2016]. Disponible en: https://www.revistareduca.es/index.php/reduca-enfermeria/article/view/59/52 [ Links ]
4. Episiotomía. Oxford Dictionaries [Internet]. 2016 [citado 07 May 2016]. Disponible en: http://www.oxforddictionaries.com/es/definicion/espanol/episiotomia [ Links ]
5. Organización de Consumidores y Usuarios. Demasiadas episiotomías en España. OCU [Internet]. 2015 Feb [citado 07 May 2016]. Disponible en: http://www.ocu.org/salud/derechos-paciente/noticias/episiotomias [ Links ]
6. Alperin M, Krohn M, Parviainen K. Episiotomy and increase in the risk of obstetrics laceration in a subsequent vaginal delivery. Obstet Gynecol [Internet]. 2008 Jun [citado 07 May 2016]; 111(6):1274-1278. Disponible en: https://www.researchgate.net/publication/5334611_Episiotomy_and_Increase_in_the_Risk_of_Obstetric_Laceration_in_a_Subsequent_Vaginal_Delivery [ Links ]
7. European Perinatal Health Report: Health and Care of Pregnant Women and Babies in Europe in 2010. Euro-Peristat Network [Internet]. 2010 [citado 07 May 2016]. Disponible en: http://www.europeristat.com/images/doc/EPHR2010_w_disclaimer.pdf [ Links ]
8. Recio Alcaide A. La atención al parto en España: Cifras para reflexionar sobre un problema. Dialnet [Internet]. 2015 [citado 07 May 2016]; 18:13-26. Disponible en: https://dialnet.unirioja.es/descarga/articulo/5106931.pdf [ Links ]
9. Grupo de trabajo de la Guía de Práctica Clínica sobre Atención al Parto Normal. Guía de Práctica Clínica sobre la Atención al Parto Normal. Plan de Calidad para el Sistema Nacional de Salud del Ministerio de Sanidad y Política Social. Agencia de Evaluación de Tecnologías Sanitarias del País Vasco (OSTEBA). Agencia de Evaluación de Tecnologías Sanitarias de Galicia (Avalia-t). 2010 [citado 07 May 2016]. Guías de Práctica Clínica en el SNS: OSTEBA Nº 2009/01. Disponible en: http://www.guiasalud.es/GPC/GPC_472_Parto_Normal_Osteba_compl.pdf [ Links ]
10. Ballesteros Meseguer C. Factores que Condicionan la Práctica de la Episiotomía en el Marco de la Estrategia de Atención al Parto Normal en un Hospital Universitario de la Región de Murcia [Tesis Doctoral en Internet]. Murcia: Universidad de Murcia; 2014 [citado 09 May 2016]. 296 p. Disponible en:http://www.tdx.cat/bitstream/handle/10803/134965/TCBM.pdf?sequence=1 [ Links ]
11. Sevilla Hernández MG. Situación actual del procedimiento de la episiotomía en el Complejo Hospitalario Universitario del Área II del Servicio Murciano de Salud [Trabajo Fin de Grado]. Murcia: Universidad de Murcia; 2015 [citado 07 May 2016]. [ Links ]
12. López A. La madre no controla el parto. Diario online El Mundo [Internet]. 2015 Feb [citado 07 May 2016]. Disponible en: http://www.elmundo.es/salud/2015/09/14/55f1cd3122601d47428b45a5.html [ Links ]
13. Ministerio de Sanidad, Servicios Sociales e Igualdad. Observatorio de Salud de las Mujeres (OSM). Informe del Estado de Situación de la Atención al Parto Normal en el Sistema Nacional de Salud. 2012 [citado 09 May 2016]. [ Links ]
14. Ghosh C, Mercier F, Couaillet M, Benhamou D. Quality-assurance program for the improvement of morbidity during the first three postpartum days following episiotomy and perineal trauma. Acute Pain [Internet]. 2004 [citado 09 May 2016]; 6:1-7. Disponible en: https://www.researchgate.net/publication/244797207_Quality-assurance_program_for_the_improvement_of_morbidity_during_the_first_three_postpartum_days_following_episiotomy_and_perineal_trauma [ Links ]
15. Juste-Pina A, Luque-Carro R, Sabater-Adán B, Sanz-de Miguel E, Viñerta-Serrano E, Cruz-Guerreiro E. Episiotomía selectiva frente a episiotomía rutinaria en nulíparas con parto vaginal realizado por matronas. Matronas Prof [Internet]. 2007 [citado 09 May 2016]; 8 (3-4):5-11. Disponible en: http://www.federacion-matronas.org/revista/matronas-profesion/sumarios/i/6702/173/episiotomia-selectiva-frente-a-episiotomia-rutinaria-en-nuliparas-con-parto-vaginal-realizado-por-matronas [ Links ]
16. Amorim Francisco A, Junqueira Vasconcellos de Oliveira SM, Barbosa da Silva FM, de Oliveira Santos J, Leister N, Gonzalez Riesco ML. Efecto del dolor perineal en las actividades de mujeres sometidas a episiotomía. Index Enferm [Internet]. 2012 Sept [citado 09 May 2016]; 21(3):150-154. Disponible en: http://scielo.isciii.es/scielo.php?pid=S1132-12962012000200009&script=sci_arttext&tlng=pt [ Links ]
17. Dannecker C, Hillemanns P, Strauss A, Hasbargen U, Hepp H, Anthuber C. Episiotomy and perineal tears presumed to be imminent: randomized controlled trial. Acta Obstet Gynecol Scand [Internet]. 2004 Apr [citado 11 May 2016]; 83(4):364-8. Disponible en: http://www.ncbi.nlm.nih.gov/pubmed/15005784 [ Links ]
18. Hartmann K, Viswanathan M, Palmieri R, Gartlehner G, Thorp J Jr, Lohr KN. Outcomes of routine episiotomy: a systematic review. JAMA [Internet]. 2005 May [citado 11 May 2016]; 293(17):2141-8. Disponible en: http://jama.jamanetwork.com/article.aspx?articleid=200799 [ Links ]
19. Grupo de trabajo de la Guía de práctica clínica de atención en el embarazo y puerperio. Guía de práctica clínica de atención en el embarazo y puerperio. Ministerio de Sanidad, Servicios Sociales e Igualdad. Agencia de Evaluación de Tecnologías Sanitarias de Andalucía; 2014 [citado 11 May 2016]. Guías de Práctica Clínica en el SNS: AETSA 2011/10. Disponible en: http://www.msssi.gob.es/organizacion/sns/planCalidadSNS/pdf/Guia_practica_AEP.pdf [ Links ]
20. Mueller-Lissner SA. and Wald A. Constipation in adults. BMJ Clin Evid [Internet]. 2010 Jul [citado 11 May 2016]. Disponible en: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3217654/pdf/2010-0413.pdf [ Links ]
21. Alexandre CW, Kimura AF, Tsunechiro MA, Oliveira SMJV. A interferência da dor nas atividades e necessidades da puérpera. Rev Nurs [Internet]. 2006 [citado 12 May 2016]; 93(3):664-668. Disponible en:https://www.researchgate.net/publication/285819108_A_interferencia_da_dor_nas_atividades_e_necessidades_da_puerpera [ Links ]
22. Andrews V, Thakar R, Sultan AH, Jones PW. Are mediolateral episiotomies actually mediolateral? BJOG [Internet]. 2005 Aug [citado 12 May 2016]; 112(8):1156-1158. Disponible en: http://onlinelibrary.wiley.com/doi/10.1111/j.1471-0528.2005.00645.x/full [ Links ]
23. Sartorato Beleza AC, Jorge Ferreira CH, de Sousa L, Spanó Nakano AM. Mensuração e caracterização da dor após episiotomia e sua relação com a limitação de atividades. Rev Bras Enferm [Internet]. 2012 Mar-Apr [citado 12 May 2016]; 65(2):264-8. Disponible en: http://www.scielo.br/pdf/reben/v65n2/v65n2a10.pdf [ Links ]
24. Pimenta CAM. Dor: manual clínico de enfermagem. 2000 [citado 12 May 2016]. [ Links ]
25. Klein MC, Gauthier RJ, Robbins JM, Kaczorowski J, Jorgensen SH, Franco ED et al. Relationship of episiotomy to perineal trauma and morbility, sexual disfunction, and pelvic floor relaxation. Am J Obstet Ginecol [Internet]. 1994 Sept [citado 13 May 2016]; 171:591-598. Disponible en: https://www.researchgate.net/publication/15107455_Relationship_of_episiotomy_to_perineal_trauma_and_morbidity_sexual_dysfunction_and_pelvic_flor_relaxation [ Links ]
26. Williams et al, 2007, citado por Browne M, Jacobs M, Lahiff M, Miller S. Perineal injury in nulliparous women giving birth at a community hospital: reduced risk in births attended by certified nurse-midwives. J Midwifery Womens Health [Internet]. 2010 May-Jun [citado 13 May 2016]; 55(3):243-2499. Disponible en: http://www.medscape.com/viewarticle/723966 [ Links ]
27. Sule ST, Shittu SO. Puerperal complications of episiotomies at Ahmadu Bello University Teaching Hospital Zaria, Nigeria. East Afr Med J [Internet]. 2003 Jul [citado 13 May 2016]; 80(7):351-356. Disponible en: http://www.uonbi.ac.ke/journals/files/journals/1/articles/557/submission/review/557-2058-1-RV.pdf [ Links ]
28. Dannecker C, Hillemanns P, Strauss A, Hasbargen U, Hepp H, Anthuber C. Episiotomy and perineal tears presumed to be imminent: randomized controlled trial. Acta Obstet Gynecol Scand [Internet]. 2004 Apr [citado 13 May 2016]; 83(4):364-368. Disponible en: http://onlinelibrary.wiley.com/wol1/doi/10.1111/j.0001-6349.2004.00366.x/full [ Links ]
29. Robinson JN. Approach to episiotomy. UpToDate [Internet]. 2016 Apr [citado 13 May 2016]. Disponible en: http://www.uptodate.com/contents/approach-to-episiotomy [ Links ]
30. Turmo M, Echevarría M, Rubio P, Almeida C. Cronificación del dolor tras episiotomía. Rev Esp Anestesiol Reanim [Internet]. 2015 [citado 15 May 2016]; 62(8): 436-442. Disponible en: http://www.sciencedirect.com/science/article/pii/S0034935614002941 [ Links ]
Received: August 28, 2017; Accepted: November 10, 2017
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
