










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.18 n.56 Murcia Oct. 2019 Epub Dec 23, 2019
https://dx.doi.org/10.6018/eglobal.18.4.361401
Originals
Work Overload Degree and Characterization of Caregivers of Older Adults with Type 2 Diabetes Mellitus
1Nursing Students at Universidad de Sonora, Department of Health Sciences. Nursing, Cajeme Campus. México.
2Full Time Teacher, Universidad de Sonora, Nursing Department, Centro Campus. México. reyna.hernandez@unison.mx
3Full Time Teacher, Coordinator of the Academia Program of the Bachelor’s Degree in Nursing, Universidad de Sonora, Cajeme Campus. México.
Objective
to determinate association between overload degree and sociodemographic characteristics of informal caregivers of older adults with type 2 diabetes mellitus.
Material and method
quantitative, descriptive, correlational, cross-sectional study of 83 informal caregivers of older adults with type 2 diabetes mellitus, from the northeast sector of Ciudad Obregón, Sonora, Mexico. The Zarit Scale was used to measure the overload degree, items regarding to sociodemographic characteristics were included.
Results
the profile of the caregiver with tendency to overload was: woman (81.9%), housewife (47%), with an average age of 40 years, married (53%), daughter of the older adult (72.3%), low schooling (66.1%) and monthly income less than or equal to 6,799 mexican pesos (51.8%), from one to three years as caregiver (54.2%) and dedicating more than 17 hours per day to it (51.8%). The 48.2% of the caregivers showed intense overload, 44.6% absence of overload and 7.2% slight overload. A statistically significant association was found (p=0.02) between the degree of overload and the variables marital status and occupation.
Conclusions
The significant association indicates that marital status and occupation is related to the caregivers perceived overload degree. It is relevant to propose interventions directed to these characteristics in order to reduce intense overload degree, which is a risk for caregiver’s health with this profile, since it is related with greater odds of medical, psychiatric and social morbidity and mortality.
Key words: workload; demographic data; caregivers; aged
INTRODUCTION
Worldwide there are around 700 million people aged 60 and above, it is estimated that by 2050 this amount will double, most of them living in less-developed countries 1. In Mexico, population dynamics have changed in recent years, showing a clear deceleration of population growth; in the last two decades, the population group that has grown the most has been adults over 65 years of age or above 2.
According to the results of the 2010 Population Census, in Mexico there were 10 million adults over 60 years of age, representing 9% of the total population 3, with an annual growth rate of 3.8%, which means that there are currently 14 million older adults. As a consequence of these changes, there is an ageing population.
The increase in life expectancy represents a challenge for the health of older adults in terms of Non-Communicable Diseases (NCDs); in the age group of 65 years or above, the main causes of death are ischemic heart disease, diabetes, and strokes 2; the aforementioned diseases are associated to greater functional impairment in the elderly. As a consequence, a large percentage of older people spend a long time with disabilities before they die 4.
Additionally, in the last decades the number of cases of diabetes, and its prevalence, has steadily increased 5. Currently, it is a social problem of global importance, not only because of the number of deaths it causes, but because of the high prevalence of dependent elderly people without the potential to meet their needs, therefore, family members (spouses, children, grandchildren, etc.) fulfill the responsibility; as a consequence, the progressive limitation of the functional performance of the older adult, who demands and needs attention and support to perform basic and instrumental daily activities, can create in the caregiver multiple psychosocial, family, and economic conflicts 6.
The person entrusted to cover basic and psychosocial needs of the elderly person can be defined as family caregiver, who is the individual who supervises the daily activities of the elderly person at home, and it is called family caregiver, because generally the person who assumes this responsibility is related to the elderly; it can also be called informal caregiver because it lacks formal preparation to perform care activities. As a result of the informality and responsibility, the care provided by family caregivers change the time dedicated to their recreational activities and social relationships, affecting their intimate life and freedom, causing problems in his emotional harmony7.
Therefore, the informal caregiver lives a situation of work overload that causes the tendencies to physical and mental imbalance, compromising in many cases the life of the caregiver. The demographic transition that is happening in our country includes high rates and prevalence of diabetes mellitus in older adults, thus, in the coming years the number of informal caregivers will rise.
Considering the above, the following hypothesis is proposed, that is, the degree of work overload is significantly related to the sociodemographic characteristics of informal caregivers of older adults with Type 2 Diabetes Mellitus. The objective of this study is to determine the relationship between the degree of work overload and the sociodemographic characteristics of informal caregivers of older adults with Type 2 Diabetes Mellitus living in the northeast sector of Ciudad Obregon, Sonora, Mexico.
MATERIAL AND METHODS
The study design was quantitative with correlational and cross-sectional approach. The study was conducted from April to August 2018. It was aimed to associate the dependent variable "informal caregiver work overload" with the independent variables that corresponded to sociodemographic characteristics, with a population of N = 105 adults over 60 years of age, with diagnosis of Type 2 Diabetes Mellitus and registered in the health center “Centro de Salud Urbano Norte (CSUN)” in Ciudad Obregon, Sonora 8. The following assumption were considered for the selected population: each elderly person with Type 2 Diabetes Mellitus, with at least one visit registered to the CSUN, would have one informal caregiver to provide care, in the understanding that there is no database of informal caregivers in Ciudad Obregon, Sonora.
Therefore, convenience sampling was used where n = 83 (IC = 95%) informal caregivers of these patients participated in the study. The inclusion criteria were: to be caregivers of adults older than 60 years diagnosed with Type 2 Diabetes Mellitus and registered in CSUN, to be a main informal caregiver, to be able to read and write, gender indistinct, without receiving economic remuneration for the care provided, without formal training to provide care, and accepted to participate in the study. Additionally, the exclusion criteria were: being a professional caregiver, with economic remuneration for providing care, having patients under 60 years of age or suffering from a different chronic degenerative disease, not accepting to participate in this study, and those who did not fully respond to the instruments used.
For the collection of information regarding sociodemographic characteristics, the Sociodemographic Data Sheet (CDS by its acronym in Spanish) created by the researchers was used. This is a multiple-choice questionnaire directed by the interviewer consisting of 18 questions. it is divided into two sections, the first section collects the caregiver's information and the second section collects the general information of the older adult; among the variables measured by this questionnaire are: caregiver's age, patient's age, caregiver's sex, kinship, schooling, socioeconomic status, caregiver's religion, number of children of the caregiver, hours per day dedicated to provide care, time acting as caregiver, among others.
The Zarit Caregiver Burden Scale (ESCT-Zarit) was used to measure the degree of work overload of the informal caregiver, which has been validated in several languages including Spanish and has showed a satisfactory internal consistency, with a Cronbach's alpha coefficient of 0.91 9. This assessment consists of 22 Likert-type questions with five answer choice: 1 = never, 2 = rarely, 3 = sometimes, 4 = many times, and 5 = always; with a minimum score of 22 points and a maximum score of 110 points, the higher the score, the greater the burden (work overload) on the caregiver; and classifies the caregiver with: absence of work overload ≤ 46 points; light work overload of 47-55 points and intense work overload ≥ to 56 points; the application time is eight to 10 minutes.
The Zarit Caregiver Burden Scale originally had 29 items and was designed to evaluate aspects such as physical and psychological health, economic and labor aspects, social relationships, and relationship with the patient, but it was reduced to 22 items10. It should be mentioned that there is no agreement on the number of factors that have been found on the scale, or the name of the factors; however, the following factors explain 55% of the variance: 1) impact of the care, 2) interpersonal relationships, and 3) expectations of self-efficacy 11,12. In this research, the total score obtained on the scale by each participant of the selected sample was considered to categorize the degree of work overload based on the aforementioned classification.
The analysis was carried out using the Statistical Package for the Social Sciences 22.0 Version, the internal consistency of the Zarit’s overburden scale of the caregiver was reviewed, and frequencies and percentages were obtained for the categorical variables. For the numerical variables, measures of central tendency and measures of dispersion were obtained. The Kolmogorov-Smirnov Normality Test was applied to verify the normality in the distribution of continuous variables and it was found that the distribution of the variables was not normal, so it was decided to use non-parametric statistics to be able to respond to the proposed hypothesis, Chi Square for the nominal polytomous variables and Kendall's Tau-b for the ordinal variables, and, thus, establish the association of the degree of work overload and the sociodemographic data of the caregiver.
The research was in accordance with the provisions established in the “Reglamento de la Ley General de Salud en Materia de Investigación para la Salud, México” (Regulation of the General Health Law on Health Research, Mexico) 13. The favorable opinion of the Research Ethics Committee of the Department of Nursing of the University of Sonora, registration CEI-ENFERMERIA-E-73/2018, was obtained.
RESULTS
The application of the Zarit Caregivers Burden Scale gave a satisfactory internal consistency, with a Cronbach's alpha coefficient of 0.91 (α = 0.91), and according to the classification of caregiver's work overload, most of caregivers (48.2%) presents intense work overload, 44.6% of caregivers have no work overload, and 7.2% of caregivers have a slight work overload (Table 1).
Table 1. Classification of the caregiver’s work overload; Ciudad Obregon, Sonora, 2018

Source: Zarit Caregiver Burden Scale. n = 83
Table 2 shows the association of the degree of work overload with the occupation of the caregiver. This Table shows that “homemaker” is the occupation that has a higher degree of intense work overload (25.3%) and it was determined that the perception of work overload is intimately linked to caregivers who are homemakers, with a statistically significant association (p = 0.025).
Table 2. Association of the degree of work overload with the occupation of the caregiver; Ciudad Obregon, Sonora, 2018

Source: Zarit Scale and Sociodemographic Data Sheet. n = 83
Note: X 2 = Chi-square, p= <0.05
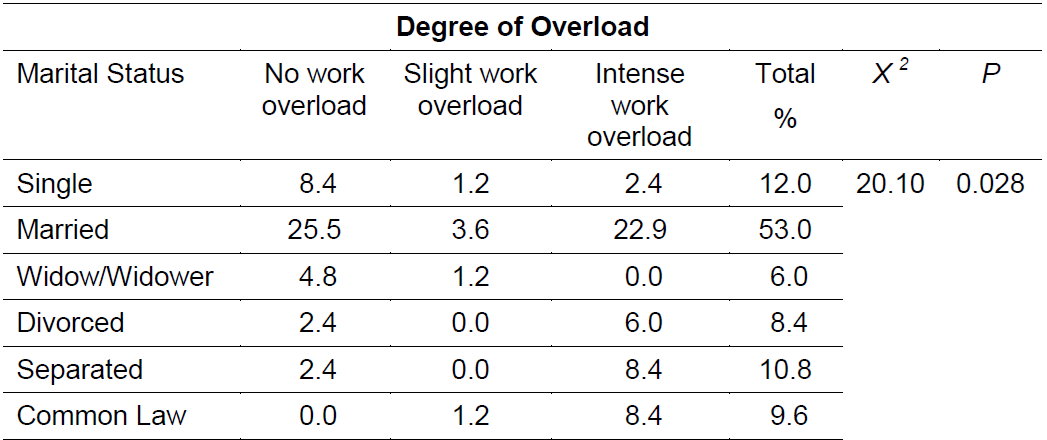
Table 3 shows the association of the degree of work overload with the caregiver’s marital status. This Table indicates that “married” is the marital status with the highest participation in the study, with 53%, a statistically significant dependence was identified between the degree of work overload and the married marital status of the caregivers (p = 0.028).
Table 3. Association of the degree of work overload with the caregiver’s marital status; Ciudad Obregon, Sonora, 2018
Source: Zarit Scale and Sociodemographic Data Sheet. n = 83
Note: X 2 = Chi-square, p= <0.05
In the association of the degree of work overload with the gender of the caregiver, it was seen that the “female” gender has a greater tendency to intense work overload (42.2%); however, it was possible to demonstrate that the degree of work overload in the caregiver is independent of his gender (p = 0.350). The association of the degree of work overload with kinship of the caregiver, showed that “son” is the kinship with more work overload (34.9%), although the work overload in the caregiver does not depend on the kinship with the older adult since it showed a significance of p = 0.575.
The religion with the largest presence in the population was “Catholic” (81.9%), which in turn was the variable that had the greatest tendency to intense work overload (38.6%); however, it was possible to identify that the degree of work overload in the caregiver is independent of its religion, since this variable did not show a statistically significant association (p = 0.900).
In the association of the degree of work overload with the caregiver’s age, a greater tendency to intense work overload was seen in the ages between 40 and 49 years (15.7%), followed by the age between 50 and 59 years (13.3%); however, it could be identified that there is no dependence between the degree of work overload and the caregiver’s age, as it does not show a statistically significant association (p = 0.168).
In the association of the degree of work overload with the degree of schooling of the caregiver, the variable that showed the greatest tendency to work overload was “completed middle school” (9.6%), followed by “completed or incomplete high school”; however, it was possible to demonstrate that the degree of work overload in the caregiver does not depend on his level of education, since the significance shown for this variable was p = 0.851.
The greatest degree of work overload occurred in those caregivers who have a monthly income between $2,700 and $6,799 pesos (26.5%); even so, no significant relationship was found between the work overload and the family income of the caregiver (p = 0.988); therefore, in this study, the monthly income is not a predictor variable of work overload in the caregivers.
In the association of the degree of work overload with the years devoted to the care of the patient, it was seen that caregivers who have care for the patient less than three years, show greater work overload (27.3%); however, there was no dependence between the degree of work overload and the time dedicated to the care of the elderly (p = 0.416). Likewise, the association of the degree of work overload with the hours per day as caregivers showed that the caregivers who show the greatest work overload are those who spend more than 17 hours a day providing care for the patient (24.1%); however, it was not possible to establish a statistically significant association for this variable (p = 0.675).
It was identified that the caregivers with the greatest tendency to work overload are those with “one to three children” (27.7%); however, it was demonstrated that the degree of work overload in the caregiver does not depend on the number of children (p = 0.361), therefore, in this study, this is not a predictor variable of work overload.
DISCUSSION
In this study, most of the caregivers showed intense work overload. This result is similar to the results reported in various national and international researches. Quantitative research has suggested a caregiver profile with more risk of work overload14,7,15.
A study conducted in Cuba by Romero, Rodriguez and Pereira 16 found the presence of work overload in 51.5% of caregivers of patients with chronic renal failure. Additionally, a study conducted in Spain by Villarejo, Zamora and Casado 17 showed the presence of work overload in 48.9% of caregivers of dependent elderly people.
The above is due to the fact that the work overload generates important changes in the personal, family, work, and social environments of the caregivers; in addition, health problems may arise due to the physical and emotional overload, and in some cases this may cause the abandonment of the role of caregiver 18. Moreover, work overload is associated to greater medical, psychiatric, and social morbidity and mortality of the caregiver 19.
The “homemaker” occupation showed a statistically significant association, since these results are similar to those reported in a study conducted in Colombia by Ortiz et al.14, which establishes that the perception of work overload is statistically significant in caregivers whose occupation is that of homemaker (p = 0.00).
When comparing the results with the literature, it was found that more than two thirds of women provide permanent care 15,7,18. This is due to the need of the elderly to have a caregiver most of the day, so that housewives are those who suffer from work overload more frequently and are more likely to have negative impacts. In theory, it can be thought that the adoption of multiple roles (besides the traditional one of a homemaker), and the difficulty in making the different tasks compatible have a direct impact on their lives.
This study shows that there is statistically significant association between the degree of work overload and the marital status, which is a similar result to the result obtained by Ortiz et al 14, where they found that there is dependence between the degree of Work overload and the marital status, and that this association is statistically significant for married caregivers (p = 0.05). Some studies 18,20 have suggested that caregivers married to the patient, the physical and emotional dependence with the spouse, the feeling of obligation to provide care, and the simultaneous attention to different roles produce conflicts and tensions in the caregiver, which with the passage of time become overload-generating factors.
Although it was not possible to demonstrate a significant relationship between the degree of work overload, the gender, and kinship of the caregiver, it was seen that the female gender and son/daughter kinship had a marked tendency towards work overload. De Valle-Alonso and collaborators7 explain that this phenomenon is due to prevailing cultural patterns in our society, which assigns to women the role of caregiver, mainly for the care of dependent people, such as children, elderly, and people with physical and mental disabilities. In addition to the foregoing, these women play other roles such as mother, wife, and daughter. Therefore, the same traditionalism and the role pressure cause the caregiver to have the tendency to work overload.
Regarding the age of the caregiver, this study did not show a statically significant association, contrary to the study carried out by Ortiz et al. 14, which found a significant association between the age of the caregiver and his degree of work overload. This study mentions that the greater the age of the caregiver, the greater the degree of work overload experienced. The literature emphasizes that the degree of work overload increases as the caregiver's age increases, while the lack of formal training and abilities of the caregiver and the co-morbidity of the patient seem to explain the aforementioned fact in general terms 20.
Although the level of schooling does not seem to be a variable statistically associated with work overload, caregivers with completed middle school showed a greater tendency to work overload. On this topic, authors such as Ortiz et al. 14 suggest that people with higher levels of education have better access to the information needed to assume their role of caregiver and use a series of coping strategies different from those used by people with lower schooling.
This study did not find a statistically significant relationship between work overload and the income of the caregiver; however, it is known that with a low income it is not possible to have the goods and services that provide comfort to the caregiver to reduce the work overload.
A study conducted in the state of Veracruz, Mexico, by Martinez, Diaz and Gomez 21 mentions that the majority of caregivers have a basic level of education, in addition to low income, since most caregivers do not work because they have the responsibility to provide care to their loved ones.
The variables studied of the caregiver profile that did not show a statistically significant relationship were schooling (p = 0.851), income (p = 0.988), kinship (p = 0.575), gender (p = 0.350), age (p = 0.168), religion (p = 0.900), caregiver’s pathology (p = 0.750), years acting as caregiver (p = 0.416), hours/day dedicated to providing care (p = 0.675), and number of children (p = 0.361). These results were similar to those obtained by De Valle-Alonso et al. 7 in a study conducted in Mexico for caregivers of elderly people, which did not find a statistically significant relationship between the caregiver’s work overload and sociodemographic characteristics such as age, gender, kinship, schooling, time as a caregiver, and hours per day dedicated to the role of caregiver. In turn, a study conducted in Chile by Flores and collaborators 15 did not find a statistically significant relationship between the caregiver’s work overload and sociodemographic characteristics such as gender, family income, and hours/day dedicated to the role of caregiver.
CONCLUSIONS
It was possible to determine the following specific profile of the informal caregiver with tendency to intense work overload: woman, homemaker, with an average age of 40 years, married, daughter of the elderly patient, low schooling, average economic income, with one to three years acting as the caregiver, dedicating more than 17 hours a day providing care, and having approximately 3 children.
There are caregivers with intense work overload, caregivers with moderate work overload, and some of them assume their caregiver role without perceiving any work overload.
In our study population we found a statistically significant association of the independent variables "occupation" and "marital status" with the dependent variable "work overload degree of the caregiver", which is why the research hypothesis is accepted.
Caregivers not only have accumulated work overload, many of them have signs of depression, stress, isolation, frustration, and are in a vulnerable position compared to the rest of the population.
Limitation for this study
One limitation is the absence of a database on informal caregivers of people with non-communicable diseases; the aforementioned database would facilitate the location of this population.
Implications for future research
This study strengthens the outreach of nursing as a social support and buffering factor of work overload in the caregiver. It confirms the need to implement a support plan for the caregiver of older adults with various pathologies that includes interventions such as education, counseling, and providing nursing care based on evidence of the needs of caregivers.
It is feasible to carry out mixed or merely qualitative studies in the studied population due to the characteristics shown during the interviews, since psychological problems that influence the care provided were identified.
REFERENCES
1. ONU. Organización de las Naciones Unidas. Informe sobre desarrollo humano. El ascenso del sur: Progreso humano en un mundo diverso. Nueva York: Programa de Naciones Unidas para el Desarrollo. 2015. Recuperado de: http://hdr.undp.org/sites/default/files/hdr_2015_overview_sp_final.pdf [ Links ]
2. Secretaria de Salud. Informe Sobre la Salud de los Mexicanos 2015. 2015. Recuperado de: https://www.gob.mx/salud/documentos/informe-sobre-la-salud-de-los-mexicanos-2015 [ Links ]
3. INEGI. Instituto Nacional de Estadística y Geografía. Mujeres y hombres en México 2017. México. 2017. Recuperado de: http://cedoc.inmujeres.gob.mx/documentos_download/MHM_2017.pdf [ Links ]
4. Cerquera Córdoba AM, Uribe Rodríguez AF, Matajira Camacho YJ, Correa Gómez HV. Dependencia funcional y dolor crónico asociados a la calidad de vida del adulto mayor. Psicogente [Internet]. 2017;20(38):398-409. Recuperado de: https://www.redalyc.org/articulo.oa?id=497555991014 [ Links ]
5. OMS. Organización Mundial de la Salud. Informe mundial sobre la diabetes. Resumen de orientación. 2016. Recuperado de: http://www.who.int/diabetes/global-report/ [ Links ]
6. Narváez Bravo ML, Martínez Martínez D. Caracterización del Síndrome de Sobre Carga del cuidador en familiares de pacientes institucionalizados y no institucionalizados con diagnóstico de Alzheimer mediante la escala Zarit. Inclusión & Desarrollo. 2015;4(1):102-107. [ Links ]
7. De Valle-Alonso MJ, Hernández-López IE, Zúñiga-Vargas ML, Martínez-Aguilera P. Sobrecarga y Burnout en cuidadores informales del adulto mayor. Enfermería Universitaria [Internet]. 2015;12(1):19-27. Recuperado de: http://www.revistas.unam.mx/index.php/reu/article/view/48065/43151 [ Links ]
8. OMENT. Observatorio Mexicano de Enfermedades No Transmisibles. Tablero de Control de Enfermedades Crónicas. 2018. Recuperado de: http://oment.uanl.mx/Tablero-de-control-de-enfermedades/ [ Links ]
9. Martín M, Salvadó I, Nadal S, Mijo LC, Rico JM, Lanz P, Taussig MI. Adaptación para nuestro medio de la Escala de Sobrecarga del Cuidador de Zarit. Revista de Gerontología [Internet]. 1996;6:338-346. Recuperado de: http://envejecimiento.csic.es/documentacion/biblioteca/registro.htm?id=3599 [ Links ]
10. Zarit S, Orr N, Zarit J. The hidden victims of Alzheimer´s disease. Families under stress. New York: University Press. 1985. [ Links ]
11. Montorio C, Izal F, López L, Sánchez C. La entrevista de carga del cuidador. Utilidad y validez del concepto de carga. An Psicol 1998:14:229-48 [ Links ]
12. Montero X, Jurado S, Valencia A, Méndez J, Mora I. Escala de carga del cuidador de Zarit: evidencia de validez en México. Psicooncología. [Internet]. 2014; 11(1): 71-85. DOI: 10.5209/rev_PSIC.2014.v11.n1.44918 [ Links ]
13. Secretaria de Salud. Reglamento de la Ley General de Salud en Materia de Investigación para la Salud. Diario Oficial de la Federación. 2014. Recuperado de: http://www.dof.gob.mx/nota_detalle.php?codigo=5339162&fecha=02/04/2014 [ Links ]
14. Ortiz Claro YG, Lindarte Clavijo AA, Jiménez Sepúlveda MA, Vega Angarita OM. Características sociodemográficas asociadas a la sobrecarga de los cuidadores de pacientes diabéticos en Cúcuta. Revista CUIDARTE [Internet]. 2013;4(1):459-466. Recuperado de: https://www.redalyc.org/articulo.oa?id=359533224005 [ Links ]
15. Flores GE, Rivas RE, Seguel PF. Nivel de sobrecarga en el desempeño del rol del cuidador familiar de adulto mayor con dependencia severa. Ciencia y Enfermería [Internet]. 2012;XVIII(1):29-41. Recuperado de: https://www.redalyc.org/articulo.oa?id=370441809004 [ Links ]
16. Romero Massa E, Rodríguez Castilla J, Pereira Díaz B. Sobrecarga y calidad de vida percibida en cuidadores familiares de pacientes renales. Rev Cubana Enfermer [Internet]. 2015;31(4). Recuperado de: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-03192015000400001&lng=es [ Links ]
17. Villarejo Aguilar L, Zamora Peña M, Casado Ponce G. Sobrecarga y dolor percibido en cuidadoras de ancianos dependientes. Enfermería Global [Internet]. 2012;11(3):159-164. Recuperado de: https://www.redalyc.org/articulo.oa?id=365834796009 [ Links ]
18. Pinzón EA, Carrillo GM. Carga del cuidado y calidad de vida en cuidadores familiares de personas con enfermedad respiratoria crónica. Rev Fac Nac Salud Pública [Internet]. 2016;34(2):193-201. Recuperado de: http://www.redalyc.org/pdf/120/12045638008.pdf [ Links ]
19. Tripodoro V, Veloso V, Llanos V. Sobrecarga del cuidador principal de pacientes en cuidados paliativos. Inst de Inv Gino Germani [Internet]. 2015;17:307-330. Recuperado de: https://publicaciones.sociales.uba.ar/index.php/argumentos/article/view/1324/1216 [ Links ]
20. Pérez Perdomo M, Llibre Rodríguez JJ. Características sociodemográficas y nivel de sobrecarga de cuidadores de ancianos con Enfermedad de Alzheimer. Revista Cubana de Enfermería [Internet]. 2010;26(3):110-122. Recuperado de: http://scielo.sld.cu/pdf/enf/v26n3/enf04310.pdf [ Links ]
21. Martínez Ruiz EC, Díaz Vega FE, Gómez Blanco EI. Sobrecarga del cuidador primario que asiste a un familiar con cáncer. Altepepaktli. 2010;6(11): 32-41. Recuperado de: http://132.248.9.34/hevila/Altepepaktli/2010/vol6/no11/4.pdf [ Links ]
Received: February 01, 2019; Accepted: March 11, 2019
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
