










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.19 n.58 Murcia Apr. 2020 Epub May 18, 2020
https://dx.doi.org/eglobal.377801
Reviews
Telemonitoring as a health strategy for the accession of the patient with heart failure - integrative review
1Intensive Care Nurse, Master Student of the Professional Master's Program in Nursing Assistance, Federal Fluminense University (UFF) and Member of LASIC Laboratory of Attention to Health of the Elderly.Rio de Janeiro. Brazil. dora.guerreiro7@gmail.com
2Full Professor of the School of Nursing of the UFF, PhD in Nursing, Coordinator of the Center of Attention to the Health of the Elderly-CASIC / UFF Rio de Janeiro. Brazil.
3Nurse PhD student in Health Care Sciences from Fluminense Federal University (UFF) Rio de Janeiro. Brazil.
4Resident nurse of the Cardiovascular Nursing Program at the University of the State of Rio de Janeiro (UERJ) and Member of the LASIC Laboratory of Attention to the Health of the Elderly. Rio de Janeiro. Brazil.
Objective
Identify tele-monitoring strategies for patients with heart failure who collaborate for adherence when it comes to treatment.
Material and Method
Integrative review of the literature carried out in the databases CINAHL, PubMed, Scielo and LILACS. The elaboration of the problem was guided by the PICO strategy that gave rise to the following question: "What are the tele-monitoring strategies for patients with heart failure that contribute to their adherence to treatment?".
Results
Sixteen articles met the criteria defined by the study and, therefore, participated in the analysis of this review.
Conclusion
Tele-monitoring allows the monitoring of a larger number of patients, contributing to the control of signs and symptoms of heart failure. Also, It favors the optimization of pharmacological and non-pharmacological treatments, reducing rates of rehospitalization and mortality.
Keywords: Heart Failure; Telemedicine; Remote Consultation; Nursing Care; Patient Compliance
INTRODUCTION
In the United States, the diagnoses of 550 thousand new cases of Heart Failure are performed each year, being the fifth most frequent cause of hospitalization. In Brazil, there are 238 thousand hospitalizations in the DATASUS Department of Informatics of the Unified Health System, culminating in 26 thousand deaths during hospitalization, representing 9.5% of this total during the year 2012. The BREATHE (Brazilian Registry of Acute Heart Failure) showed a hospital mortality rate of 12.6% 1.
There are approximately 23 million people with Heart Failure (HF) in the world, with an increase of two million cases each year, being more common the hospitalization in the elderly in Brazil. It is a disease that represents a clinical challenge for health professionals because it characterizes as being one of the main heart diseases among several others 1.
The syndrome of heart failure is associated with other chronic diseases and has a progression that deteriorates the health of the person. The evolution of heart disease results in increased hospital admissions, reduced life expectancy, negative repercussions on the quality of life, and it means an overload for the family and society. Disease management and nursing care are planned and developed to support family and caregivers during the transition from the hospital to the home 2.
However, frequent re-hospitalization events, as well as the increase in hospitalization period, lead to an increase in comorbidities and hospital costs. Thus, there is a need to implement other strategies such as telemonitoring directed at the patient with HF. Research on other assistance strategies, such as tele-monitoring, is relevant for decreasing rates of re-hospitalization, clinical decompensation, and the cost of treatment of these patients 3.
In addition, it is believed that the practice of telemonitoring can subsidize an increase in the performance of nursing professionals in the process of prevention of comorbidities and in the reduction of morbi-mortality more prevalent in patients with heart failure (HF).
Based on this assumption, this integrative review was developed with the objective of identifying telemonitoring strategies that contribute to adherence to the treatment of patients with heart failure 4.
MATERIAL AND METHOD
A descriptive and exploratory research was carried out, as an integrative literature review; the descriptive study was developed from observation, description 5. Integrative review is a research method applied to the Evidence Based Practice (EBP), which consists of the incorporation of evidence into the clinical practice of nurses. This method aims to gather and synthesize research results on a thematic, in a systematic and sequenced way, contributing to the deepening of the knowledge of the researched topic 6.
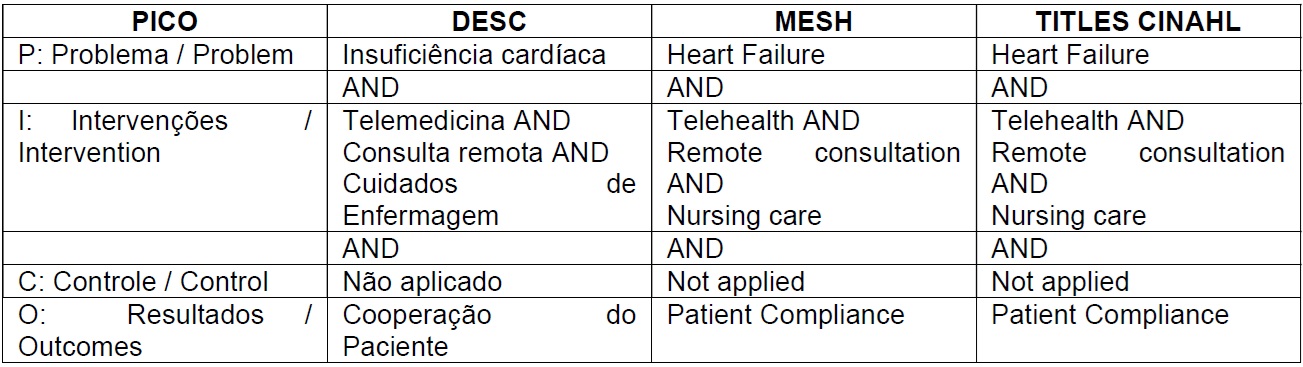
In order to develop the integrative review, the research problem was elaborated through the PICO strategy. The acronym PICO stands for P (Problem / Problem), I (Intervention), C (Control / Control) and O (Outcomes / Results). The C (Control / Control) does not apply, because there was no comparison of two interventions. In this way, the controlled descriptors and Mesh-Therms were aligned in order to raise adequate evidence to solve the research question 7.
From the PICO strategy the question elaborated was: What are the telehealth strategies for patients with heart failure that contribute to their adherence to treatment?
Current Nursing and Allied Health Literature (CINAHL), PubMed, Scielo and LILACS, were selected as portals of the Virtual Health Library (VHL) during the period from March to April 2018. The descriptors (DeCs) research through the portal of the Virtual Health Library were: "heart failure", "telemedicine", "remote consultation", "nursing care" and "patient cooperation" For the search carried out under the PubMed database, the following terms were listed as Medical SubjectHeading (MeSH): "heart failure"; telehealth; "Remote consultation"; "Nursing care" and "patient compliance". The description of the search with the Boolean operators is given in Table 1.
The inclusion criteria applied in the sample survey were: full articles, in the time period from 2013 to 2017, peer reviewed, with samples of patients with heart failure (HF) and age greater than or equal to 18 years. Duplicate studies, integrative review studies, studies on other subjects and studies on telehealth for patients with other conditions other than heart failure, available in the CINAHL, PubMed, Scielo and LILACS databases were excluded (Table 2).
The articles were written in Portuguese, English and Spanish, with the following themes: interventions (educational activities only and / or educational and clinical activities); the theoretical basis and intervention (telephone and / or telemonitoring system); the sample (only the patient, or patient and family and / or caregiver, or hospital resource, for example, medical records); and the attributes of recovery of patients' health and primary and secondary outcomes.

Based on the search carried out, an exploratory reading of the titles and abstracts and their compatibility with the proposed theme were carried out. Then, the articles in English and Spanish were translated by performing the detailed reading in search of evidence aligned with the proposed objectives.
After the reading of the articles, they were grouped into two thematic units, the first thematic unit was referring to telemonitoring strategies, describing the resources and equipment available in each study for health care and the second thematic unit, describes the perception of health professionals and users about the tele-monitoring.
RESULTS AND DISCUSSION
The search procedures of the studies were applied through the use of the descriptors in health sciences and the Mesh Therms in the databases. The results obtained were N = 65 from CINAHL, N = 17 from PubMed, N = 0 studies from the Scielo repository and N = 02 from LILACS. In the process of adoption of exclusion criteria were excluded because they were repeated, N = 01 study belonging to PubMed and N = 02 studies in LILACS. N = 4 studies from CINAHL and N = 2 studies from PubMed were excluded because they were integrative reviews. Studies not applied to the subject consisted of N = 51 in CINAHL and N = 08 in PubMed.
At the end, 16 studies met the criteria and were thoroughly reviewed, of which, N = 10 were derived from the CINAHL Base and N = 6 studies from the PubMed Base. It was evidenced that the year of greatest publication were those of 2014 and 2015, each year with n = 5 publications and the years 2016 and 2013, each year with N = 03 publications respectively.
The PRISMA check list and Flowchart for Systematic Reviews and Meta-Analyzes are intended to provide greater reliability to systematic review studies and meta-analyzes. Although the present study is an integrative review, the PRISMA checklist and flowchart were applied with the objective of bringing quality to it, excluding items referring to systematic reviews. The search flowchart is described in Figure 1 8.
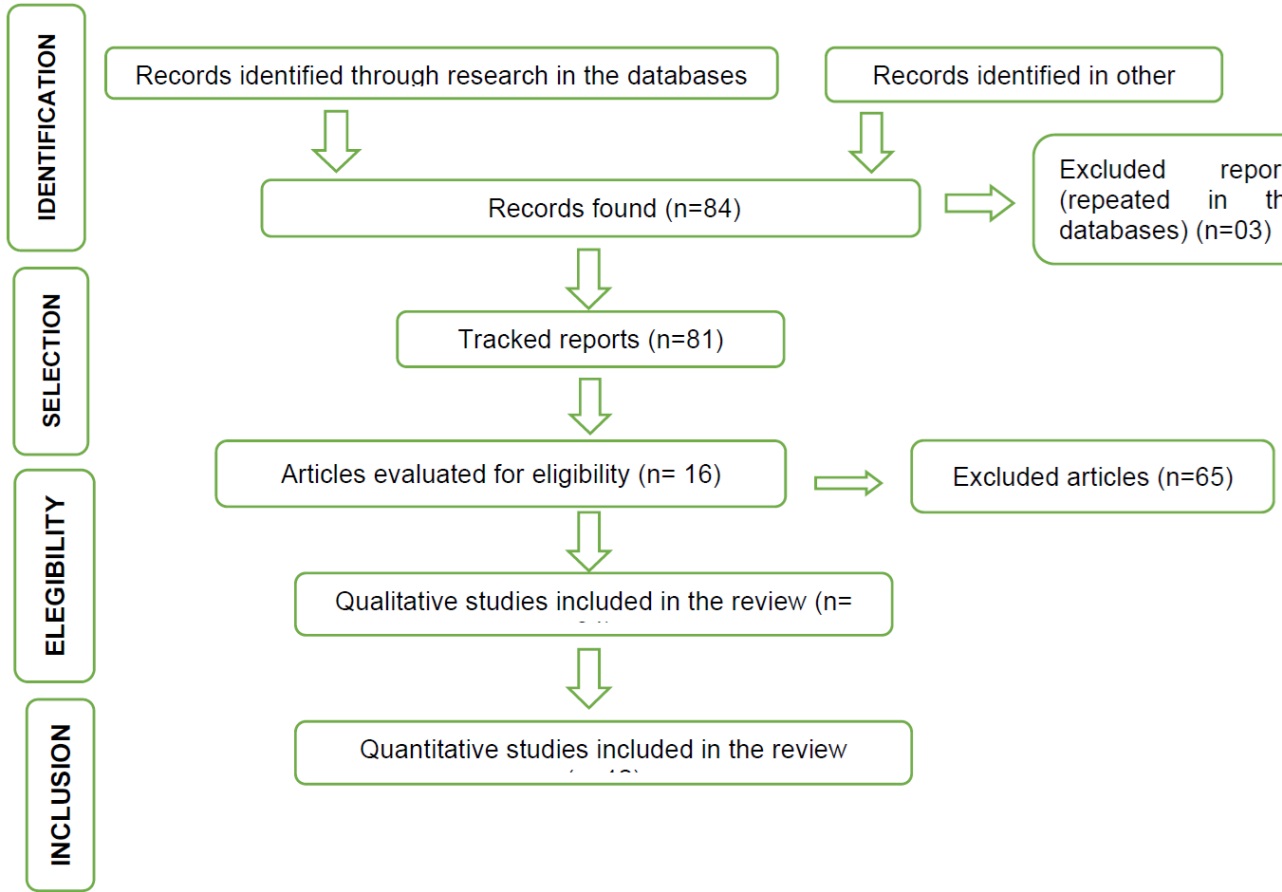
Figure 1. Flowchart of the process of inclusion, selection and identification of the studies elaborated from the PRISMA recommendation.
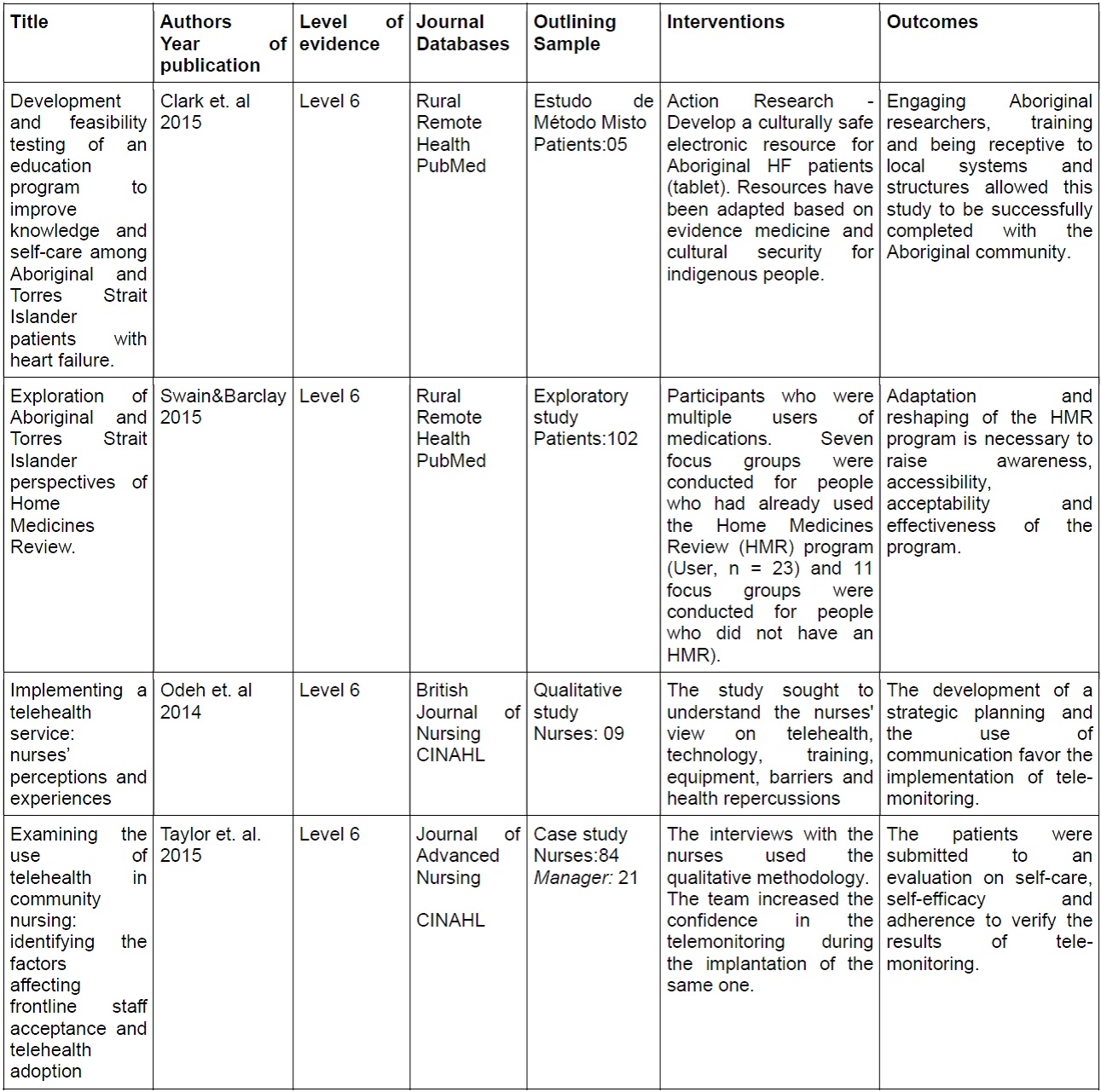
In the analysis of the selected studies, the following attributes were listed in an instrument by the authors: title, year of publication, design, sample, Evidence Level, intervention characteristics and outcomes (Tables 3and 4).
The level of evidence of the studies is delimited according to the study design, that is, methodological design, according to the Evidence Based Practice. The studies are classified into seven levels, they are listed in categories: level 1, systematic review or meta-analysis of the randomized controlled clinical trials; level 2, randomized controlled clinical trial; level 3, controlled clinical trial without randomization; level 4, cohort or case-control study; level 5, systematic review of qualitative and descriptive studies; level 6, descriptive or qualitative studies; level 7, opinions of authorities or experts 9.
In order to facilitate the understanding of the selected articles, two quantitative Tables were elaborated referring to the thematic units discussed in this review, where the results are presented. These are: Telemonitoring Strategies (Table 3); Perception of health professionals and users about telemonitoring (Table 4).
Table 3: Quantitative distribution of the bibliographies found in the databases, PubMed and CINAHL, used in the discussion of the thematic unit Strategies of Tele-monitoring.
| Title | Authors Year of publication | Level of evidence | Journal Databases | Outlining Sample | Interventions | Outcomes |
|---|---|---|---|---|---|---|
| Evaluation of telehealth service for patients congestive heart failure in the north Israel. | Eilat-Tsanani et.al 2016 | Level 4 | Euro J. Cardiovasc Nurs PubMed | Cohort Study Patients: 141 | Monitoring: weight, vital signs, symptoms of cardiac decompensation and use of furosemide. | Evidence indicated a significant reduction of hospitalization through telemonitoring and the Minnesota instrument. |
| Remote Health Monitoring for Older Adults and Those with Heart Failure: Adherence and System Usability | Evans. et. Al 2016 | Level 4 | Telemed J. E. Health PubMed | Case control study Patients: 41 | The remote system consisted of a wireless wristwatch that collected temperature and movement data. The other information was obtained from the use of balance, blood pressure cuff and Tablet. | Study shows adherence to remote system monitoring in the elderly through NeedScale and Technology Experience Questionnaire. |
| Randomized controlled feasibility trial of two telemedicine medication reminder systems for older adults with heart failure | Goldstein et. al. 2014 | Level 2 | J. Telemed. Tele-monitoring PubMed | Randomized Study Patients: 60 | Comparison between four groups analyzing a telehealth intervention, comparing the use of an electronic pill box and the use of the application in the smartphone. | The overall adherence rate was 78%. Patients with a telehealth device joined 80% of the time and people with a mobile device joined 76% of the time. |
| A multidisciplinary telehealth program in patients with combined chronic obstructive pulmonary disease and chronic heart failure: study protocol for a randomized controlled trial. | Bernocchi et. al. 2016 | Level 2 | Trials PubMed | Randomized Controled study Patients: 50-6 | The intervention group, through telephone contact (monitoring of cardiorespiratory parameters) and home rehabilitation program (miniergometer exercises, calisthenics exercises and walking). | The 6MWT was chosen as the main outcome measure. The score was derived from the counting of movements of an electronic physical activity monitor, activity diaries and levels of self-assessed activities. |
| Can Telemonitoring Reduce Hospitalization and Cost of Care? A Health Plan's Experience in Managing Patients with Heart Failure | Maeng et. Al 2014 | Level 4 | PubMed Population Health Management CINAHL | Case control study Patients: 541 | Advanced Bluetooth Monitoring Scales with Interactive Voice Response System were offered to patients with Heart Failure. | Telemonitoring clients showed a 23% decrease in admission chances, 44% in readmission chances in 30 days and 38% in readmission chances in 90 days. |
| Technology, health and the home: eHealth and the community nurse | Peate, Ian 2013 | Level 7 | British Journal of Community Nursing CINAHL | Opinion article | The health and well-being of the client and the family achieve satisfactory results through information communication technology, telephone health advice, text messaging, web-based support, and remote monitoring of vital signs. | Primary outcomes: better monitoring of vital signs; ease of access to emergency services; faster diagnosis and promotion of self-management HF. |
| A Home Telehealth Heart Failure Management Program for Veterans Through Care Transitions | Baldonado et.al. 2013 | Level 3 | Dimensionsof Critical Care Nursing CINAHL | Quasi-experimental study Patients: 100 | The tele-monitoring system consists of a hub, desk, monitor device that connects to a home phone or internet router, facilitating communication with the health team through interactive video and / or audio features. | Telehealth promotes early changes and adjustments in care plans in both clinic and hospital settings. |
| Effects of tailored telemonitoring on heart failure patients' knowledge, self- care, self-efficacy and adherence: A randomized controlled trial | Boyne et. al. 2014 | Level 4 | European Journal of Cardiovascular Nursing CINAHL | Case control study Patients: 382 | The patients were submitted to an evaluation about the knowledge related to self-care, self-efficacy and adherence to verify the results of the tele-monitoring. The clients received four questionnaires with questions about self-care. | The patients were submitted to outpatient visits and monitored by the Health Body. The study showed that there is no clarity about which intervention improves adherence to non-pharmacological treatment. |
| Evaluation of a Veteran-specific Clinic Video Telehealth Pilot Project | Clanton; March& Ruff 2014 | Level 6 | Journal of Nurse Practitioners CINAHL | Descriptive study Records:11 | The study was performed through a medical records review. Demographic and treatment data were obtained from medical records | Video telehealth is a technology not much explored in the health services and the results regarding the cost of treatment are not very wide. |
| Effects of Care Management and Telehealth: A Longitudinal Analysis Using Medicare Data | Baker et. al. 2013 | Level 4 | Journal Of Geriatrics Society CINAHL | Retrospective cohort study Patients: 1767 | The Buddy Health Program (BH) device is an electronic device that collects information about symptoms, vital signs, behavior and health knowledge. | The study showed that the use of the BH program contributed to the reduction of hospitalizations and to a higher survival rate. |
| Telehealth: Enhancing collaboration, improving care coordination | DeBlois&Millefoglie 2015 | Level 4 | Nursing Manage- ment CINAHL | Case control study Patients: 3200 | Web-based telehealth program with the participation of nurses, patient education modules and portals for the exchange of information. | The study showed a decrease in hospitalizations at a rate of 20% to 10%, improvements in self-management of signs and symptoms, and adherence to treatment. |
| Hearing the Veteran's Voice in Congestive Heart Failure Readmissions | Stevenson et. al 2015 | Level 4 | Professional Case Management CINAHL | Case control study Patients: 21 | The study points to health interventions through educational materials, telehealth and ambulatory CHF. | The study points to health interventions through educational materials, telehealth and outpatient CHF, with readmission rates ranging from 35% to 23%. |
Table 4. Quantitative distribution of bibliographies found in databases, PubMed and CINAHL, used in the discussion of the thematic unit The perception of health professionals and users about tele-monitoring.
Telemonitoring strategies
This category includes the articles that describe the tools available in the telemonitoring, making a total of (12) articles; the studies were selected in the databases CINAHL and PubMed.
The health services adopt the strategies according to pre-defined programs, in which the remote consultation can be done by telephone or through electronic equipment. The information is transmitted via web and / or bluetooth; it is necessary to provide fixed or mobile telephone lines for the transmission and monitoring of data through electronic resources such as video monitors, Tablets, alarm boxes, digital scales and wristwatches 10 11.
The instruments of clinical evaluation and health guidelines have variations according to the remote consultation programs. Health professionals perform monitoring of weight, vital signs, signs and symptoms of clinical decompensation of heart failure (HF); the evaluation of functional capacity for daily life activities and health-related quality of life (HRQoL); besides offering support for the patient with HF 12.
The user's poor understanding of discharge readiness has been identified as one of the leading causes of re-hospitalization within 30 days. The patient may find it difficult to assimilate discharge guidelines referring to home self-care due to their clinical conditions and the family, based on factors such as stress, work and home care planning for the patient. Lack of understanding of information provided during hospital discharge can cause uncertainties and make adherence difficult. Effective communication can contribute significantly to the success of transitional care 13.
The remote consultation has been used by nurses as a tool for the educational process, management of the signs and symptoms of decompensation of HF and support for the search of emergency and emergency care. Information on the clinical conditions and pharmacological and non-pharmacological treatment offered to the patient contributes to health promotion, with increased knowledge and improved self-care 14.
The development of new studies is of great value, with a description of the approach taken in the remote consultation and of the applied teaching-learning process, with the analysis of knowledge and self-care variables in HF and the possible clinical outcomes such as re- hospitalization and death, leading to new randomized clinical trials due to their shortage in Brazil 14.
In a study 15who used the Interactive Voice System to answer questions related to physical condition (dyspnea, edema and changes in appetite) and adherence to pharmacological treatment, the weight was monitored by Bluetooth. The sample comprised 541 patients and showed a 23% reduction in admission chances, a 44% chance of readmission in 30 days and a 38% chance of readmission in 90 days. The cost of treatment reduced by 11% during the use of this system.
Another study 16quasi-experimental study, with non-randomized selection, applied to elderly patients with heart failure and life expectancy from 02 to 03 years, a system was developed using text messages and videophone, transmitting patients data on vital signs and clinical parameters for a team of health professionals. The data submitted were analyzed based on evidence medicine. Studies before and after the implementation of telehealth have shown a decrease in total costs with care, visits to the emergency department and hospitalization.
Management of care is addressed in another retrospective cohort study 17integrated by 1767 patients. The Buddy Health System developed in the USA consists of an electronic equipment with screen that captures information related to symptoms, vital signs, behavior and knowledge about health. The information obtained is sent to a software through a secure web portal. The data of the program showed a positive impact on the self-management, contributing to the adherence to the pharmacological treatment, exercises, diets and direct communication with the health professionals.
Managing care associated with the Buddy Health program provides healthcare professionals with the information they need to support clients in reinforcing positive treatment behaviors. The study 1717 identified a decrease in the mortality rate of 15% of the controls in relation to the group in relation to the propensity rate, also including a decrease in the admission rate of 18%.
Corroborating with the above surveys, a cohort study 18performed with 141 patients during one year, focusing on the evolution of the remote referral service, monitored the weight, vital signs and signs and symptoms of cardiac decompensation. The data obtained regarding weight were transmitted to a central and electronic medical record. The research showed a rapid feed-back by the medical professional when patients presented changes in weight. Patients who did not respond to furosemide were directed to an evaluation by a general practitioner. And, the patients with a clinical worsening were oriented to look for an emergency service.
In the same study 18cited above, the application of the Minnesota Quality of Life Instrument score showed a gradual improvement in the parameters on a quarterly basis; this in turn may be related to an increase in confidence in your health care due to tele-monitoring or in relation to an improvement in physical vigor due to weight control. Another relevant parameter was the decrease in hospitalization rate per person (4.7 to 2.6 p <0.001).
The evaluation of health-related quality of life (HRQL) makes it possible to understand several aspects of the individual's well-being, related to the presence of the disease and / or therapeutics. HF reduces patients' functional capacity and ability to perform activities of daily living, leading to a decrease in HRQL 19.
In another study applied in a multidisciplinary telemonitoring program 12, composed of nurses and physiotherapists, the Physical Activity Scale of the Elderly (PASE) and the Minnesota instrument that evaluates Health-Related Quality of Life (HRQL) were used. The randomized study comprised a sample of 50 to 60 patients over a period of 6 months. The follow-up by telephone contact served to verify adherence to therapy, maintain motivation for exercise, educate for the early recognition of signs and symptoms of cardiac decompensation, and evaluate acquired skills.
The aforementioned research 12was implemented to know the efficacy of this technology in patients with HF and chronic obstructive pulmonary disease (COPD) due to the existence of few studies addressing HF and comorbidities. Data from the study were obtained from the Physical Activity Scale of the Elderly (PASE) and from the Minnesota instrument that evaluates Health-Related Quality of Life (HRQL). The quality of life evaluation is an important indicator of the home program; but, it is little applied in the investigations of telemonitoring. Most studies with the Minnesota instrument focus on hospitalizations and mortality; however, there is a lack of studies that address the efficacy of the programs, physical performance and quality of life.
In another research20, the telemonitoring was implemented with an interactive web-based video monitor with support from medical professionals and nurses for patients with HF, COPD, diabetes and wounds. Among the relevant aspects, it is important to highlight the transmission of vital signs and summaries to electronic medical records, facilitating communication among health professionals. Another important parameter was the performance of the physicians in the task group using the diuretic protocol, to avoid the hospitalizations of patients with HF in the terminal phase, evidencing the efficacy of this treatment at home.
The above study shows that the implementation of home care, telehealth and the application of the diuretic protocol 20the following benefits: a) the provision of quality health care; b) reduction of hospitalizations and care in the emergency services, through early interventions such as monitoring of vital signs, use of appropriate medications and consultations with health professionals; c) greater patient compliance through contact with health professionals and informal caregivers; d) e, the decrease of the stress of the patients and improvement of the quality of life, contributing to the autonomy of the patients.
The remote consultation facilitates the patient's access to technology without leaving home, the nurse has the ability to communicate, in this way, a support is offered with the health information, which maintains the standard of attendance of the physical consultations. Consequently, there is a decrease in the search for emergency services by patients, since their needs are met remotely 4.
A retrospective study 21from 11 medical records, brought important data for the deepening of the use of remote consultation, indicating the need for further studies on this form of care. The study analyzed the number of emergency services, admissions, length of stay, scheduled and unscheduled home visits.
The data from the above study 21, showed that the average number of unplanned home visits pre-screened was lower than the average number of unplanned home visits post-tele-monitoring. In addition, the average number of visits to the emergency service during the remote consultation was less than the average number of visits to the emergency service after the remote consultation. It is likely that the increase in the number of post-tele-monitoring consultations is related to the decline in the health of these patients who have chronic diseases, and there is no failure in the telemonitoring.
The remote consultation allows the follow-up of patients with HF through parameters such as vital signs, weight, signs and symptoms of HF decompensation and, through health guidelines. The studies showed that telemonitoring is an efficient and effective strategy for the patient with HF. However, it is emphasized that the transmission of knowledge to the users in an isolated way does not contribute to identify their adherence to the treatment. To achieve this goal, it is essential to base the educational actions with Orem's Theories of Motivation, Self-Determination and Self-Care Deficit, including also the Motivational Interview and Decision-Making Model 22.
Similar study reported the adherence and usability to a remote system by elderly people with chronic diseases or not in an extended period of time. The results showed that the elderly can benefit from a health monitoring system for a long period in order to follow their chronic conditions and stay longer in their homes 10.
Personalized tele-monitoring can aid in the prevention of heart failure decompensation, facilitating patient self-care and providing greater adherence to treatment 11. The education of patients with heart failure is an essential part of controlling the disease. Thus, it is very important to increase the investment in actions that help the diffusion of the knowledge and the education of these patients 23,24. The success of non-pharmacological treatment requires repeated and frequent efforts, enabling the health team to approach the patients with HF and family, consolidating information on HF and self-care 25.
The perception of health professionals and users about telemonitoring
The second category that covers the perception of health professionals and users about telemonitoring, emerged from (04) articles listed in the CINAHL AND PUBMED databases, with emphasis on knowledge, information technology, communication and support for the implementation and development of the consultation remote.
In a study26developed from semi-structured interviews, a group of 16 telemonitoring nurses was asked about this tool, the training, equipment, barriers and repercussions of the strategy on users' health. The findings in the study described the difficult aspects for the remote consultation as: the lack of resources and organizational support, restrictive criteria for patients' enrollment in the remote consultation program and the lack of technical support.
The implementation of a telemonitoring service 26in the professionals, a resistance. To overcome this barrier imposed by professionals, it is necessary to develop strategic planning and the use of communication between the manager and health professionals. Other attributes that strengthen the use of this technology are the training, the collaboration and the support aiming to overcome the obstacles existing for this type of assistance.
In the United Kingdom, a case study 27was developed with eighty-four (84) nurses and professionals who participate in health services and others who do not participate, twenty-one (21) managers and stakeholders. The case study was conducted at four community health services in England to understand how patients were being monitored remotely.
Research data 27show the barriers and facilitating aspects for remote consultation. Among the barriers mentioned, are the acceptance of telemonitoring by the team of professionals, aspects related to the configuration of the services; the lack of clarity regarding the application and efficacy of the technology and the paradigm change regarding the physician's performance in relation to these patients, since other professionals would participate in this care.
With regard to the facilitator aspects 27, the data point out the incentive to trust in technological innovation, the sharing of knowledge and the early identification of barriers by the team with the objective of overcoming them, including also the acquisition of resources for the sustainability of the process.
Health professionals should participate in the planning and construction of an uninterrupted and interactive counseling protocol for patients with chronic illnesses, taking into account necessary changes such as information technology and health technology. The health service will undergo changes based on the patients' demands, in order to meet their needs 4.
Regarding users' views on remote consultation, two studies developed with an indigenous population in Australia were elaborated: based on their cultural characteristics. A research 28had five participants aged 61.6 ± 10 years and class III or IV IC (NYHA). The mixed method was applied, in the first phase the action research contributed to the construction of an electronic resource (Tablet) that evaluated the indigenous population in a safe way. In the second phase, the new resource was tested to verify the acceptability and viability of the indigenous population.
From this study 28two themes emerged: identity (the resource showed the local people's robes, skin tone and voice) and understanding (simple images and text in the first person). Patients reported a high level of satisfaction with the electronic resource 83%. Knowledge about HF increased (percentage of correct answers) from 48.00 plus or minus 6.7% to 58.00 plus or minus 9.7%, an increase of 20.8%, there was a 95% increase in the self-care (46.7 ± 16.0 to 91.1 ± 11.5). Changes in management and maintenance scores varied among patients.
In another study29with the indigenous population, the sample had 102 patients who were divided into eighteen focal groups followed at eleven Aboriginal Health Services. Seven focus groups were performed for people who had already used the HMR program (n = 23) and 11 focus groups were performed for people who did not use an HMR program (n = 79). All the participants realized that the lack of awareness and promotion of the HMR program were factors that contributed to the low adherence to the program. Most users reported that the HMR interview was very helpful in learning more about their medications. However, many reported that they found the process confusing and confronting. The study showed that in the patients' perception, health professionals should develop communication, knowledge transmission, referral and follow-up satisfactorily.
Limitations of the Study
The integrative review was developed under the careful analysis and evaluation of four reviewers, this action does not rule out the risk of bias occurrence. The bias includes any distortion during the search for scientific evidence, which can occur in any type of design. The types of bias can be classified in the following forms: selection bias, information bias and confounding bias. The occurrence of these can be limiting factors for the study 30.
CONCLUSION
Telemonitoring helps to manage the signs and symptoms of cardiac decompensation, weight control and self-care of the patient. The cooperation of the patient with HF during the follow-up by the interdisciplinary team optimizes the results of the pharmacological and non-pharmacological treatment and contributes to the reduction of the rate of re-hospitalization, number of days of hospitalization, mortality and cost.
The telemonitoring facilitates the monitoring of a larger group of users by a smaller number of health professionals in their homes, through the use of monitoring equipment or via telephone consultation, reducing the demand for health services and emergencies by patients with HF.
The remote consultation in the perception of the health professionals requires an adequate infrastructure, technological support, communication, facility for the inclusion of the users in the programs and qualification for the development of this form of assistance.
However, it is necessary to carry out new randomized studies to show the effectiveness and effectiveness of telemonitoring programs. Among these, we highlight studies that evaluate health-related quality of life and primary and secondary outcomes, such as length of hospital stay, re-hospitalization rates, mortality and cost.
REFERENCIAS
1. Poffo M., Assis A., Fracasso M., Londero O., Alves S., Bald A., et al. Profile of Patients Hospitalized for Heart Failure in Tertiary Care Hospital. Int J Cardiovasc Sci. 2017; 30(3):189-198. [ Links ]
2. Chiang L-C, Chen W-C, Dai Y-T, Ho Y-L. The effectiveness of telehealth care on caregiver burden, mastery of stress, and family function among family caregivers of heart failure patients: a quasi-experimental study. Int J Nurs Stud. 2012;49(10):1230-42. [ Links ]
3. Estrada A. Telemonitoramento cardiológico: proposta de atenção humanizada e com redução de custos para pacientes com insuficiência cardíaca. Congresso Nacional de Excelência em Gestão 2015;15. [ Links ]
4. Peate I. Technology, health and the home: eHealth and the community nurse. Br J Community Nurs. 2013;18(5):222, 224-7. [ Links ]
5. Mariano A., Santos M. Revisão da Literatura: Apresentação de uma Abordagem Integradora. AEDEM International Conference. 2017;18. [ Links ]
6. Mendes KDS, Silveira RCPC, Galvão CM. Revisão Integrativa: método de pesquisa para a incorporação de evidências na saúde e nanfermagem. Texto Contexto Enferm. 2008;17(4):758-64. [ Links ]
7. Santos CMC, Pimenta CAM, Nobre MRC. The Pico Strategy for the Research Question Construction and Evidence Search. Rev Latino-Am Enfermagem. 2007;15(3):508-11. [ Links ]
8. Fuchs SC, Paim BS. Meta-Analysis and systematic review of observational studies. Rev HCPA. 2010;30(3):294301 [ Links ]
9. Galvão CM. Evidence Hierarchies. Acta Paul Enferm. 2006;19(2):VI. [ Links ]
10. Evans J., Papadopoulos A., Silvers C., Charness N., Boot W., Schlachta-Fairchild L., et al. Remote Health Monitoring for Older Adults and Those with Heart Failure: Adherence and System Usability. Telemed J E-Health Off J Am Telemed Assoc. 2016;22(6):480-8. [ Links ]
11. Goldstein C., Gathright E., Dolansky M., Gunstad J., Sterns A., Redle J., et al. Randomized controlled feasibility trial of two telemedicine medication reminder systems for older adults with heart failure. J Telemed Telecare. 2014;20(6):293-9. [ Links ]
12. Bernocchi P., Scalvini S., Galli T., Paneroni M., Baratti D., Turla O., et al. A multidisciplinary telehealth program in patients with combined chronic obstructive pulmonary disease and chronic heart failure: study protocol for a randomized controlled trial. Trials. 2016;17(1):462. [ Links ]
13. Stevens, S. Preventing 30-day readmissions. Nurs Clin North Am. 2015 Mar;50(1):123-37. [ Links ]
14. Oliveira, J. et al. Impacto do monitoramento telefônico em pacientes com insuficiência cardíaca: ensaio clínico randomizado. Acta paul enferm. 2017, 30(4):333-342. [ Links ]
15. Maeng D., Starr A., Tomcavage J., Sciandra J., Salek D., Griffith D. Can telemonitoring reduce hospitalization and cost of care? A health plan's experience in managing patients with heart failure. Popul Health Manag. 2014;17(6):340-4. [ Links ]
16. Baldonado A., Rodriguez L., Renfro D., Sheridan S., McElrath M., Chardos J. A home telehealth heart failure management program for veterans through care transitions. Dimens Crit Care Nurs DCCN. 2013;32(4):162-5. [ Links ]
17. Baker L., Macaulay D., Sorg R., Diener M., Johnson S., Birnbaum H. Effects of care management and telehealth: a longitudinal analysis using medicare data. J Am Geriatr Soc. 2013;61(9):1560-7. [ Links ]
18. Eilat-Tsanani S., Golovner M., Marcus O., Dayan M., Sade Z., Iktelat A., et al. Evaluation of telehealth service for patients with congestive heart failure in the north of Israel. Eur J Cardiovasc Nurs J Work Group Cardiovasc Nurs Eur Soc Cardiol. 2016;15(3):e78-84. [ Links ]
19. Pelegrino V., Dantas R., Clark A. Health-related quality of life determinants in outpatients with heart failure. Rev Lat Am Enfermagem. 2011;19(3):451-7. [ Links ]
20. DeBlois D., Millefoglie M. Telehealth: Enhancing collaboration, improving care coordination. Nurs Manag Springhouse. 2015;46(6):10-2. [ Links ]
21. Clanton, R., Sonny R. Evaluation of a Veteran-specific Clinic Video Telehealth Pilot Project. Journal for Nurse Practitioners. 2014): 820-23. [ Links ]
22. Boisvert S., Proulx-Belhumeur A., Gonçalves N., Doré M., Francoeur J., Gallani M. An integrative literature review on nursing interventions aimed at increasing self-care among heart failure patients. Rev Lat Am Enfermagem. 2015;23(4):753-68. [ Links ]
23. Boyne J., Vrijhoef H., Spreeuwenberg M., De Weerd G., Kragten J., Gorgels A., et al. Effects of tailored telemonitoring on heart failure patients' knowledge, self-care, self-efficacy and adherence: a randomized controlled trial. Eur J Cardiovasc Nurs J Work Group Cardiovasc Nurs Eur Soc Cardiol. 2014;13(3):243-52. [ Links ]
24. Stevenson C., Pori D., Payne K., Black M., Taylor V. Hearing the Veteran's Voice in Congestive Heart Failure Readmissions. Prof Case Manag.2015;20(4):177-85. [ Links ]
25. Francis G., Greenberg B., Hsu D., Jaski B., Jessup M., LeWinter M., et al. ACCF/AHA/ACP/HFSA/ISHLT 2010 clinical competence statement on management of patients with advanced heart failure and cardiac transplant: a report of the ACCF/AHA/ACP Task Force on Clinical Competence and Training. J Am Coll Cardiol. 2010;56(5):424-53 [ Links ]
26. Odeh B., Kayyali R., Nabhani-Gebara S., Philip N. Implementing a telehealth service: nurses' perceptions and experiences. Br J Nurs Mark Allen Publ.2014;23(21):1133-7. [ Links ]
27. Taylor J., Coates E., Brewster L., Mountain G., Wessels B., Hawley M. Examining the use of telehealth in community nursing: identifying the factors affecting frontline staff acceptance and telehealth adoption. J Adv Nurs.2015;71(2):326-37. [ Links ]
28. Clark R., Fredericks B., Buitendyk N., Adams M., Howie-Esquivel J., Dracup K., et al. Development and feasibility testing of an education program to improve knowledge and self-care among Aboriginal and Torres Strait Islander patients with heart failure. Rural Remote Health. 2015;15(3):3231. [ Links ]
29. Swain L., Barclay L. Exploration of Aboriginal and Torres Strait Islander perspectives of Home Medicines Review. Rural Remote Health. 2015;15:3009. [ Links ]
30. Almeida CPB, Goulart BNG. How to avoid bias in systematic reviews of observational studies. Rev CEFAC.2017;19(4):551-5 [ Links ]
Received: May 15, 2019; Accepted: July 04, 2019
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
