










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.19 n.58 Murcia Apr. 2020 Epub May 18, 2020
https://dx.doi.org/eglobal.392231
Originals
Women with high level of education, victims of the care of people with Alzheimer's
1aInstituto Maimónides de Investigación Biomédica de Córdoba. España.
1bUniversidad de Córdoba. España.
1cHospital Universitario Reina Sofía de Córdoba. España.
2Universidad de Castilla la Mancha. Toledo. España.
3Clinica Medica Unit and Center for Studies on Gender Medicine, Universidad de Ferrara. Italia.
The aim of this job is to know the existing relationship between the task of caring patients with Alzheimer's disease, caregivers' gender and their level of academic studies. Descriptive study, 69 persons diagnosed with Alzheimer's disease and their respective familiar caregivers as subjects of the study. Age, gender, academic level, burden, depression, anxiety level, quality of life and social loneliness have been measured in caregivers. Age, gender, dependency level and neuropsychological state have been measured in patients. Data collection was done in 2016. Logistic regression analysis was performed. Caregivers with high levels of academic studies suffer more burden, being women in their majority. They are more likely to present social loneliness and higher levels of anxiety and a worse quality of life than men. The burden may be due to a greater number of responsibilities to respond to, and to the inability to combine it with the role of caregiver. We can conclude that women become victims of caring Alzheimer' patients.
Key words: Alzheimer's disease; Academic studies; Burden; Family caregivers; Gender
INTRODUCTION
Alzheimer's disease is the most common type of dementia, affecting a wide range of people with dementia1, from 204.13 in Israel to 15.51 in India by 1000 persons; in Spain 39.03. In Spain the incidence is 1.4 by 1,000 persons/year from 65 years2.It is a disease for which there is no curative treatment, and whose symptoms and functional damages are aggravated as it progress. Alzheimer's disease is characterized by its chronicity, dependency status, presence of neuropsychiatric disorders and the deterioration of memory and cognitive skills that accompany it, such as speaking coherently, recognize or identify objects, etc. 3.
The increase in the prevalence of chronic diseases, including Alzheimer's disease, is caused as a result of the population aging that is being experienced nowadays. The increase in the number of elderly people in situation of dependency implies an increase in care needs, and therefore in caregivers to provide them. This role is very often assume by family, being denominated informal or familiar caregiver, the family member who carries out the task of caring.
Informal cares are the 80% of all long-term care in Europe4. Informal care that usually is provided by women4
Familiar caregivers of people with Alzheimer's disease face high levels of dependence of their relatives, inability to perform basic and instrumental activities of daily living, and in addition neuropsychiatric disorders and behavioral problems of the patient5.
These caregivers, often referred to as "hidden or unknown patients," are at increased risk for anxiety, depression, sleep disorders, reduced quality of life, increased cardiovascular morbidity, increased mortality, etc…; therefore, they can be considered as a population at risk, susceptible to suffer both physical and mental illness6. Furthermore, familiar caregivers spend most of their time to perform the role of caregiver7, what causes changes that may affect their physical and psychological health, as well as their family and social life.
Impact of caring is influenced by both objective and subjective components8. Objective components as the dedication and the performance of the caregiver role; and subjective components that are related to how the situation is perceived and, in particular, they are related to the caregiver emotional response to the experience of caring. There is some relationship between gender and subjective burden8.
Functional impairment of patients with Alzheimer's disease is one of the main problems that directly affect the quality of life of familiar caregivers9 10 11 12 13 14-15On the other hand, there are studies that indicate that non-pharmacological intervention programs in Alzheimer's patients have a positive effect on both, them and their caregivers16In this line the day care centers are presented as a solution to reduce the caregiver burden and help family caregivers to cope with demands17
Moreover, it has also been seen that the coping strategies used by familiar caregivers determine their high levels of burden, anxiety and depression, as in the studies of García-Alberca et al.18and of Iavarone et al.19, in which they observed higher levels of anxiety and depression in those caregivers that did not use suiTable coping strategies (decision making, coping with behavioral problems, etc.). Something similar was concluded in the study conducted by Cheng et al.12, in which they found that the self-efficacy of the caregiver to face problems related to care was associated with lower levels of burden. Therefore, it can be said that there is a relationship between how to address the different situations that arise from the task of caring and the quality of life that caregivers present, understood that as the level of burden, anxiety and depression they experience.
Additionally, sociodemographic characteristics of caregivers influence their quality of life, level of burden, anxiety, depression, etc20, type of diagnosis 21the kinship that keeps with the person cared14, the time they dedicate to the task of caring22, etc. have been related to the appearance of these pathologies in caregivers.
With that background, the research group wanted to know the existing relationship between the task of caring for patients with Alzheimer's disease, caregivers' gender and their level of academic studies, since care has become a gender issue and women are traditionally in charge of relatives care.
METHODS
Design
Descriptive study, with two related groups: caregivers and their relatives suffering Alzheimer's disease. The Theoretical Framework is Women's Health.
Inclusion and exclusion criteria
Inclusion criteria were patients diagnosed with Alzheimer's disease and their respective familiar caregivers; caregivers with at least 6 months dedicated to care and patients and caregivers belonging to a province of the south of Spain. Exclusion criteria were patients undiagnosed of Alzheimer's disease or diagnosed with other dementias; independent patients or with low dependence to perform basic activities of daily living (score > 90 on Barthel Index); formal caregivers or those who received some material compensation for the work they developed; caregivers who had been playing the role of caregiver for a short period of time (less of 6 months); and patients or caregivers with difficulty to understand local language.
Sample and setting
Accepting an alpha error of 0.95 for an accuracy of +/- 0.11 units in a bilateral contrast for an estimated proportion of 0.3412, a random sample of 72 patients with their respective caregivers was required assuming that the population of Alzheimer's patients in the city, reference of the study in Spain, is 8000 (in 2016). A replacement rate of 1% has been estimated. One was a formal caregiver and two did not response, so finally, a random sample of 69 patients with their caregivers, other 69 people, was gathered.
Variables
To assess the state of caregivers and patients, the next variables were taken into account: In caregivers ( sociodemographic characteristics such as age, gender, academic level, between others; level of burden, depression, anxiety, quality of life, social loneliness and level of dependence. In patients ( neuropsychological state, level of dependence for basic activities of daily living and sociodemographic characteristics (age, duration of dementia, etc…).
Measure instruments
Sociodemographic questionnaire: Of caregivers: age, gender, kinship, level of studies, time being caregiver and patient-caregiver coexistence. Of patients: age, gender, kinship, time with the diagnosis of dementia. Zarit Burden Interview:To measure caregiver burden23. Beck Depression Inventory:To measure level of depression of caregivers24. Beck Anxiety Inventory:To measure level of anxiety of caregivers25. SF-36:To measure caregiver quality of life26. ESTE-II Scale:To measure social loneliness of caregivers27. Pfeiffer test:To measure caregivers cognitive state28. Barthel Index:This instrument was applied to Alzheimer's disease patients. It is a 10-item scale used to measure performance in basic activities of daily living29. Mini-Mental State Examination:To measure patient's cognitive state30.
Data collection
Selection of participants by a treatment group of patients with Alzheimer's disease, composed by: Psychologist, Social Worker, Physiotherapist, Occupational Therapist and Nurse. To communicate to potential participants that they have been selected for a study because of their condition of familiar caregivers of people with Alzheimer's disease. To explain what the study consisted of and, if they wanted to participate, quote them for a personal interview. Checking that they fulfilled inclusion and exclusion criteria, and resolution of possible doubts. To provide the information sheet and the informed consent to caregivers and patients (or legal guardians in default).To collect sociodemographic information of the participants and to manage the instruments of data collection.
Ethical considerations
All participants (or legal guardians in default), signed an informed consent by which they accepted their participation in the study. The proposed research respects the fundamental principles of the Declaration of Helsinki, the Council of Europe on Human Rights and Biomedicine, the UNESCO Universal Declaration on the Human Genome and Human Rights and the Oviedo Council on Human Rights and Biomedicine. The project has the approval of the Ethics Committee (reference 2949).
Data analysis
Results have been analyzed using the program SPSS Statistics version 22 (IBM Corp, Armonk, NY, USA) for statistical analysis, licensed to the University of Castilla La Mancha (Spain). Qualitative variables were described as count and percentages, while quantitative were summarized with mean and standard error of the mean. Variables were related using chi-square test in the case of qualitative ones, and variance analysis of quantitative data. For statistical significance it has been considered a p<.05. For significant differences between groups the analysis of variance of a factor and multifactorial with post-hoc of Student-Newman-Keuls multiple comparisons adjustment were carried out. On hypothesis contrast, the normality of the sample was verified by the Shapiro-Wilk test, being significant if p<.05, which assumes that the samples do not follow a normal distribution. Because of this, non-parametric tests were used: the “U” of Mann-Whitney and the Kruskal-Wallis test according to the grouping variable. If the Shapiro-Wilk test was not significant, normal sample distributions were assumed and parametric tests were used: Student's T-test or ANOVA of one factor depending on the clustering variable. In making predictions between variables logistic regression analysis were performed.
RESULTS
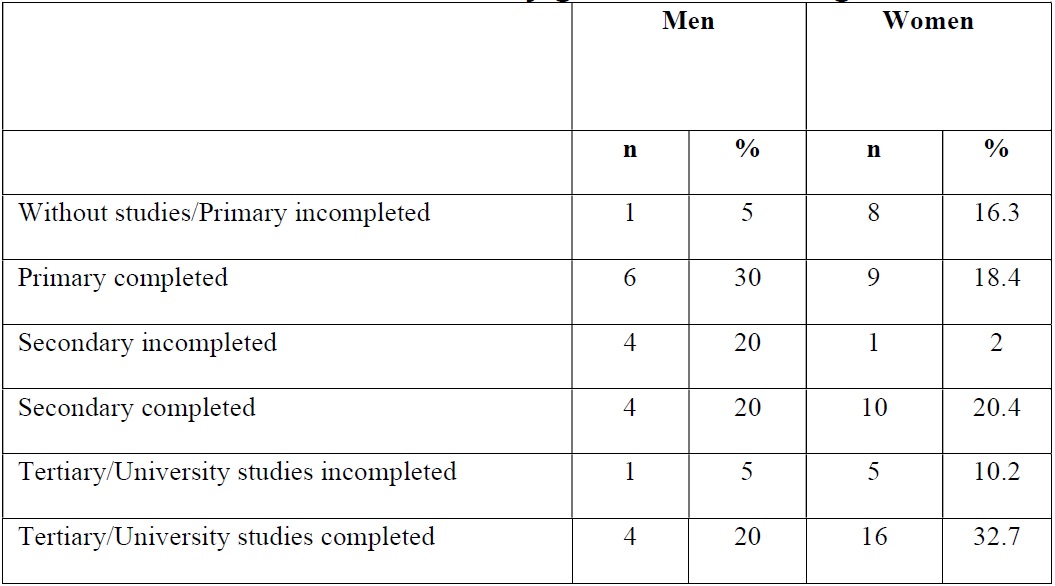
As shown in Table 1, 69 familiar caregivers were recruited, from which 49 (71%) were women and 20 (29%) were men. They had a mean age of 58.77 ± 11.23 years old. Most of caregivers, 43 (62.3%), were sons or daughters of the person cared, and 45 (65.2%) lived with the person they cared. Familiar caregivers had been caring a mean of 6.59 ± 6.16 years. Regarding to the educational level, most part of caregivers, 29% of them, had completed tertiary education (32.7% of the women and 20% of the men had that educational level).
Table 1. Sociodemographic Characteristics of 69 Caregivers
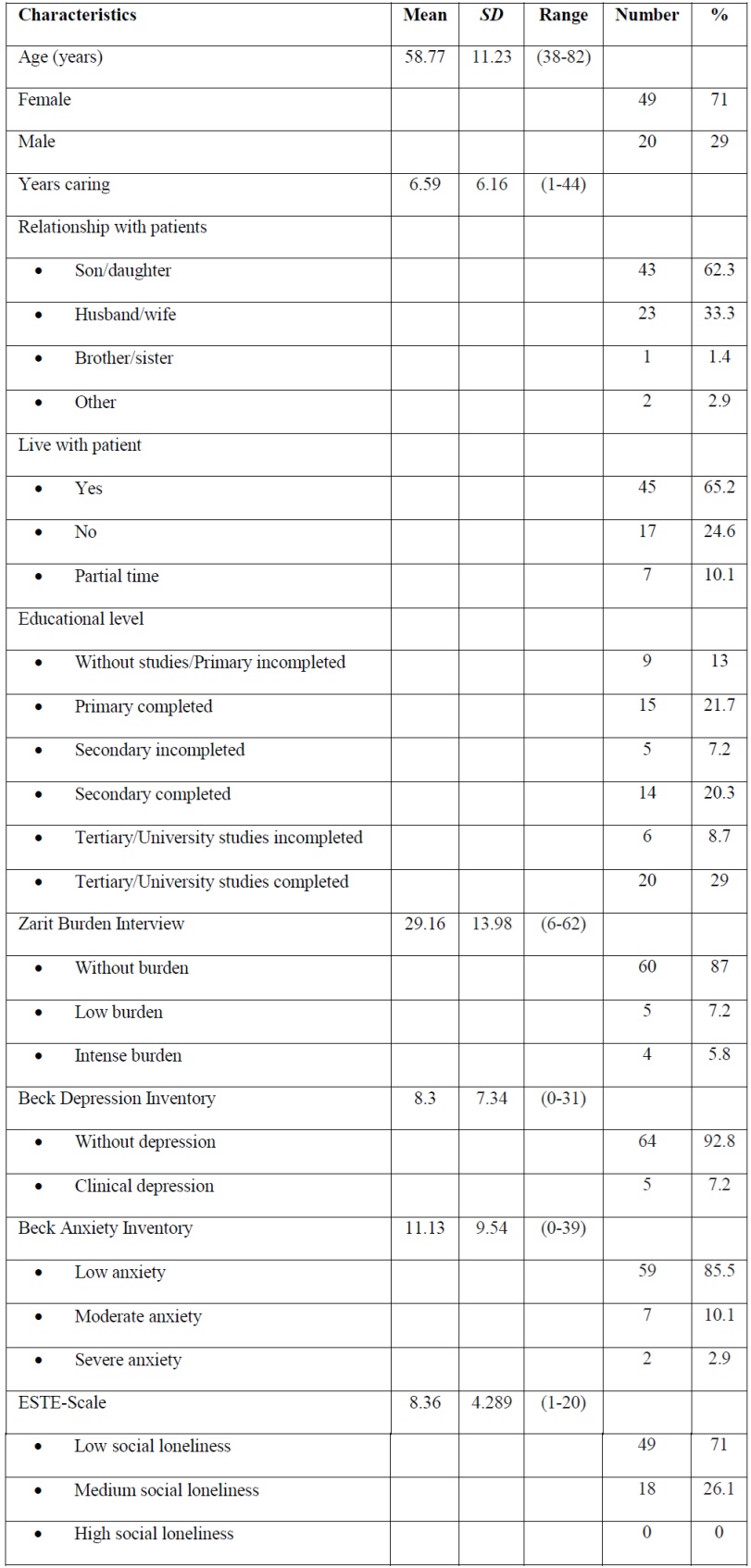
Note: SD=Standard Deviation. %=Percentage
The level of academic studies stratified by caregiver gender can be seen in Table 2. Familiar caregivers of people with Alzheimer's disease had a mean burden of 29.16 ± 13.98; a mean anxiety of 11.13 ± 9.54 and a mean depression of 8.3 ± 7.34. The average social loneliness was of 8.36 ± 4.289 points.
As shown in Table 3, patients had a mean age of 79.83 ± 7.93 years old. From the 69 included on the study, 21 (30.4%) were men, while 48 (69.6%) were women. 43,5% of the patients had been diagnosed of Alzheimer's disease between 1 and 5 years ago. 28 (40.6%) patients had a total dependence to perform basic activities of daily living, and 41 (59.4%) had a severe cognitive impairment.
Table 3. Characteristics of 69 Alzheimer's disease Patients

Note: SD=Standard Deviation. %=Percentage
On hypothesis contrast, using caregiver burden as dependent variable, it has been found that statistically significant differences exist between educational levels, when comparing caregivers burden between groups “without studies/primary uncompleted” [23.33 (SD 10.27)], and “tertiary/university studies completed” [33.25 (SD 11.34)] (p=.03). Also, between groups “primary completed” [22 (SD 11.86)], and “tertiary/university studies completed” [33.25 (SD 11.34)] (p<.001). It can be said that caregivers with high level of studies suffer more burden and, as it has been seen, the majority of caregivers with this level of studies were women. Results obtained on hypothesis contrast are shown in Table 4.

Additionally, there are statistically significant differences on caregivers burden when comparing caregivers with depression [52.4 (SD 8.74)], and without depression [27.34 (SD 12.64)] (p<.001). So there is more burden when the caregiver also suffers depression (Table 4).
Moreover, when comparing burden of caregivers of patients with moderate dependence [25.43 (SD 12.88)], and burden of caregivers of patients with severe dependence [35.65 (SD 12.15)], there have been found statistically significant differences, so the burden is higher when the level of dependence is higher (p=.018). But when comparing burden between caregivers of patients with severe dependence [35.65 (SD 12.15)] and caregivers of patients with total dependence [27.39 (SD 14.55)], it was found that caregivers suffered more burden when the level of dependence of patients was lower (p=.016) (Table 4).
When stratifying data according to gender of the caregiver, we found statistically significant differences in anxiety levels and in quality of life levels. In terms of anxiety level, women [12.73 (SD 9.73)] had higher levels than men [7 (SD 7.83)] (p=.013). With regard to the level of quality of life, women presented lower quality of life than men in the items vitality (p=.012), social function (p=.028) and emotional role (p=.048) (Table 4).
Focusing on social loneliness, there are higher social loneliness in those caregivers who live with the patient against those who do not (p=.045). This social loneliness is higher when they live always together than when it is for seasons (p=.041). It has been also found a relationship between social loneliness and caregivers' age. Caregivers with medium social loneliness have higher ages than those with low social loneliness (p<.001), increasing social loneliness scale as caregiver's age increased. Furthermore, caregivers who have depression feel higher social loneliness that those who do not have depression (p=.039) (Table 4).
Moreover, when comparing burden of caregivers of patients with moderate dependence [25.43 (SD 12.88)], and burden of caregivers of patients with severe dependence [35.65 (SD 12.15)], there have been found statistically significant differences, so the burden is higher when the level of dependence is higher (p=.018). But when comparing burden between caregivers of patients with severe dependence [35.65 (SD 12.15)] and caregivers of patients with total dependence [27.39 (SD 14.55)], it was found that caregivers suffered more burden when the level of dependence of patients was lower (p=.016) (Table 4).
When stratifying data according to gender of the caregiver, we found statistically significant differences in anxiety levels and in quality of life levels. In terms of anxiety level, women [12.73 (SD 9.73)] had higher levels than men [7 (SD 7.83)] (p=.013). With regard to the level of quality of life, women presented lower quality of life than men in the items vitality (p=.012), social function (p=.028) and emotional role (p=.048) (Table 4).
Focusing on social loneliness, there are higher social loneliness in those caregivers who live with the patient against those who do not (p=.045). This social loneliness is higher when they live always together than when it is for seasons (p=.041). It has been also found a relationship between social loneliness and caregivers' age. Caregivers with medium social loneliness have higher ages than those with low social loneliness (p<.001), increasing social loneliness scale as caregiver's age increased. Furthermore, caregivers who have depression feel higher social loneliness that those who do not have depression (p=.039) (Table 4).
A logistic regression was performed to relate the variables associated with social loneliness, with women being 8.1 times more likely (95% CI = 1.23-53.45) to present social loneliness than men (p=.03). In addition, for each year of age of the caregiver, the probability of suffering social loneliness increased in 1.08 (95% CI = 1.01-1.16) (p=.028). Finally, people with mild burden were 105 times more likely to suffer social loneliness (95% CI = 4.39-2585) than those without burden (p=.004). Logistic regression results are shown in Table 5.

DISCUSSION
The majority of caregivers included in this study are women (71%), which is certainly the most predominant feature among these caregivers, confirming the female sex as a defining feature of them, which is possibly due to the cultural conception that caring is a function attached to women as part of their gender role. Other studies show such predominance of female sex over male sex11 31 32
In this study, significant associations were identified between caregiver's gender and affectations such as their anxiety level and their quality of life, being the level of anxiety higher among women, as in the study of García-Alberca et al.18, whereas the level of quality of life was higher in men (in the items of vitality, social function and emotional role). We also detected an association between the female gender of caregivers and their level of social loneliness, although no other studies have been found that reflect such association.
The age of these caregivers also appears to be well defined, being medium or high ages in the majority of studies. Age influences the caregiver's experience of care, as we found, caregivers' social loneliness increased as their age did. Dalpai et al.33report that greater age has relation with higher care burden, lower quality of life and more frequent depression in informal caregivers.
In the present study, high levels of academic studies have been detected among caregivers, which is not usually when comparing to the characteristics of familiar caregivers in Spain. For example, in the study carried out by Toribio-Díaz et al.34, only 10,8% of principal caregivers had university studies. As seen in the results, having a high level of studies implies an increase in the level of burden of caregivers, which may be due to a greater number of responsibilities to respond to, and to the inability to combine it with the role of caregiver.
Relationship with patients is also a defining characteristic of familiar caregivers, who are very often sons/daughters or husbands/wives of the person cared34 35 36 37 38. In this study we also confirm this fact, being 62.3% daughters or sons, and 33.3% husbands or wives. This can be explained because these are the relationships in which it exists a greater union between the caregiver and the person cared and, consequently, they probably feel the responsibility to perform the task of caring. In our study we have not found associations between the variable “relationship” and others like “burden” or “depression”, but there are studies that affirm higher level of burden and higher level of depression when the caregivers are sons or daughters of the person cared12 14 34 37.
Living with the person cared has also repercussions on how the caregiver lives the experience of caring. As we found higher social loneliness in those caregivers who lived with the patients, in others studies21 39they found higher burden when caregiver and patient lived together.
The level of patient's dependence for the realization of the basic activities of daily living influences the level of burden of caregivers; some studies detected a positive correlation between caregiver's burden and patient's dependence9 15. By contrast, we found a negative correlation between burden and dependence when comparing burden between caregivers of patients with severe dependence and caregivers of patients with total dependence.
Social loneliness experienced by caregivers is an important variable to take into account because, as we found, it presents associations with others such as the presence of depression. Despite this, it is a variable hardly studied, and future projects should focus on its development and study.
As main contributions to the literature, it can be highlighted the association found between the higher level of caregiver studies and the higher level of burden, especially within the female gender, which predominates at this level of studies. It should also be noted that women live in a worse way the experience of care and they are more affected than men by the disturbances that derive from it.
Knowledge of how burden interferes with caregivers with high educational levels implies that Nurses help to these people, to allow them to continue their careers. These professionals should develop interventions oriented to the intellectual area: decision making, self-help groups… as well as studies to know if decision making is the reason that overload them.
The study has some limitations, the willingness of caregivers to participate in the study and complete the questionnaires. It has been a cross-sectional so it is not possible to stablish causal relationships. Another limitation is the sample size, it would be better a bigger one for generalizing the results; and only one center as setting of the study.
CONCLUSIONS
Finally, we can conclude that women become victims of caring Alzheimer' patients. They experience greater burden (higher when they have high levels of academic studies), anxiety, social loneliness and lower quality of life. As it has been said, caregivers of people with Alzheimer's disease who have a higher educational level suffer a greater deterioration in their quality of life. It is a serious impediment to their personal and professional development, which can have repercussions at other levels and may cause them to take decisions as giving up their professional careers.
These data have relevance to the health field (Clinical Implications), Nurses must know if caregivers are overload by decision making and in this case they should implementing individual adequate interventions.
REFERENCIAS
1. Kirsten MF, Jodie IR, Collen JM et al. The Prevalence and Incidence of Dementia Due to Alzheimer´s Disease: a Systematic Review and Meta-Analysis. Can J Neurol Sci. 2016; 43: S51-82. DOI:10.1017/cjn.2016.36 [ Links ]
2. Garre-Olmo J. Epidemiología de la enfermedad de Alzheimer y otras demencias. Rev Neurol. 2018; 66:377-386. DOI: https://doi.org/10.33588/rn.6611.2017519 [ Links ]
3. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Association; 2013. [ Links ]
4. European Commision. Informal care in Europe. Exploring Formalization, Availability and Quality. Luxembourg: Publications Office of the European Union. 2018. DOI: 10.2767/78836 [ Links ]
5. Ornstein K, Gaugler JE. The problem with "problem behaviors": a systematic review of the association between individual patient behavioral and psychological symptoms and caregiver depression and burden within the dementia patient-caregiver dyad. Int Psychogeriatr. 2012;24(10):1536-52. DOI: 10.1017/S1041610212000737 [ Links ]
6. Seidel D, Thyrian JR. Burden of caring for people with dementia-comparing family caregivers and professional caregivers. A descriptive study. J Multidiscip Healthc. 2019; 12:655-663. DOI: http://doi.org/10.2147/JMDH.S209106 [ Links ]
7. Eby DW, Molnar LJ, Kostyniuk LP. Characteristic of informal caregivers who provide transportation assistance to older adults. PLoS One. 2017; 12 (9): e0184085. DOI: https://doi.org/10.1371/journal.pone.0184085 [ Links ]
8. Del-Pino-Casado R, Pastor-Bravo MM, Palomino-Moral PA, Frías-Osuna A. Gender differences in primary home caregivers of older relatives in a Mediterranean environment: A cross-sectional study. Archives of Gerontology and Geriatrics. 2017; 69:128-133. DOI: https://doi.org/10.1016/j.archger.2016.11.012 [ Links ]
9. Sutcliffe C, Giebel C, Bleijlevens M, Lethin C, Stolt M, Saks K, et al. Caring for a person with Dementia on the margins of long-Term Care: A perspective on Burden From 8 European Countries. J Am Med Dir Assoc. 2017;18(11):967-973. DOI: http://dx.doi.org/10.1016/j.jamda.2017.06.004 [ Links ]
10. Liu S, Li C, Shi Z, Wang X, Zhou Y, Liu S, et al. Caregiver burden and prevalence of depression, anxiety and sleep disturbances in Alzheimer´s disease caregivers in China. J Clin Nurs. 2017; 26(9-10):1291-1300. DOI: 10.1111/jocn.13601 [ Links ]
11. Canonici AP, Andrade LP, Gobbi S, Santos-Galduroz RF, Gobbi LT, Stella F. Functional dependence and caregiver burden in Alzheimer's disease: a controlled trial on the benefits of motor intervention. Psychogeriatrics. 2012;12(3):186-92. DOI: 10.1111/j.1479-8301.2012.00407.x. [ Links ]
12. Cheng S-T, Lam LCW, Kwok T, Ng NSS, Fung AWT. Self-efficacy Is Associated With Less Burden and More Gains From Behavioral Problems of Alzheimer's Disease in Hong Kong Chinese Caregivers. The Gerontologist. 2012;53(1):71-80. DOI: 10.1093/geront/gns062. [ Links ]
13. Dauphinot V, Delphin-Combe F, Mouchoux C, Dorey A, Bathsavanis A, Makaroff Z, et al. Risk factors of caregiver burden among patients with Alzheimer's disease or related disorders: a cross-sectional study. J Alzheimers Dis. 2015;44(3):907-16. DOI: 10.3233/JAD-142337. [ Links ]
14. Jones RW, Romeo R, Trigg R, Knapp M, Sato A, King D, et al. Dependence in Alzheimer's disease and service use costs, quality of life, and caregiver burden: the DADE study. Alzheimers Dement. 2015;11(3):280-90. DOI: 10.1016/j.jalz.2014.03.001. [ Links ]
15. Kang HS, Myung W, Na DL, Kim SY, Lee JH, Han SH, et al. Factors associated with caregiver burden in patients with Alzheimer's disease. Psychiatry Investig. 2014;11(2):152-9. DOI: 10.4306/pi.2014.11.2.152. [ Links ]
16. Hsu TJ, Tsai HT, Hwang AC, Chen LY, Chen LK. Predictors of non-pharmacological intervention effect on cognitive function and behavioral and psychological symptoms of older people with dementia. Geriatr Gerontol Int. 2017; Suppl 1: 28-35. DOI: 10.1111/ggi.13037 [ Links ]
17. Tretteteig S, Vatne S, Rokstad AM. The influence of day care centres designed for people with dementia on family caregivers-a qualitative study. BMC Geriatr. 2017; 17(1): 5. DOI 10.1186/s12877-016-0403-2 [ Links ]
18. García-Alberca JM, Lara JP, Garrido V, Gris E, Gonzalez-Herrero V, Lara A. Neuropsychiatric Symptoms in Patients With Alzheimer´s Disease: the Role of Caregiver Burden and Coping Strategies. Am J Alzheimers Dis Other Demen. 2014; 29(4): 354-361. DOI: 10.1177/1533317513518649 [ Links ]
19. Iavarone A, Ziello AR, Pastore F, Fasanaro AM, Poderico C. Caregiver burden and coping strategies in caregivers of patients with Alzheimer's disease. Neuropsychiatr Dis Treat. 2014;10:1407-13. DOI: 10.2147/NDT.S58063. [ Links ]
20. Shikimoto R, Sado M, Ninomiya A, Yoshimura K, Ikeda B, Baba T, et al. Predictive factors associated with psychological distress of caregivers of people with dementia in Japan: a cross-sectional study. Int Psychogeriatr. 2018; 30 (8): 1089-1098. DOI:10.1017/S1041610217002289 [ Links ]
21. Elmstahl S, Dahlrup B, Ekström H, Nordell E. the association between medical diagnosis and caregiver burden: a cross-sectional study of recipients of informal support and caregivers from the general population study "Goog Aging in Skane", Sweden. Aging Clin Exp Res. 2018; 30(9): 1023-1032. DOI: https://doi.org/10.1007/s40520-017-0870-0 [ Links ]
22. Yikilkan H, Aypak C, Gorpelioglu S. Depression, anxiety and quality of life in caregivers of long-term home care patients. Arch Psychiatr Nurs. 28. United States: 2014 Elsevier Inc; 2014. p. 193-6. DOI: 10.1016/j.apnu.2014.01.001. [ Links ]
23. Zarit SH, Reever KE, Bach-Peterson J. Relatives of the impaired elderly: correlates of feelings of burden. Gerontologist. 1980;20(6):649-55. [ Links ]
24. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4:561-71. [ Links ]
25. Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol. 1988;56(6):893-7. DOI: 10.1037/0022-006X.56.6.893. [ Links ]
26. Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473-83. [ Links ]
27. Pinel Zafra M, Rubio Rubio L, Rubio Herrera R. Un instrumento de medición de la soledad social. Escala ESTE II Madrid: Universidad de Granada; 2009 Available from: http://envejecimiento.csic.es/documentos/documentos/rubio-soledad-este2.pdf (Consulted: 01-08-2019) [ Links ]
28. Pfeiffer E. A short porTable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J Am Geriatr Soc. 1975;23(10):433-41. [ Links ]
29. Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J. 1965;14:61-5. [ Links ]
30. Folstein MF, Folstein SE, McHugh PR. "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189-98. [ Links ]
31. Mosquera I, Larrañaga I, Del Río M, Calderón C, Machón M, García MM. Desigualdades de género en los impactos del cuidado informal de mayores dependientes en Gipuzkoa: Estudio CUIDAR-SE. Rev Esp Salud Pública.2019;93: 28 de enero e201901002. [ Links ]
32. Losada A, Márquez-González M, Vara-García C, Gallego-Alberto L, Romero-Moreno R, Pillemer K. Ambivalence and guilt feelings: two relevant variables for understanding caregivers´depressive symptomatology. Clin Psychol Psychother. 2017; 1-7. DOI: https://doi.org/10.1002/cpp.2116 [ Links ]
33. Dalpai D, Castro R, Camozzato A. Effect of caregiver characteristics on dementia management strategies. Dement Neuropsychol. 2016; 10(2): 143-147. DOI:10.1590/S1980-5764-2016DN1002010 [ Links ]
34. Toribio-Díaz ME, Medrano-Martínez V, Moltó-Jorda JM, Beltran-Blasco I. Rol de Cuidadores informales de los pacientes con demencia en la provincia de Alicante, descripción de sus características. Neurología. 2013; 28(2):95-102 DOI: 10.1016/j.nrl.2012.03.010 [ Links ]
35. Khoo SA, Chen TY, Ang YH, Yap P. The impact of neuropsychiatric symptoms on caregiver distress and quality of life in persons with dementia in an Asian tertiary hospital memory clinic. Int Psychogeriatr. 25. England 2013. p. 1991-9. DOI: https://doi.org/10.1017/S1041610213001518 [ Links ]
36. Miller LA, Mioshi E, Savage S, Lah S, Hodges JR, Piguet O. Identifying cognitive and demographic variables that contribute to carer burden in dementia. Dement Geriatr Cogn Disord. 2013;36(1-2):43-9. DOI: 10.1159/000347146. [ Links ]
37. Conway ER, Watson B, Tatangelo G, McCabe M. Is it all bleak? A systematic review of factors contributing to relationship change in dementia. Int Psychogeriatr. 2018; 30(11): 1619-1637. DOI:10.1017/S1041610218000303 [ Links ]
38. Rosdinom R, Zarina MZ, Zanariah MS, Marhani M, Suzaily W. Behavioural and psychological symptoms of dementia, cognitive impairment and caregiver burden in patients with dementia. Prev Med. 2013;57 Suppl: S67-9. DOI: 10.1016/j.ypmed.2012.12.025. [ Links ]
39. Turró-Garriga O, Garre-Olmo J, Vilalta-Franch J, Conde-Sala JL, de Gracia Blanco M, López-Pousa S. Burden associated with the presence of anosognosia in Alzheimer's disease. Int J Geriatr Psychiatry. 2013;28(3):291-7. DOI: 10.1002/gps.3824. [ Links ]
Received: August 01, 2019; Accepted: November 09, 2019
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
