










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.18 n.54 Murcia Apr. 2019 Epub Oct 14, 2019
https://dx.doi.org/10.6018/eglobal.18.2.337321
Originals
Stress, burnout and depression in nursing professionals in intensive care units
1Nursing Student, Scholar of the Scientific Initiation Institutional Program (PIBIC/CNPq) of the Seune College, Researcher of the Group of Studies Dona Isabel Macintyre, Federal University of Alagoas (GEDIM/UFAL/CNPq). Maceió (AL), Brazil. enfreinaldomoura@gmail.com
2Nurse, Specialist in Libras from the Cândido Mendes University, Professor of the Seune College and Cesmac University Center, Researcher of the GEDIM/UFAL/CNPq. Maceió (AL), Brazil.
3Occupational Nurse, MSc in Nursing from the UFAL, Professor of the Nursing Technician Course of the Federal Institute of Alagoas. Maceió – AL, Brazil.
4Nurse, PhD i Nursing from the Federal University of Rio de Janeiro, Professor of the Stricto Sensu Postgraduate Program in Nursing of the UFAL and Leader of the GEDIM/UFAL/CNPq. Maceió – AL, Brazil.
5Nurse, Master’s Student from the Post-Graduation in Nursing of the UFAL, Researcher of the GEDIM/UFAL/CNPq. Maceió – AL, Brazil.
6Nurse, MSc in Intensive Care from the Intensive Care Brazilian Society, Professor of the Lato Sensu Post-Graduation in Health of the Integrated College of Patos. Maceió – AL, Brazil.
Objective:
To analyze the preliminary levels of stress, Burnout and depression among nursing assistants and technicians working at intensive care units of some private hospital services.
Method:
A quantitative-analytical and cross-sectional study in three private hospital services and in four intensive care units. The data collection instrument consisted of five validated questionnaires: socioeconomic and demographic profile, stress symptomatology in Bacarro, Work Stress Scale, JBeili Questionnaire, Brazilian version inspired by the Maslach Burnout Inventory (HSS - Human Services Survey) and the Beck Depression Inventory, all data were treated using analytical statistics.
Results:
The study included 72 nursing assistants and technicians, the majority was female (52.8%), nursing technician (95.8%), aged 31-35 years old (27.8%), married (54,2%) and with two or more employments (62.5%). They were classified with moderate stress (70.8%) in Bacarro, with mild stress (66.7%) on the work stress scale, in initial phase of Burnout syndrome (68.1%) and with dysphoric-depressive symptoms (45,8%).
Conclusion:
Intensive care units are potentially tensiogenic unhealthy environments and with high absenteeism rates. The study participants keep double working hours, mostly women and with children, presenting high scores of stress, Burnout and depression.
Key words: Nursing Research; Working Conditions; Burnout, Professional; Occupational Health Nursing; Intensive Care Units
INTRODUCTION
The study object were stress, Burnout syndrome and depressive symptoms in nursing assistants and technicians (NATs) who work at intensive care units (ICUs) of some private hospital services (PHSs). This study had two motivations: the first one is that one study member has worked as nursing technician (NT) for 10 years in two PHSs, is currently a Nursing student and observed the silent illness of labor colleagues; the second is the gap in databases covering such object in these services, and in the northeast region.
ICUs have specialized professionals with technological resources to deal with patients in serious situations, the NATs are as important part of the work team in these environments and directly related to ongoing nursing care1. In this assistance, the NATs are subjected to various forms of difficulties, accumulating various functions and obliged to develop a series of activities, which, in most cases, are not their responsibilities2. In the meantime, at some hospital services, the nursing professionals work in unhealthy and stressful environments, with excessive physical and mental labor, poor remuneration and in inadequate conditions for their occupational health2. This unhealthy condition, accompanied by personal problems of these professionals, may cause alteration in the worker’s psychophysiology, reflecting from a primary irritability, through a quiet mental illness, by constant confrontation of stressors present in in ICUs3.
The occupational stress is the set of subjective phenomena experienced internally and externally, individually and distinctive regarding stressors in the workplace, and the effect of mutual influence and excessive labor and imposed resources, in the long term, causing a high rate of absenteeism, which results in expenses for the State, the worker and the employer, which, alone, justifies this study2 4.
Nursing is a poorly remunerated profession and whose professionals have other employment to compose a larger income, thus increasing their work overload, maintaining daily contact with highly depolarizing situations, i.e., which require professionals’ constant adaptation with the working environment, and these conditions interfere in the occupational health of NATs5 6.
The study is important and relevant since it considers two important surveys in different studies, the first one7 that the illness of NATs who are part of the patient’s care in the healthcare network at PHSs can generate great consequences, and the second1, by the lack of knowledge about the object in databases involving PHSs. Therefore, the objective was to analyze the preliminary levels of stress, burnout and depression among NATs who work in CUs of some PHSs.
MATERIAL AND METHODS
Quantitative-analytical and cross-sectional study. Only three out of the eight PHSs from Alagoas agreed to be part of the study. The study was developed in medium- and large-sized PHSs, named in accordance with the confidentiality principles: Jupiter Hospital (JH), Saturn Hospital (SH) and Uranus Hospital (UH). The UH has an intensive care unit (ICU) with eight beds, the JH has also a Cardiologic unit with 12 beds. The SH has two ICUS, called A/Cardiology ICU with 10 beds and B/General ICU with nine beds.
Based on Resolution 293/2004 by the Federal Nursing Council (COFEN)8, in force when the study occurred, which establishes the minimum parameters to estimate the amount of nursing professionals for intensive care, with often 100% occupation, at ICUs, the recommendation is the proportion of 02 Beds/01 NAT, with a safety margin of 10%, i.e., the three PHSs should have 116 nursing technicians and assistants.
The study participants were selected by simple random sampling calculation, considering a confidence level of 95% and a maximum error of 0.5%, and sample calculation totaled 90 NATs. Prior to this calculation, some inclusion criteria were listed: NATs from the care team with minimum service time > one year in the ICUs and who signed the Informed Consent Form (ICF). Exclusion criteria: pregnant NATs, on medical leave or vacation and those who delivered incomplete questionnaires.
After entering the data collection field, the sample needed to be recalculated, due to insufficient nursing staff dimensioning in some ICUs. After applying the inclusion and exclusion criteria, 72 NATs remained from the universe of 90 NATs, corresponding to the established “n”, considered statistically accepTable. The variables chosen were: gender, age, marital status, employment, education, nursing function, time working in the ICU and in the hospital service and the scores of the questionnaires proposed in the data collection instrument.
The data collection instrument consisted of five validated questionnaires: the socioeconomic and demographic profile based on the variables chosen for the study; determination of stress through its symptomatology, with experienced problems in the past two months with the Bacarro Test9(composed by items, with 00 corresponding to the professional with no problems, 01 occasionally and 02 often); the third, the Work Stress Scale (WSS)10(addressing both a stressor, as a reaction to this and the impact on the work environment); the fourth, inspired by the Maslach Burnout Inventory (MBI) version HSS (Human Services Survey) with scores suggestive for depolarization of the JBeili questionnaire11; and the fifth, the Beck Depression Inventory (BDI)12(questions that assess depressive symptoms). None of the instruments used replaces the medical or psychological diagnosis.
In April and June 2016, data collection occurred, following two steps: first, after explanations about the research objectives, the NATs received the ICF in their work environment for signature, and secondly, the specific scores were applied and made available to the study participants. The data were grouped into a database of Microsoft Excel®and analyzed by the analytical statistics in the Statistical Software Package for Social Science (SPSS) version 20 and Statistical Analysis System 9.02, which correlated variables, tested the hypothesis through the Chi-square test with the significant P value < 0.05, grouped in Tables and graphs for better presentation.
The study was approved by the Research Ethics Committee of the Federal University of Alagoas, under opinion number: 1,350,399 and CAAE: 50677015.9.0000.5013. However, data collection only began four months after approval, because the PHSs delayed this phase.
RESULTS
The study participants (n=72) were NATs who work in four ICUs of three large-sized hospitals, considering that one of the hospitals has two ICUs, thus distributed: JH 29.2%; SH 22.2%; UH ICU A 22.2% and UH ICU B 26.4%. Based on the socioeconomic variables, two sample (n=72) profiles were proposed, divided to better understand the social and the economic-professional profile.
The social profile had predominance of: women (52.8%), nursing technicians (95.8%), with medium education (62.5%), marital status married (54.2%), young adults - 31 to 35 years (27.8%) and those who responded having children (69.4%) (Table 01).
Table 01. Social Profile, according to Gender, Professional Category, Marital Status, Age Group and Children. Maceió (AL), Brazil, 2016.
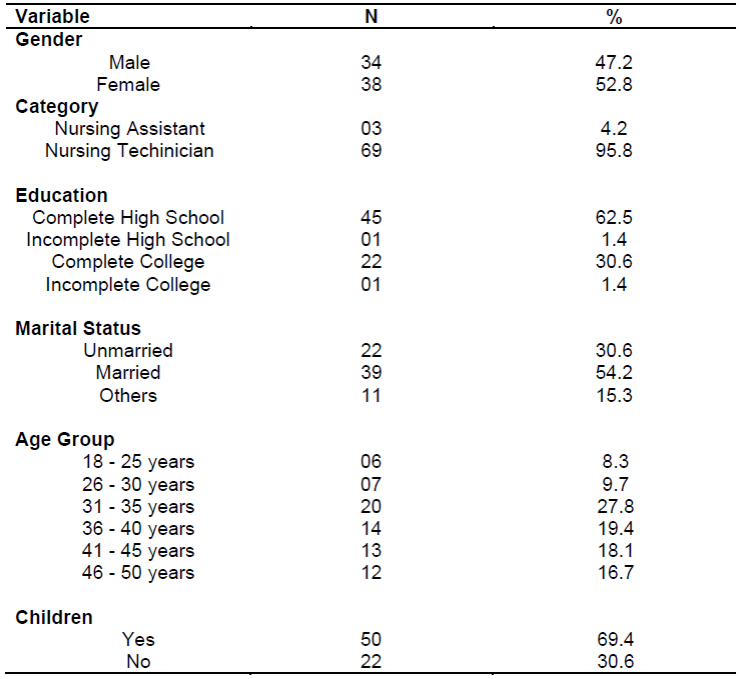
Source: Research Data.
Table 02describes the economic and professional profile of NATs, showing that the majority owned their own house (75%), service time in the ICUs from three to five years (37.5%), time since graduation and working time from six to 10 years (34.7%), two or more (69.4%) employments and, in relation to the work shift, the majority worked at all (morning, afternoon and evening) (93.1%).
Table 02. Economic and Professional Profile, Residence, Time of Service in the Intensive Care Unit, Work Time, Employment and Work Shift. Maceió (AL), Brazil, 2016.
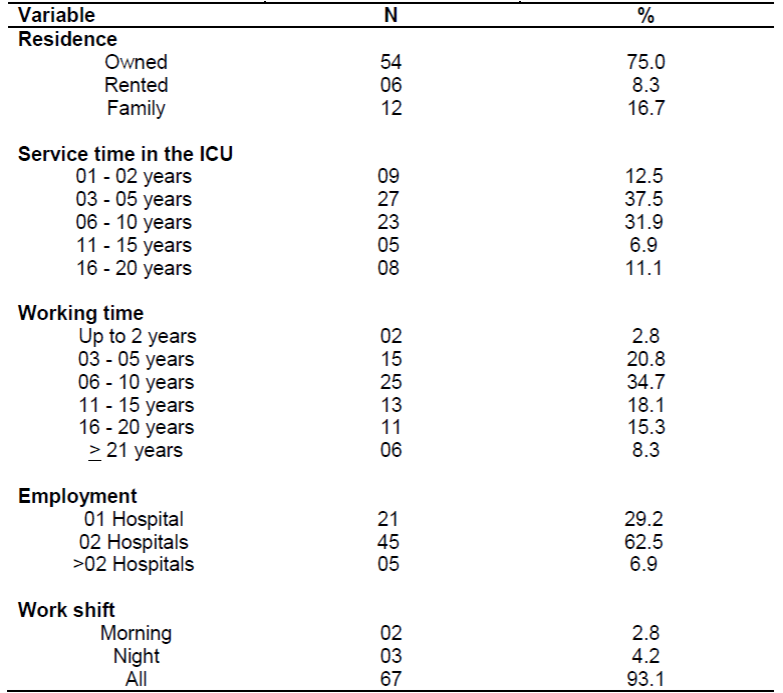
Source: Research Data.
Once presented the characteristics of NATs, there is need to show the distribution according to the dependent variable, which is, the stress levels of these professionals.Graph Ishows data about the evaluation of stress symptoms, assessed from Baccaro’s test (1998), which showed that the majority has moderate stress (70.8%).
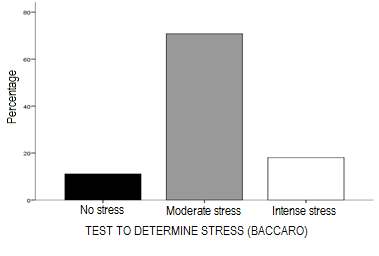
Source: Research Data.
Graph I. Stress Levels according to Baccaro’s Test. Maceió (AL), Brazil, 2016.
The results of the WSS show a prevalence of mild stress (68.7%), in relation to the sum of moderate and intense stress scores (15.6%) (Table 03).

Another distribution described was the result of the levels of Burnout Syndrome, according to the preliminary questionnaire of Jbeili, which classified most NATs in the initial phase (68.1%) and the sum of the possibility of developing moderate phase and considerable phase deserve attention (31.9%), since none of them had zero development (Graph II).
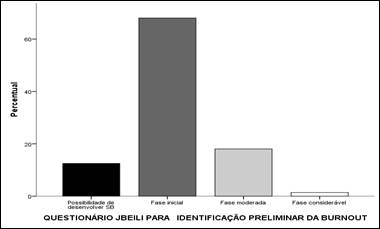
Source: Research Data.
Graph II. Levels of Burnout Syndrome according to Jbeili Questionnaire (MBI). Maceió (AL), Brazil, 2016.
For the description of the depressive symptoms, the pattern of normality was, in its majority, 54.2%; however, dysphoria occurred along with depressive symptoms, with nearly half of the sample (45.8%), compared to those who were within the pattern of normality according to the BDI.
Table 04. Depression Levels according to the Níveis de Depressão segundo o Beck Depression Inventory. Maceió (AL), Brazil, 2016.

Source: Research Data.
Considering P < 0.01, there were some significant statistical associations. Analyzing the others, only three stood out, which, in the first one, NATs with “moderate/intense stress” on Bacarro (88.9%) are likely to develop “moderate or considerable phase” of the Burnout Syndrome (18.1%); in the second, NATs with “Moderate stress/High level of stress” in the WSS (15.3%) are likely to develop a “Considerable or moderate phase” of the Burnout Syndrome (19.5%) and the third, which shows that, according to the BDI, the age range “suggestive to depression” is above 35 years.
DISCUSSION
The material and method topic of this study brought a datum, which showed that the ICUs of the surveyed PHSs had a reduced number of NATs and also had nursing assistants, who, according to Resolution 293/2004 of Cofen, should not be in the care team. Furthermore, there was also incorrect personnel dimensioning8.
A study13performed at the Clinical Hospital of the College of Medicine of the University of São Paulo (ICHC-FMUSP), Brazil (BR), whose objective was to analyze the influence of the work load, stress, Burnout, satisfaction and perception of the care environment by the nursing team with the presence of adverse events (AEs) in the ICU, points out that the possible consequences of this poor dimensioning, added to inadequate material resources, may favor the appearance of alarming rates of EAs notified and workers’ illness.
A systematic review14, which aimed to know the scientific production on the nursing worker's health, explains that the insufficient number of workers in the ICUs is not only a nursing problem, but also to: the clients assisted by their care, the State and the employer, because, when the professional gets sick, he/she is incapable of offering a quality service and overloads the others, thus contributing to the increased labor absenteeism, thus corroborating another aforementioned study13).
Most NATs are men, with prevalence of young adults and married (Table 01), which can be explained by a study15of Cofen, carried out by the Oswaldo Cruz Foundation (FIOCRUZ), with the goal of raising the profile of Brazilian nursing, which points out that the Brazilian Nursing is a mostly female profession, with a “trend to masculinization of the category”, young adults and married, converging with the data of this study. Complementing13, most NATs in their sample had children (62.3%), corroborating the results of this study (Table 01) and others aforementioned2 6 7 11.
Another scientific production of similar methodological design16, carried out at the Clinical Hospital of Botucatu of the State University of São Paulo, BR, which aimed to assess the level of Burnout Syndrome in nursing professionals in the ICU, pointed out that, in relation to the education variable, most NATs had secondary education (69.5%), their own homes (68%), as described inTable 02. The other variables, gender, age and children, converged with this study, and with other productions mentioned previously13 15.
Another study conducted at a university hospital in the state of Rio Grande do Sul, BR, with similar methodological design and with the objective of evaluating the association between psychological demands, control over work and reduced capacity to work in nursing workers3, stresses the convergence with this study (Tables 01and02), when describing the predominance of females among NATs, marital status married, schooling, and among the professional categories, NT stands out, whichever was greater depth in their research, because, in relation to more than one employment, the explanation was the poor remuneration, which, in the characterization of the professionals involved, was not mentioned (Tables 01and02).
The aforementioned authors3corroborate other production also mentioned, when confirming that nursing is a poorly remunerated profession and that its professionals have other employments to compose a larger income, thus increasing their work overload5.
The working dynamics at ICUs is potentially stressful and, when combined with personal problems, may cause alteration in the worker’s psychophysiology, leading to a quiet mental illness, or even a primary constant irritability3,4. In relation to the schooling variable and the search by some NATs for graduation, there is a significant proportion (Table 01), which may have been driven by the agreement of the federal government, through the Ministry of Education, which encouraged the expansion of higher education in Brazil and made the possibility of reconciling work and study17. Mentioning again other production16, in relation to the working time of NATs in the ICUs and the time of profession, the cited mean was up to 10 years of work, converging with the data specified inTable 02.
In relation to work shifts, there was a divergence of the study with other scientific production18, held in the city of São Paulo, BR, in eight ICUs of a public hospital service, which pointed out that the prevalent work shift of participants in the study were the morning and the afternoon, differently from this study (Table 02), which described that most NATs worked in all shifts (morning, afternoon and evening), however, in agreement with the results presented in other works14 17 19corroborate the data presented here (Table 02).
A scientific synthesis of integrative nature19suggests that the night work can affect harmfully the health of nursing workers, but they often choose this, for their personal and professional needs, such as: family (home and children care), financial (need for more than one job and/or night extra) and personal reasons (studying during the day or living far from the job), maintaining harmony with the description of this study (Tables 01and02), when mentioning that most of the population of this review were women, married and with children, i.e., leading to a reflection that they also work at home.
Graph I, in relation to the levels of stress among NATs from the questionnaire used, pointed out that the majority was with scores of moderate stress, which, according to studies already cited4 18, the explanation that corroborates this situation is that the nursing care exposes to various factors that generate stress and other mental pathologies, because this assistance involves the systematization of emotions, aspirations, expectations, nostalgic feelings from the context present in intensive environments. Some authors13, when showing that most of their study participants also presented with a moderate score (77.40%), converge with the aforementioned results (Graph I).
Another literary synthesis20, which had aimed at identifying the influence of workloads in occupational health nursing, pointed out that the working conditions and environment of the nursing team act as predisposing factors to work overload, and this buildup in the working environment can influence the worker's illness. There is harmony with the data presented in this study, in relation to the majority of the employment option variable (Table 02), also corroborating other authors cited3 13, because two or more employments serve to compose the income. Nevertheless, this review raised another point, which studies such as this one can identify the influences for the workers’ illness and enable the implementation of organizational actions for prevention of occupational accidents and illnesses.
Within the perspective of illness of NATs described by the aforementioned authors13,20, they discuss some factors that can cause the nursing worker’s illness, such as: work overload, professional devaluation, unhealthy environment and lack of investment in actions to reduce such sectorial inconveniences, thus corroborating other studies1 2 4 13.
Moreover, another production with a similar methodological design, also financed by public resources for being a scientific initiation performed at ICUs and semi-intensive care units of the University Hospital of the University of São Paulo, BR21, showed that most study participants presented mild WSS score (54%) and the minority, high level of stress, thereby converging withTable 3. An explanation for the mild score classification in this study is that, although the intensive environment may contribute to the highest levels of stress, they can be dissipating or fleeing with coping strategies used focused on escaping the problem and not on solving it21.
Other already mentioned authorships18corroborate this study on the issue of stress levels in relation to its signs and symptoms, as well as the stressors (Graph 1andTable 03) and some sample characterization data (Tables 01and02). A small portion of the sample was in considerable Burnout score (12.5%), thus corroborating data fromGraph II; however, it diverged from the remaining data of the same graph, because the majority was classified in the initial, moderate and considerable score. The studies were carried out in different regions and hospital services.
Another literary synthesis22, which identified the factors that influenced the performance of nursing professionals in the ICUs and strategies that favored the assistance to the patient in the literature, pointed out that all factors that generate stress in nursing professionals worsen probably due to the lack of interest of leaders and managers of hospital services, which may lead to burnout syndrome, since it is a response to stressor agents related to repetitive work, thus corroborating the aforementioned studies13,18.
A qualitative production2, which gave voice to its participants, carried out in an Intensive Care Center, Rio de Janeiro, BR, which characterized situations that favored or interfered the Quality of Working Life (QWL) of intensive care nursing and analyzed the impact of the QWL in nursing workers’ health of the intensive care pointed out that some of the changes can be divided into psychophysiological and psychological, mental and emotional.
The psychophysiological ones are: fatigue, headaches, insomnia, body pains, palpitations, bowel changes, nausea, shivering, cold extremities, cardiovascular diseases and constant colds. Psychological, mental and emotional aspects are: decreased concentration and memory, indecision, confusion, loss of sense of humor, anxiety, nervousness, depression, anger, frustration, worry, fear, irritability and impatience2, thus corroborating the synthesis of other integrative reviews1 4 22, which mention that the illness of NATs in ICUs is a concerning factor, since it causes significant changes in these workers, explicit in almost half of the study sample (Table 4).
Another study23, which addressed the depression with the same data collection instrument used in this study (Table 4), conducted in three PHSs, but in another geographical reality, northwestern state of São Paulo, BR, partially corroborated the data of this study, because it classified most NATs (70%) as without depression or with mild depression and the minority (30%) with dysphoria (moderate depression) through depression (severe depression). Such study23confirm the characterization data of this study (Table 1and 2) and obtained the same statistical association, which states that NATs aged over 35 years are more likely to develop some depressive symptom.
The other statistical associations aforementioned can be explained in two ways: the first, according to a study already mentioned above16, suggests that the professionals who work by employment regimes had higher chances of developing the Burnout Syndrome and the second, according to the studies1 2 13 14 18 22that evidence the development of this syndrome in NATS, because they are human beings caring for humans, with peculiar characteristics of their work, which cause the occupational illness. Double working shifts, occupational risks, precarious material resources and constant exposure to stressors, lead professionals, besides personal and family problems, to deal without any preparation with these problems9 11 13 17 18.
Another study conducted in the Northeast Region6, at a PHS in Ceará, BR, with a different methodological design, but with a sample composed only by nursing technicians, which aimed to investigate their working conditions, the impact of these conditions on these professionals’ health and the defense strategies used to face the resulting suffering, corroborated this study (Graphs I,II,Tables 3and4) as it explains that these professionals are daily exposed to various adverse conditions in a hospital environment, with high load of assignments of activities, which many times are not their responsibilities and in frequent contact with the suffering of patients and their families, and often create strategies to minimize the unhealthy environment, and not a more appropriate output, i.e., this buildup of problems will become present at some point, thus corroborating other studies already mentioned2 16 22.
A study24carried out in three PHSs of Rio Grande do Sul, BR, aiming to identify the frequency and intensity of moral suffering experienced by nurses, nursing technicians and assistants who work at African hospitals, suggests with some notes to reduce the rates of suffering in the professionals involved, such as: better organization of the work environment, privileging discursive and reflective spaces, valuation of tensiogenic and depolarizing situations, by hospital leaders, to offer a proper monitoring, or a way for these professionals to face trivial situations in a balanced way.
Corroborating the scientific production mentioned in the previous paragraph24, most of the studies cited above4 13 16 22suggest strategies for minimizing the physiological and psychological consequences of this silent illness, which should be executed by the institutional leaders and workers, including programs that encourage professional recognition, actions aimed at improving working conditions, investments in the process of health/satisfaction of their employees, staff dimensioning in accordance with the law8, a better financial remuneration, an awareness of the team regarding the problem and, most importantly, studies that assess periodically pathologies that address occupational diseases.
CONCLUSION
The proposed objective was achieved as the levels of stress, burnout and depression of NATs who work in the ICUs of some PHSs were described, correlating with the socioeconomic and professional profiles, and the hypothesis was ratified, when showing that NATs are getting sick silently.
In conformation with the addressed literature, the characterization of NATs was maintained, because the sample consisted mostly of nursing technicians, married, with complete secondary education and focusing on a university formative process, who work in all available shifts, with children, in productive age and with two or more employments. Despite the lack of an assertion about the reason for two or more employments, these literatures mention the poor remuneration of the category.
In relation to stress symptoms according to Baccaro, the majority is in the score from moderate to intense and, paradoxically, in the WSS, the majority presented with mild stress. The Burnout Syndrome predominantly had initial and mild scores, demonstrating that NATs are getting sick gradually and silently. Some significant statistical associations were also confirmed, showing that any professional with scores of stress in Baccaro and WSS is more likely to develop significant phase of Burnout Syndrome.
Another important fact is that, in relation to depressive symptoms, nearly half of the sample were dysphoric-depressive according to the BDI and that, according to other statistical association, the age range over 35 years is more likely to be in this pattern. To decrease the factors related in the ICUs, a greater concern of leadership of hospital services is necessary, as well as an awareness of NATs, who often do not perceive their illness.
Furthermore, further clarification about the study object is necessary, due to some limitations in the research, from the study time, which was a scientific initiation, through the type of study, which did not allow predicting cause/effect (cross-sectional) and the non-inclusion of workers on leave. Therefore, the research protocol should be expanded, especially in PHSs and in the northeast region.
Acknowledgements
To the Institutional Scholarship Program of Scientific Initiation, Seune College, linked to the National Council for Scientific and Technological Development (PIBIC/SEUNE/CNPq) and, particularly, to dear professors Rossana Marinho and Zandra Maria Cardoso Candiotti.
REFERENCES
1. Moura RS, Saraiva FJC, Barbosa MAS, Lima VP, Tomé AMCS, Albuquerque WMD. Absenteísmo da Equipe de Enfermagem das UTI Adulto no Brasil: revisão integrativa. Revista Hórus, v. 10, n. 1, p. 60-79, 2015. Available from: http://revistaadmmade.estacio.br/index.php/revistahorus/article/viewFile/3947/1905 [ Links ]
2. Ramos EL, Souza NVDO, Gonçalves FGA, Pires AS, Santos DM. Qualidade de vida no trabalho: repercussões para a saúde do trabalhador de enfermagem de terapia intensiva. J res fundam care. online 2014. abr./jun. 6(2):571-583. Available from: http://www.redalyc.org/articulo.oa?id=505750622013 [ Links ]
3. Prochnow A, Magnago TSBS, Urbanetto JS, Beck CLC, Lima SBS, Greco PBT. Capacidade para o trabalho na enfermagem: relação com demandas psicológicas e controle sobre o trabalho. Rev Latino-Am Enfermagem nov.-dez. 2013;21(6):1298-305. Available from: https://www.revistas.usp.br/rlae/article/viewFile/76053/79747 [ Links ]
4. Moura RS, Reis RP, Melo ES, Maranhão IM, Barbosa AMS. Estresse da Equipe de Enfermagem Atuante no Cuidado na UTI Adulto: Revisão Integrativa. Revista Hórus, v. 9, n.1, p. 35-52, 2014. Available from: http://revistaadmmade.estacio.br/index.php/revistahorus/article/viewFile/4223/1941 [ Links ]
5. Machado MH, Santos MR, Oliveira E, Wermelinger M, Vieira M, Lemos W, et al. Condições de trabalho da enfermagem. Rev Enferm Foco [Internet]. 2015 [citado 2016 Jul 03]; 6 (1/4): 63-71. Available from: http://revista.portalcofen.gov.br/index.php/enfermagem/article/view/695/305 [ Links ]
6. Barrocas PHN, Maciel RH, Maia LM. Condições de trabalho de técnicas de enfermagem de um hospital particular. Público Priv.(Online), n. 25, p. 77-100, 2015. [ Links ]
7. Bordignon M, Monteiro MI, Mai S, Martins MFSV, Rech CRA, Trindade LL. Satisfação e insatisfação no trabalho de profissionais de enfermagem da oncologia do Brasil e Portugal. Texto & Contexto Enferm [Internet]. 2015. Available from: http://www.scielo.br/pdf/tce/2015nahead/pt_0104-0707-tce-201500004650014.pdf [ Links ]
8. Brasil. Conselho Federal de Enfermagem (Cofen) - Resolução 293/2004. Available from: http://www.cofen.gov.br/resoluo-cofen-2932004_4329.html [ Links ]
9. Baccaro, A. Vencendo o estresse: como detectá-lo e superá-lo. 6a ed. Petrópolis: Vozes; 1998. [ Links ]
10. Paschoal T, Tamayo A. Validação da escala de estresse no trabalho. Rev Estud psicol (Natal) [Internet] 2004 [citado 2017 Mai 20]; 9(1): 45-52. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-294X2004000100006&lng=en&nrm=iso [ Links ]
11. Ariane QS, Adriana GB, Ana CSD, Viviane EPS. PERSPECTIVAS DE SÍNDROME DE BURNOUT NA EQUIPE DE ENFERMAGEM DA UNIDADE DE TERAPIA INTENSIVA. R pesq cuid fundam. online 2012. jul./set. 4(3):2672-78. Available from: http://www.redalyc.org/articulo.oa?id=505750894021 [ Links ]
12. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J (junho de 1961). An inventory for measuring depression. Arch Gen Psychiatry. 4: 561-71. Available from: https://www.ncbi.nlm.nih.gov/pubmed/13688369 [ Links ]
13. Padillha KG, Barbosa RL, Andolhe R, Oliveira EM, Ducci AJ, Bregalda RS, Dal Secco LM. Carga de trabalho de enfermagem, estresse/Burnout, satisfação e incidentes em unidade de terapia intensiva de trauma. Texto Contexto Enferm, 2017; 26(3):e1720016. Available from: http://www.scielo.br/pdf/tce/v26n3/0104-0707-tce-26-03-e1720016.pdf [ Links ]
14. Valença CN, Azevêdo LMD, Oliveira AG, Medeiros SSA, Malveira FAZ, Germano RM. The scientific production about occupational health of nursing. Rev de Pesq Cuid Fundamental [Internet] 2013. Available from: https://www.ssoar.info/ssoar/bitstream/handle/document/54871/ssoar-revpesquisa-2013-5-valenca_et_al-The_scientific_production_about_occupational.pdf?sequence=1 [ Links ]
15. Machado MH, Filho WA, Lacerda WF, Oliveira E, Lemos W, Wermelinger M, et al. Características Gerais da Enfermagem: o perfil sócio demográfico. Enferm Foco [Internet] 2015 [citado 2018 Mai 20] ; 7 (esp): 11-17. Available from: http://revista.portalcofen.gov.br/index.php/enfermagem/article/view/686/296 [ Links ]
16. Fernandes LS, Nitsche MJT, Godoy. Síndrome de Burnout em profissionais de enfermagem de uma unidade de terapia intensiva. J Rev Fund Care Online. 2017 abr/jun; 9(2):551-557. Available from: http://www.seer.unirio.br/index.php/cuidadofundamental/article/viewFile/4199/pdf_1 [ Links ]
17. Paula MFC, Vargas HM. A Inclusão do estudante-trabalhador e do trabalhador-estudante na Educação superior: desafio público a ser enfrentado. Rev Aval Educ Sup. [Internet]. 2013 [citado 2016 Ago 03]; 18(2): 459-486. Available from: http://submission.scielo.br/index.php/aval/article/view/97717/8279 [ Links ]
18. Andolhe R, Barbosa RL, Oliveira LM, Costa ALS, Padilha KG. Stress, coping and burnout among Intensive Care Unit nursing staff: associated factors. Rev esc enferm USP [Internet]. 2015 [citado 2017 Mai 16]; 49(spe):58-64. Available from: http://www.scielo.br/pdf/reeusp/v49nspe/en_1980-220X-reeusp-49-spe-0058.pdf [ Links ]
19. Silveira M, Camponogara S, Beck CLC. Scientific production about night shift work in nursing: a review of literature. J res fundam care. online 2016. jan./mar. 8(1):3679-3690. Available from: http://www.redalyc.org/comocitar.oa?id=505754103029 [ Links ]
20. Carvalho DP, Rocha LP, Barlem LGT, Dias JS, Schallenberger CD. Cargas de trabalho e a saúde do trabalhador de enfermagem: revisão integrativa. Cogitare Enferm. 2017 Jan/mar; 22(1): 01-11. Available from: http://www.saude.ufpr.br/portal/revistacogitare/wp-content/uploads/sites/28/2017/03/46569-194206-2-PB.pdf [ Links ]
21. Silva GAV, Silva GSA, SILVA RM, Andolhe R, Padilha KG, Costa ALS. Estresse e coping entre profissionais de enfermagem de unidades de terapia intensiva e semi-intensiva. Rev enferm UFPE on line., Recife, 11(Supl 2):922-31, fev., 2017. Available from: https://periodicos.ufpe.br/revistas/revistaenfermagem/article/view/13461/16153 [ Links ]
22. Hercos TM, Oliveira MS, Vieira FS, Sonobe HM. O Trabalho dos Profissionais de Enfermagem em Unidades de Terapia Intensiva na Assistência ao Paciente Oncológico. Revista Brasileira de Cancerologia 2014; 60(1): 51-58. Available from: http://www.inca.gov.br/rbc/n_60/v01/pdf/08-revisao-literatura-o-trabalho-dos-profissionais-de-enfermagem-em-unidades-de-terapia-intensiva-na-assistencia-ao-paciente-oncologico.pdf [ Links ]
23. Vargas D, Dias APV. Prevalência de depressão em trabalhadores de enfermagem de Unidade de Terapia Intensiva: estudo em hospitais de uma cidade do noroeste do Estado São Paulo. Rev Latino-Am Enfermagem set.-out. 2011;19(5). Available from: http://www.scielo.br/pdf/rlae/v19n5/pt_08.pdf [ Links ]
24. Dalmolin GL, Lunardi VL, Lunardi GL, Barlem ELD, Silveira RS. Sofrimento moral e síndrome de Burnout: existem relações entre esses fenômenos nos trabalhadores de enfermagem? Rev Latino-Am Enfermagem jan-fev 2014;22(1): Available from: https://www.periodicos.usp.br/rlae/article/download/76067/79789 [ Links ]
Received: July 13, 2018; Accepted: August 11, 2018
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
