










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.19 n.57 Murcia Jan. 2020 Epub Mar 16, 2020
https://dx.doi.org/eglobal.19.1.380441
Originals
Incidences and Causes of Surgery Cancellation in a University Hospital in Barranquilla, Colombia, in 2016
1Universidad Simón Bolívar, Barranquilla, Colombia.
2Anesthesiology and Intensive Care Service, Hospital Povisa, Vigo, Spain.
Introduction
Surgery is any procedure performed in the operating room that allows timely treatment of pathologies and injuries; in Colombia, an indicator of the quality of the information system is the proportion of scheduled surgery cancellations.
Materials and method
We designed a retrospective observational study, selecting all patients scheduled for surgery at the hospital institution from January 1, 2016 to December 31, 2016. A total of 3207 patients were included. We analyzed cases of surgery cancellations because of factors attributable to the patient, institution, and medical order.
Results
Of the 3207 scheduled procedures, 1739 (54.2%) were men and 1468 (45.8%) were women. Surgical procedures were scheduled for patients aged between 6 months and 116 years, with an average age of 38 years. Of the scheduled procedures, 244 (7.6%) surgeries were cancelled. The months with the lowest and highest incidences of surgery cancellation were August and November, with 9 (3.7%) and 36 (14.8%) cancellations, respectively. The cancellation rate for surgical specialties independently ranged from 1 (0.4%) for gynecology specialties of oncology, maxillofacial, and urology and 85 (34.8%) for orthopedics.
As the causes of cancellation, 93 (38.1%) were attributable to the institution, 99 (40.6) to patients, and 52 (21.3%) to medical orders.
Conclusions
In total, 41% of cancellations could have been avoided. We recommend continuous monitoring of scheduled patients, as well as the dissemination of our findings to professionals for the empowerment of responsibilities and the need for education for patients undergoing intervention.
Key words: Surgery; Surgical suspension; Causes of cancellation
INTRODUCTION
Patient safety is currently a worldwide public health concern. According to data from the World Health Organization (WHO), 1 in 300 patients suffers from harm caused by medical care compared with the likelihood of a passenger suffering harm on an airplane, which is one in every million passengers 1.
The cancellation of scheduled surgeries is classified as one of the unsafe healthcare practices that can lead to adverse events, specifically including those factors related to resource management, such as lack of surgical supplies or equipment, lack of sterile clothing, or staff shortage. As emergency surgery replacement can also be provided2, WHO emphasizes that approximately 230 million major surgical procedures are performed worldwide every year, and it is estimated that investments in the surgical department make up 30.1% of the hospital’s budget 3. Therefore, the cancellation of scheduled surgeries affects and determines the budgetary, labor, and medico-legal conflicts in the institution, thereby increasing costs and having a negative impact on patient care, particularly to those belonging to the most underprivileged section of the population 4. As a result, the service and its impact must be organized and optimized5.
In Colombia, Law 100 of 1993 established the General System of Social Security in Health (SGSSS) in order to declare health as a social right through the promotion, prevention, diagnosis, treatment, and rehabilitation of individuals who access the health system services. The first quality indicator for healthcare presented by the SGSSS in 2007 was the cancellation of scheduled surgeries, which represented a rate of 7.7% 6.
The Integrated System of Information in Health and Social Protection, in its quality indicators of Resolution 0256 of 2016, showed an indicator of surgery cancellation which, within the periods 2016-1 and 2016-2, showed an average of 3.62 and 0.92, respectively, at a national level; however, there are only reports from four institutions7.
According to the report from the Observatory for National Health Care Quality, the trend of the indicator for cancellation of scheduled surgeries showed a decrease of 1.8%, from 8.7% in the second half of 2006 to 6.9% in the first half of 2009 8. It is estimated that approximately 60% of elective surgical cancellations were potentially avoidable if improved techniques were used 9.
Avoiding factors that lead to surgery cancellations obliges institutions to commit themselves to reduce those agents that affect pre-surgery arrangements, which may generate additional healthcare costs, costs derived from internal or external failures, and prevention and analysis costs. To achieve excellence, institutions must prove their efficiency and quality via continuous improvement, which results in a relationship of trust between the patient and institution as a result of the optimization of resources and extra work needed for the preparation of operating rooms 9-11.
The objective of this research was to analyze the causes behind scheduled surgery cancellations in the university institution to allow surgeons, anesthesiologists, surgical instrument technicians, nurses, and administrators to introduce suitable measures to reduce the department’s cancellation rate.
MATERIAL AND METHODS
We designed an observational study with a retrospective database. All patients scheduled for surgery at the University Hospital between January 1, 2016 and December 31, 2016, were included, with a total of 3207 patients.
A secondary data source of surgical planning was completed by the head of the institution’s surgery department. For the study, sociodemographic variables (sex and age), and surgical procedure (scheduled month, surgical specialty, completion or cancellation of the procedure, and reason for cancellation) were evaluated.
This is a level 4 healthcare institution with surgical specialties and cutting-edge technology and infrastructure, with seven operating rooms for the development of scheduling, with interdisciplinary talent and anesthesia, cardiovascular, general surgery, oncology, pediatrics, plastic surgery, dermatology, gynecology, maxillofacial, nephrology, pneumology, ophthalmology, otorhinolaryngology, orthopedics, and urology specialties.
The surgical schedule is prepared on a daily basis at 5:00 pm for due organization and planning, and it is delivered to the department for the preparation of the hospitalized patient; for outpatients, surgeries are confirmed by telephone the day before surgery.
Cancellation is defined as any scheduled surgical intervention that is not performed (scheduled and unperformed surgery)
The reasons for surgery cancellation were classified into three groups:
Failure of the institution: lack of authorizations by the Health Promoting Agencies (EPS), unavailable medical equipment, unavailable supplies, incomplete preoperative processes
Patient’s reasons: rejection of the intervention, patient’s non-attendance
Medical decision: health status, acute intercurrent illness
The data were analyzed in Microsoft Excel for statistical significance with a bivariate analysis using the Chi-square test and the statistical software SPSS, version 22.
RESULTS
Of the 3207 procedures scheduled, 1739 (54.2%) were surgeries for men and 1468 (45.8%) were for women. Surgical procedures were scheduled for patients aged between 6 months and 116 years old, with an average age of 38 years (standard deviation, 24).
Of the total scheduled interventions, 244 (7.6%) ended up being cancelled. The months with the lowest and highest incidences of cancellations were August and November, with 9 (3.7%) and 36 (14.8%) cancellations, respectively. Analysis of the distribution of surgical procedures performed and cancelled per month revealed statistically significant differences (chi-square = 58.71; p < 0.000) (Table 1).

Analysis of the surgical specialties independently revealed varying cancellation rates, ranging from 1 (0.4%) for the oncology, gynecology, maxillofacial, and urology specialties and 85 (34.8%) for the orthopedics specialty. Analysis of the distribution of surgical procedures performed and cancelled by surgical specialty revealed statistically significant differences (chi-square = 534.93; p < 0.000) (Table 2).

Among the reasons for surgery cancellation attributable to the institution, we found 93 (38.1%) cases in which the most common reasons were incapacity by the specialist, damaged equipment such as an image intensifier, bed unavailability in the intensive care unit, lack of hospital supplies for the procedure, and delay in the surgery schedule (Table 3).
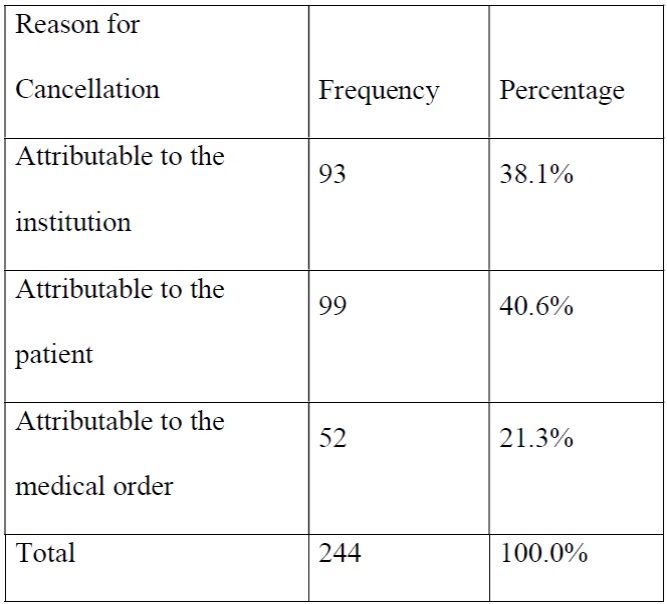
When reviewing the cancellation causes attributable to patients, we found 99 (40.6%) cases in which the patient’s non-attendance and unsigned consent were very common.
Cancellation causes attributable to medical orders accounted for 52 of cases (21.3%), including cases of patients with high blood pressure, fever, vomiting, diarrhea, hyperglycemia, hypertension, and a patient who died before surgery.
The high cancellation rate of 28% (n = 70) in orthopedics was due to the absence or incompleteness of material.
When classifying cancellation causes into three groups based on the possible prevention thereof, we found that 101 (41%) cases of cancellation could be avoided with the participation of the institution, professionals, and external agents.
DISCUSSION
Surgery cancellation is a public health issue because of its impact both on the institutions’ economy and on patients’ psychological status. Various institutions, such as the Modernization Agency of the National Health Service 8, after an analysis of the causes, have issued recommendations regarding measures aimed at correcting surgery cancellation.
In a study conducted at the CMA 9, the primary cause for cancellation was the incorrect selection or preparation of the patient, which accounted for 27.1% of cases. Our study showed factors attributable to the institution resulting from doctors’ incapacities, lack of supplies, and equipment damage. In 2013, 7.6% of cases were cancelled worldwide, and the three most frequent reasons for cancellation were those related to patients, facilities, and inadequate treatment 10.
A retrospective analysis of 8 years at an institution resulted in a reasonable cancellation rate of 3.66% within the world average 11, while our cancellation rate was 7.6%. However, the study classified cancellations into those attributable to the patient, administrative, and medical causes, with a percentage of 26.8% for those attributable to administrative causes; while ours was 38.1%.
Administrative factors that were considered to be the main cause of surgery cancellations are indicative of the need to improve the organization and planning in this institution, and in the present study, those processes related to orthopedic procedures, which were the interventions that presented the highest rate of cancellation 12.
November and December showed the highest and lowest cancellation rates, respectively 13; in Brazil, surgery cancellation was 7.6%, with the lowest rate in December (4.3%), and the highest rate recorded in November (11.1%) 14. At our institution, November recorded the highest rate, while the lowest rate was recorded in August.
A study conducted in Australia showed 51 procedures cancelled on the day of surgery, in which 14.3% were due to the lack of surgical aptitude, followed by inadequate surgical time 15. However, in institutions that make a preoperative call 2 days before surgery and a weekly review of the surgery schedule, the cancellation rate was reduced from 3.8% to 3.5%. This strategy could improve the cancellation rate in the institutions of the region, thereby improving the surgical cancellation indicator. Cancellations related to the patient were reduced from 81% to 79.7%, while those attributable to the hospital were reduced from 17.5% to 15.9% 16.
During a period of 2 months across 13 specialties, a qualitative and prospective analysis was performed, which showed that cancellations occurred before the day of surgery and occurred because patients’ health status was not optimal for the scheduled surgery or due to the lack of organizational resources 17, a situation in the present study in which the factors were associated with the patient and administrative procedures.
An analysis of the efficiency of operating rooms conducted a measurement of procedures with indicators of surgery onset on time, percentage of cancellations, and average number of patients per day; these are indicators that refer to the quality of service. In the present study, although only the incidence of cancellation and causes17 were assessed, it is advisable to investigate the efficiency, costs, surgical times, and profitability of surgery services because, in addition to providing health services to the population, it is a profitable business.
Instead of applying the instrument to professionals, the results determined that 83% of the population surveyed had noticed the cancellation of surgeries in the departments; approximately 50% attended the surgery department and 33% in hospitalization. Other reasons for cancellation were 44% because of the institution’s administrative staff, 12% because of the lack of interdisciplinary team management, 28% because of poor medical management, and 16% because of poor nursing management 3.
CONCLUSIONS
This study showed that the surgical cancellation rate of the hospital institution in 2016 was 7.6%. Regarding the causes for cancellation, the most frequent reasons were related to the specialty of orthopedics (34.8%), and those attributable to the patient accounted for 40.6%.
In total, 41% of cancellations could have been avoided by providing education to the patient and suitably planning procedures in which specialized surgical medical supplies are needed.
The results in this research indicate the need to provide training programs addressed to healthcare professionals who are a part of this process so that proper measures can be taken to improve the quality of the service, in addition to being a reference at the local level because such a study has not been conducted before.
We suggest conducting studies that address this issue in the city, department, and country, as well as the efficiency of the measures taken to reduce this quality indicator in health institutions.
REFERENCIAS
1. OMS, 10 datos sobre seguridad del paciente. WHO [Internet]. 2018 [cited 2018 Jul 18]; Available from: http://www.who.int/features/factfiles/patient_safety/es/ [ Links ]
2. Zenewton André da Silva Gama, Adriana Catarina de Souza Oliveira, Pedro Jesus Saturno Hernández. Cultura de seguridad del paciente y factores asociados en una red de hospitales públicos españoles. 2013 [cited 2018 Jul 18]; Available from: http://www.scielo.br/pdf/csp/v29n2/15.pdf [ Links ]
3. Gaviria-García G, Lastre-Amell G, Suárez-Villa M. Causas que inciden en cancelación de cirugías desde la percepción del personal de salud. Enfermería Univ [Internet]. 2015 [cited 2018 Jul 16];11(2):47-51. Available from: http://www.elsevier.es/ [ Links ]
4. Barbosa MH, Miranda Goulart DM, Vieira de Andrade E, De Mattia AL. Análisis de la suspensión de cirugía en un hospital docente. Enferm Glob [Internet]. 2012 [cited 2018 Apr 19];11(2):164-73. Available from: http://scielo.isciii.es/pdf/eg/v11n26/administracion2.pdf [ Links ]
5. Gómez-Ríos MA, Abad-Gurumeta A, Casans-Francés R, Calvo-Vecino JM. Claves para optimizar la eficiencia de un bloque quirúrgico. Rev Esp Anestesiol Reanim [Internet]. 2019 Feb 1 [cited 2019 Apr 9];66(2):104-12. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0034935618301440 [ Links ]
6. 1er Informe Nacional de Calidad de la Atención en Salud [Internet]. 2009 [cited 2018 Jul 18]. Available from: http://www.minproteccionsocial.gov.co [ Links ]
7. Ministerio de Salud. Indicadores de Calidad Resolución 256/16 [Internet]. [cited 2018 Jul 18]. Available from: http://oncalidadsalud.minsalud.gov.co/Paginas/Indicadores.aspx [ Links ]
8. National Health Service (NHS) Modernisation Agency Eurofound [Internet]. [cited 2019 Apr 9]. Available from: https://www.eurofound.europa.eu/observatories/emcc/erm/factsheets/national-health-service-nhs-modernisation-agency [ Links ]
9. Guillén JM, Bernadó AJ, Solanas JAG, Guedea ME, Villahoz ER, Díez MM. Cancelación en CMA: Incidencia y causas. Cirugía Española [Internet]. 2012 Aug 1 [cited 2019 Apr 9];90(7):429-33. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0009739X11002491 [ Links ]
10. Dhafar KO, Ulmalki MA, Felemban MA, Mahfouz ME, Baljoon MJ, Gazzaz ZJ, et al. Cancellation of operations in Saudi Arabian hospitals: Frequency, reasons and suggestions for improvements. Pakistan J Med Sci. 2015; [ Links ]
11. Broullón Dobarro A, Cabadas Avión R, Leal Ruiloba MS, Vázquez Lima A, Ojea Cendón M, Fernández García N, et al. Análisis retrospectivo de las suspensiones quirúrgicas y de los factores influyentes durante 8 años. Cirugía Española [Internet]. 2019 Apr 1 [cited 2019 Apr 9];97(4):213-21. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0009739X19300077 [ Links ]
12. Andrea Velásquez-Restrepo P, Karina Rodríguez-Quintero A, Sebastián Jaén-Posada J. Aproximación metodológica a la planificación y a la programación de las salas de cirugía: una revisión de la literatura Methodological approach to the planning and scheduling of operating rooms: a literature review Aproximação metodológica à planificação e programação das salas de cirurgia: revisão de literatura [Internet]. Rev Gerenc Polit Salud 2010 [cited 2019 Apr 9]. Available from: http://www.scielo.org.co/pdf/rgps/v12n24/v12n24a15.pdf [ Links ]
13. Abeldaño RA, Coca SM. Tasas y causas de suspensión de cirugías en un hospital público durante el año 2014. Enfermería Univ [Internet]. 2016 Apr 1 [cited 2019 Apr 9];13(2):107-13. Available from: http://www.revista-enfermeria.unam.mx/ojs/index.php/enfermeriauniversitaria/article/view/93 [ Links ]
14. Keller A, Ashrafi A, Ali A. Causes of elective surgery cancellation and theatre throughput efficiency in an Australian urology unit. F1000 Research 2014;3:197 [ Links ]
15. Al Talalwah N, McIltrot KH, Al Ghamdi A. Elective Surgical Cancellations in a Tertiary Hospital in the Middle East: Quality Improvement Process. J PeriAnesthesia Nurs [Internet]. 2019 Apr 1 [cited 2019 Apr 11];34(2):310-21. Available from: https://www.sciencedirect.com/science/article/pii/S1089947218301448 [ Links ]
16. Turunen E, Miettinen M, Setälä L V-JK. Elective Surgery Cancellations During the Time Between Scheduling and Operation. J Perianesth Nurs [Internet]. 2019;34:97-107. Available from: https://ezproxy.unisimon.edu.co:2126/record/display.uri?eid=2-s2.0-85045553765&origin=resultslist&sort=plf-f&src=s&st1=%22surgery+cancellation%22&st2=&sid=07895ca8b3832a547da62ebc64b2f954&sot=b&sdt=b&sl=37&s=TITLE-ABS-KEY%28%22surgery+cancellation%22%29&relpos=1&citeCnt=0&searchTerm= [ Links ]
17. Córdoba S, Caballero I, Navalón R, Martínez-Sánchez D, Martínez-Morán C, Borbujo J. Analysis of Operating Room Activities in the Dermatology Department at Hospital Universitario de Fuenlabrada (2005-2010). Actas Dermo-Sifiliográficas, English Ed [Internet]. 2013 Jan 1 [cited 2019 Apr 9];104(1):38-43. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1578219012003551 [ Links ]
Received: May 23, 2019; Accepted: September 18, 2019
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
