










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.19 n.59 Murcia Jul. 2020 Epub Aug 10, 2020
https://dx.doi.org/10.6018/eglobal.381641
Originals
Burnout, communication skills and self-efficacy in emergency and critical care health professionals
1 Hospital Vega Baja de Orihuela. Alicante, España.
2Facultad de Enfermería. Universidad de Murcia.España.
3Facultad de Enfermería. Universidad Católica de Murcia. España.
4Departamento de Enfermería. Universidad de Alicante. España. cleal@ucam.edu
Aim:
To analyze the level and relationship between communication skills, perceived self-efficacy and Burnout syndrome in health professionals from the hospital emergency department and the critical care unit of a regional hospital.
Method
An observational and cross-sectional study was conducted with a sample of 90 health professionals from a Regional Hospital, 19 physicians (21.1%), 47 nurses (52.2%), 24 nursing aides (26.7%). The Communication Skills Scale for Health Professionals, the Maslach Burnout Inventory Human Services Survey and the Scale of Perceived Self-Efficacy were utilized.
Results:
A negative correlation was obtained between the different dimensions of the Communication Skills Scale for Health Professionals, the personal accomplishment at work of the Maslach Burnout Inventory and the perceived self-efficacy with the emotional exhaustion and depersonalization dimensions of the Maslach Burnout Inventory. On the other hand, a positive and statistically significant correlation was observed between the dimensions of communication skills with the personal accomplishment dimension in the Maslach Burnout Inventory work and the perceived self-efficacy.
Conclusions
The communication skills and the perceived self-efficacy of the health professionals in the emergency department and critical care unit are related to less emotional exhaustion and depersonalization, and greater personal accomplishment at work.
Keywords: Burnout; Communication; Self-efficacy; Healthcare professionals; emergency department; Critical Care
INTRODUCTION
In general, health professions are intimately related with work stress and this creates a problem not only at the level of the individual, but at the interpersonal or social levels as well1.
The Burnout Syndrome is known as the symptomatic response to chronic work stress situations that are commonly found in care professions as well as other professions that require the direct contact with others. Its presence implies deterioration and wear that affects work satisfaction, involvement and performance, as well as at the personal level of the individual. Aside from the health professionals, other groups that suffer from this syndrome are teachers and high-performance athletes 2)(3.
Three large sets of risk factors (personal, group and organizational) have been linked to the appearance of this syndrome. The factors related with aspects of the workplace environment and the personal factors have had a greater relevance in most of the research works, with the factors of the relationship with the patient being the least taken into consideration until present time4.
This syndrome was described by Herbert Freudenberger in the year 1974 while working in a clinic for drug addicts in New York. Here, he observed that in most of the volunteers in the clinic, there was a progressive loss of energy until exhaustion, symptoms of anxiety and depression, as well as demotivation at work and aggressiveness with the patients after a year of working there5.
Other aspects that could have repercussions on the work environment and on the levels of burnout of health professionals are the communication skills they possess, as they foster mutual understanding, focus on the needs of the patient, share responsibility and establish a clinical relationship characterized by confidence, respect and empathy6. On the other hand, it also has repercussions on their emotional state, their level of stress and their perceived self-efficacy, with this last understood as the beliefs individuals possess about their own skills, referring not only to the resources they truly possess, but also to the professional opinion one has about what he or she can do with them7.
The health professional deals with complex tasks on the daily basis, which are influenced by diverse specific stressful factors related to their profession. These imply a high emotional involvement, and factors related with the organization of work, such as the excess of aversive stimulation (frequently dealing with situations of suffering, death, pain or loss), continuous contact with the ill (which demands a certain degree of involvement to establish a relationship), the frustration of not being able to heal, an objective they have been trained for, among others1)(6.
Therefore, to avoid situations of Burnout in the workplace setting, the professionals should develop personal strategies that are cognitive-behavioral in nature with a self-evaluation character, to eliminate or reduce sources of stress, at the individual and work group levels. The development of adequate communication skills and a perception of self-efficacy can make the health professionals feel more secure, more competent, fomenting the interpersonal relationships with their patients and their work colleagues as well3)(8.
The hospital emergency department (HED) and the Critical Care Units (CCU) require various types of complex technologies, care and treatments, making the task of caring to become mostly focused on keeping the patient alive, setting aside the human quality. It is very common to find the patient isolated from family and friends, naked, full of wires and unknown machines with a multitude of alarms and noises, so that the health professionals face a complex disease in adverse situations9)(10. Thus, they perform their care work under peculiar structural, emotional and care-providing pressures, which makes them more exposed to a greater amount of risks and work stress, which can favor the appearance of the Burnout syndrome (11)(12)(13)(14)(15)(16)(17.
Thus, the main objective of the present study is to analyze the relationship between communication skills, perceived self-efficacy and Burnout syndrome in health professionals from the hospital emergency department and critical care unit of a regional hospital. The secondary objective was to analyze the differences in the scores of the aforementioned variables according to sociodemographic and professional variables.
METHOD
Design
Observational and cross-sectional study conducted at the Vega Baja Hospital in Alicante, Spain.
Population and area of study
The sample was selected with non-probabilistic sampling, at the hospital emergency department (HED) and the critical care unit (CCU) from a regional hospital.
As inclusion criteria, all the participants had to 1) be older than 18, 2) be currently working as a care worker at the HED or CCU, 3) be a physician, nurse or nursing aide, and 4) sign an informed consent form.
To ensure that the sample was representative for a target population of 130 health professionals, the following formula was applied:  , with a level of confidence CI= 0.95 (95%) a deviation of Z=1.96, a margin of error e=0.05 (5%), and a standard of deviation of p= 0.05 (5%) as utilized in previous studies (18, with a sample size of 47 health professionals needed, although a final sample of 90 was obtained.
, with a level of confidence CI= 0.95 (95%) a deviation of Z=1.96, a margin of error e=0.05 (5%), and a standard of deviation of p= 0.05 (5%) as utilized in previous studies (18, with a sample size of 47 health professionals needed, although a final sample of 90 was obtained.
Data collection
In first place, the authorization from the center's management was solicited, and the supervisors from the HED and CCU were contacted. Once the center had accepted to participate in the study, a meeting was conducted with the supervisors in order to present the project and to provide them with the questionnaire material needed (online and physical copy), as well as the period for its completion.
Two formats of the questionnaire were presented to facilitate the adhesion of the personnel to the study, one in digital format through the use of the Google Forms, and another in paper format.
After the data collection period was finished, which lasted a month and a half, a participation rate of 90% was obtained (90 questionnaires completed), a total of 63 in physical format, and 27 in digital format. The paper questionnaires were collected by the nursing supervisors from both hospital units.
Instruments
For the evaluation, the participants completed diverse self-administered instruments which included: Sociodemographic (age, sex, marital status) and professional characteristics (professional category, type of contract, service and work history), designed ad hoc for the present study. Communication Skills Scale for Health Professionals (CSS-HP)19. A self-administered scale composed by 18 items, with a Likert-type response scale with 6 possible responses, composed of four dimensions: Informative communication: composed by 6 items (5, 8, 9, 14, 17 and 18), showing the manner in which the health professionals obtain and provide information, in the clinical relationship they established with their patients. In this dimension, the minimum score is 6 and the maximum is 36. Empathy: composed by 5 items (2,4,6,11 and 12), shows the ability of the health professionals to understand the patient's feelings and making this palpable in their relationship, as well as its behavioral dimension, named empathic attitude, composed by active listening and empathic response. In this dimension, the minimum score is 5 and the maximum is 30. Respect: composed by 3 items (1, 3 and 15). It evaluates the respect shown by the health professionals in the clinical relationship they established with the patients. In this dimension, the minimum score is 3 and the maximum is 18. Social skills: the 4 items in this dimension (7, 10, 13 and 16) show the ability of the health professionals to be assertive or have skillful social behaviors in the clinical relationship they establish with the patients. In this dimension, the minimum score is 4 and the maximum is 24. This tool had good psychometric properties with respect to the analysis of the items, internal structure, reliability (Cronbach's Alpha was 0.65 to 078 in all the dimensions) and external evidence of validity, relating the communication skills with the level of burnout perceived by the health professionals 20.
The Spanish version of the Maslach Burnout Inventory Human Services Survey (MBI-HSS) is the most utilized for evaluating the frequency and intensity of the Burnout syndrome within the healthcare work context. It is composed of 22 items, and the three dimensions that comprise the syndrome can be observed: emotional exhaustion (EE), depersonalization (DP) and personal accomplishment at work (PA). These 22 items are evaluated with a Likert-type scale, in which the subject scores the frequency with which one experiences the feelings that shape the syndrome. The frequency range is shaped by 7 categories ranging from “never” (0) to “every day” (6). The minimum and maximum score range from 0-54 in the EE dimension, from 0-30 for the DP dimension, and from 0-48 in the PA dimension. The internal consistency (Cronbach's α) was satisfactory for the dimensions EE (α=0.85) and PA (α=0.71), and moderate for the DP dimension (α=0.58). The structure of three oblique factors had a good fit 21.
Self-efficacy Scale, contains 10 items that encompass the dimension of the work self-efficacy within them, and evaluates the sTable belief of individuals on their ability to adequately manage a wide gamut of stressors found in everyday life. The minimum and maximum scores of the scale are 10 and 40. The scale showed an internal consistency (α) of 0.87 and a split-half correlation of 0.8822
Data analysis
For data processing, a database was created with Microsoft Excel®. All the questionnaires collected were introduced into this database and the variables were codified. These were posteriorly analyzed with SPSS© v23, with the following analyses performed: descriptive statistics (mean, standard deviation) of the different scores obtained in the quantitative variables by the health professionals (dimensions of the different instruments and age), as well as frequencies and percentages of the sociodemographic variables and professional categories. Also, Pearson's bivariate correlations were performed between the variables studied, as well as differences in means (Student's t-test and one-way ANOVA) between the different dimensions of the MBI, the CSS-HP and the perceived Self-efficacy with the sociodemographic variable sex and the professional variables professional category and work area. Lastly, in the ANOVA tests where significance was found, a post-hoc Tukey's test was applied to identify the significant differences between the professional category variable pairs.
Before performing Student's t-test and the one-way ANOVA, the assumption of normality of the variables was verified with the Kolmogorov-Smirnov test and the homoscedasticity of the variances with Levene's test.
Ethical considerations
The Personal Data Protection guidelines were followed in this study, as established for health-related data23, and the international recommendations: guarantee of the voluntary and informed participation, confidentiality of data and informing the participants about the results. For this, they were given instructions to provide an anonymous “Alias” in the written questionnaires for their posterior analysis.
RESULTS
The final sample was composed by 90 health professionals, of which 47 were nurses (52.2%), 19 were physicians (21.1%) and 24 were Nursing aides (26.7%)
The average age of the sample was 42 years (SD=7.40), with 27.8% being men and 72.2% women. Table 1 shows the descriptive data of the sociodemographic and professional variables of the sample (Table 1).
Of these, 52.5% (n=47) of the health professionals worked as the HED, and 47.8% (n=43) at the CCU, obtaining an adequate response rate from both units: 67.1% from the HED, and 71.7% from the CCU.
Medium-high scores were found in all the dimensions of the CSS-HP, and a high score in the dimension personal accomplishment at work from the MBI-HSS and perceived self-efficacy. On the other hand, intermediate scores were found in the dimension assertiveness and the dimension emotional exhaustion of the MBI-HSS, and low scores in the dimension depersonalization of the MBI-HSS (Table 1).
Table 1. Descriptive statistics of the sociodemographic and professional variables and the dimension of the instruments utilized.

As for the analysis of comparison of means, it can be observed that the men obtained higher scores that the women in all the dimensions of the CSS-HP except for the dimension empathy, in personal accomplishment at work from the MBI-HSS, and in self-efficacy in general. However, these differences were not statistically significant (p>0.05) (Table 2).
Table 2. Descriptive statistics (mean, standard deviation) of the scores of the sample in each of the dimensions of the CSS-HP and the MBI-HSS according to the variable sex.

M: Mean; SD: Standard Deviation; p: Significance; PAW: personal accomplishment at work
If we observe the variables according to hospital unit, we can see that the health professionals from the CCU obtained a higher score in all the dimensions of the CSS-HP as compared to those from the HED, with these differences being statistically significant in the dimensions empathy (t88=4.158; p=0.000), informative communication (t88=2.520; p=0,014) and assertiveness (t88=2.481; p=0.015). In the dimensions emotional exhaustion and depersonalization, the CCU personnel obtained lower scores, with the scores being similar in the other dimensions and perceived self-efficacy (Table 3).
Table 3. Descriptive statistics (mean, standard deviation) of the scores of the sample in each of the dimensions of the CSS-HP and the MBI-HSS according to the variable service.

M: Mean; SD: Standard Deviation; p: Significance; PAW: personal accomplishment at work
The comparison of means analysis according to the professional category variable provided statistically significant differences in the dimensions informative communication (F2,87=4.872; p=0.010), respect (F2,87=3.867; p=0.025), and assertiveness (F2,87=3.503; p=0.034). The post-hoc analysis showed that these differences were between physician and nurses with the nursing aides in the dimensions informative communication and respect, and also between nurses and nursing aid in the dimension assertiveness. As for the general self-efficacy perceived, the group with the highest score was the nurses, followed by the nursing aid technicians and physicians, respectively, although the scores were similar (Table 4).
Table 4. Descriptive statistics (mean, standard deviation) of the scores of the sample in each of the dimensions of the CSS-HP and the MBI-HSS according to the variable professional category.
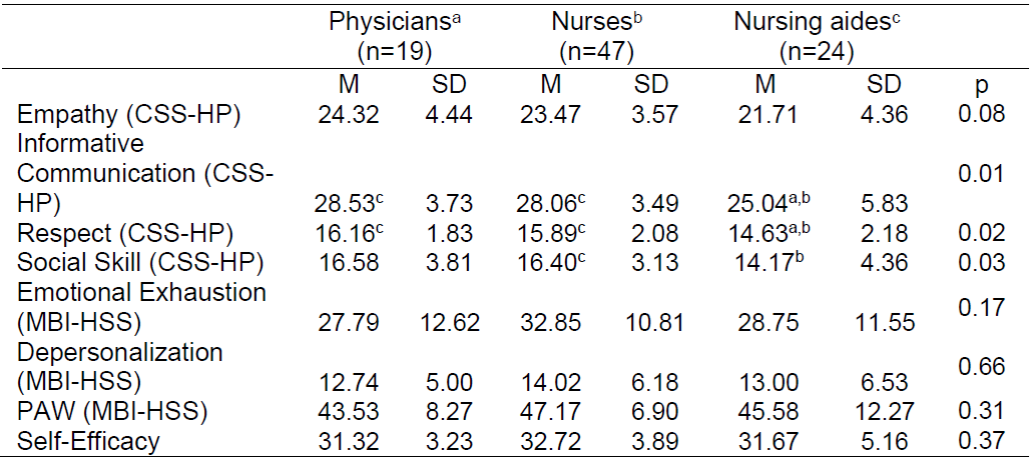
M: Mean; SD: Standard Deviation; p: Significance; PAW: personal accomplishment at work.
a, b, c indicates the professional category with which the statistically significant differences are found p<0.05 in the post-hoc analysis.
The difference in means analysis in the rest of the sociodemographic (marital status) and professional (type of contract and work history) variables did not show any statistically significant differences (p>0.05).
As for the analysis of the bivariate correlations, a negative correlation was observed between the dimensions Emotional exhaustion and Depersonalization of the MBI-HSS and the dimensions of the CSS-HP, the personal accomplishment at work from the MBI-HSS and the perceived self-efficacy. This relationship was statistically significant (p<0.05) between the dimensions perceived self-efficacy and emotional exhaustion, and on the other hand, between the dimensions empathy, respect and perceived self-efficacy with depersonalization.
On the other hand, a positive and statistically significant correlation (p<0.005) was found between the dimension personal accomplishment at work from the MBI-HSS and the dimensions from the CSS-HP and the perceived self-efficacy (Table 5).
Table 5. Pearson's bivariate correlation between the sociodemographic variables (age, sex and time worked), the dimensions of the communication skills (Informative communication, empathy, respect and assertiveness), the dimensions from burnout (emotional exhaustion, depersonalization and personal accomplishment) and the Perceived self-efficacy.
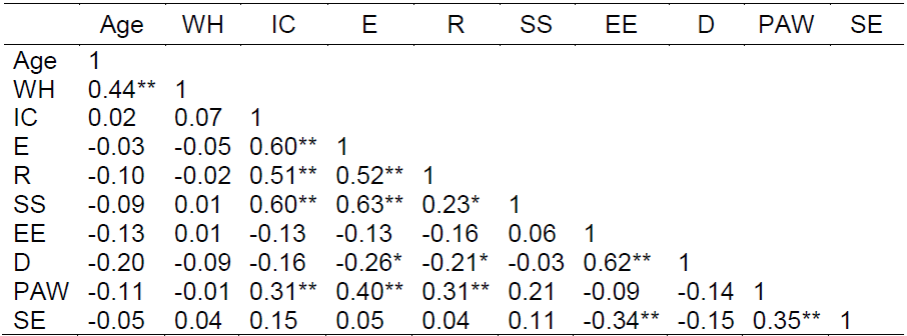
WH= Work history; IC= Informative Communication (CSS-HP); E= Empathy (CSS-HP); R= Respect (CSS-HP); SS= Social Skills (CSS-HP); EE = Emotional Exhaustion (MBI-HSS); D= Depersonalization (MBI-HSS); PAW: Personal Accomplishment at Work (MBI-HSS); SE = Self-efficacy.
** The correlation is significant at the 0.01 level.
* The correlation is significant at the 0.05 level.
DISCUSSION
The aim of this study was to analyze the relationship between communication skills, Burnout syndrome and self-efficacy of a heterogeneous sample composed of three professional groups from the healthcare system in Spain (physicians, nurses and nursing aides) and from two hospital services, the HED and the CCU, where the Burnout syndrome and the need to provide training on communication skills between professionals and patients have been found to be high.
The sample obtained a medium-high score in all the communication skills dimensions, with the physicians and nurses being the groups of health professionals with the highest scores. The collective with the lowest scores in communication skills were the nursing aides. These differences were statistically significant, and in agreement with similar studies3)(24.
On the other hand, it should be emphasized that the health professionals from the CCU obtained higher scores in communication skills with respect to those from the HED, with these differences being statistically significant in empathy, informative communication and assertiveness. However, the scores in burnout and perceived self-efficacy were similar. As for the analysis of the scores according the sex variable, the men generally obtained higher scores in communication skills, except for empathy, personal accomplishment at work and self-efficacy, and the same levels in the dimensions emotional exhaustion and depersonalization.
We can consider that these results are a direct result not only of the training received on the different professional skills described, but also the direct involvement of the institution in fomenting an adequate work context.
A possible solution to the problem of stress of health professionals was discussed by a study4 which stated that the systematic addition of a set of knowledge, resources and communication skills could prevent the burnout syndrome. Thus, training programs where they learn about resources, such as training on communication skills, management of self-esteem, relaxation techniques, coping techniques, etc., could have a positive effect on the prevention of this syndrome. According to our results, the collective with the lowest score in communication skills and the highest score in emotional exhaustion and depersonalization was the nursing aides, who could greatly benefit from these types of programs.
A study24 which analyzed Burnout in a sample of emergency and critical care nurses from a hospital in Andalusia, Spain, confirmed that the sample obtained low scores on emotional exhaustion and depersonalization, and high scores in personal accomplishment at work, without finding high levels of burnout, in agreement with our results.
Likewise, another study25 conducted with physicians from the hospital emergencies unit confirmed that self-efficacy played a fundamental role in transforming emotions at work. Thus, the interventions should be aimed at enhancing self-efficacy, when designing occupational health advocacy programs.
On the other hand, the results of our work are in line with another study3 with a sample of health professionals (physicians, nurses and nursing aides) from various hospitals, both public and private, in the areas of primary care and specialized care, which empirically showed that the communication skills of the health care personnel was a factor of prevention of Burnout. Thus, the results shown in the bivariate correlation analysis of our study are in agreement with other studies3)(26, with a negative relationship observed between the communication skills and the dimensions emotional exhaustion and depersonalization, and a positive relationship between communication skills and personal accomplishment in the area of work.
As the limitations of the study, we could argue that other predictive variables could have been introduced (such as work pressure, self-esteem, stress, among others). Thus, a step forward could be taken and more dimensions could be included that may explain the particularities and specificities of Burnout in health professionals from the HED and CCU.
Other important limitations were that our sampling was not random, the sample was not stratified either according to the service or the type of professional, and the sample was small, despite counting with a great participation of the health professionals. Thus, in the next study, the sample of professional workers included could be increased with those from other health centers. Then, a multi-center study could be conducted, stratifying the sample according to service and professional categories, ensuring that the sample represents all the different professional categories.
CONCLUSIONS
With the results obtained, various conclusions can be made. The health professionals of the sample analyzed had adequate communication skills, a high personal accomplishment at work and perceived self-efficacy. On the other hand, they have a low level of emotional exhaustion and depersonalization. The health professionals with the highest communication skills were the physicians and nurses, with the nursing aides being the group that had the lowest. The men had greater levels of communication skills, except for empathy, personal accomplishment at work and self-efficacy than the women, and the same levels of emotional exhaustion and depersonalization. The health professionals from the CCU had the greatest communication skills, and the least emotional exhaustion and depersonalization with respect to professionals from the HED. The communication skills of the health professionals from the HED and the CCU are related with a lesser emotional exhaustion and depersonalization, and a greater personal accomplishment at work, as well as the increase of self-efficacy acquired.
REFERENCIAS
1. Gil-Monte PR. El síndrome de quemarse por el trabajo (burnout) Una Enfermedad Laboral en la Sociedad del Bienestar. Madrid: Pirámide; 2005. [ Links ]
2. Moreno-Jiménez B, González JL, Garrosa E. Desgaste profesional (burnout), Personalidad y Salud percibida. En Buendía J, Ramos F. Empleo, estrés y salud. Madrid: Pirámide; 2001: 59-83. [ Links ]
3. Leal-Costa C, Díaz-Agea JL, Tirado-González S, Rodríguez-Marín J, Van-der Hofstadt CJ. Las habilidades de comunicación como factor preventivo del síndrome de Bournout en los profesionales de la salud. An Sist Sanit Navar. 2015;38(2):213-23. Disponible en: https://recyt.fecyt.es//index.php/ASSN/article/view/31787/21785 article/view/31787/21785 [ Links ]
4. Cañadas-De la Fuente GA, Vargas C, San Luis C, García I, Cañadas GR, De la Fuente EI. Risk factors and prevalence of burnout syndrome in the nursing profession. Int J Nurs Stud. 2015; 52: 240-9 [ Links ]
5. Castillo-Ávila IY, Orozco JC, Alvis E. LR. Síndrome de Burnout en el personal médico de una institución prestadora de servicios de salud de Cartagena de Indias. Burn Syndr Med Pers a Heal Serv Provid Cart. 2015;47(2):187-92. Disponible en: http://search.ebscohost.com/login.aspx?direct=true&db=fua&AN=103390909&lang=es&site=ehost-live [ Links ]
6. Lucas-Milán MG, Moreno-Manso JM y A Suárez-Muñoz. Comunicación interpersonal e incidencia del burnout en la interacción entre sanitarios y pacientes. Apuntes de Psicología. 2015; 33 (1): 23-29. [ Links ]
7. Bandura, A. Pensamiento y acción. Martinez Roca. Barcelona, 1987. [ Links ]
8. Fuertes Goñi C, Aranda Auserón G, Arroyo Anies MP. Comunicación y mindfulness como prevención del burnout. An Sist Sanit Navar. 2016;39(2):331-3. [ Links ]
9. Pérez-Fuentes MC, Molero-Jurado MM, Gázquez-Linares JJ y MM Simón-Márquez. Análisis de los predictores del burnout en enfermería: factores psicológicos de riesgo y protección. The European Journal of Psychology Applied to Legal Context. 2019; 11 (1) 33-40. [ Links ]
10. Escudero D, Viña L, Calleja C. Por una UCI de puertas abiertas, más conforTable y humana. Es tiempo de cambio. Med Intensiva. 1 de agosto de 2014; 38(6):371-5. Disponible en: http://linkinghub.elsevier.com/retrieve/pii/S0210569114000370 [ Links ]
11. Carrillo-García C, Ríos-Rísquez MI, Martínez-Hurtado R y P Noguera-Villaescusa. Nivel de estrés del personal de enfermería de la Unidad de Cuidados Intensivos de un hospital clínico universitario. Enfermería Intensiva. 2016; 27 (3): 89-95 [ Links ]
12. Fernández Araque A, Cuairán Sola M, Curbelo Rodríguez, R. Calidad de vida profesional de enfermería en urgencias de un hospital de referencia. Enfer Glob 2016; 42: 376-385. [ Links ]
13. Gómez-Martínez S, Ballester-Arnal R, Gil-Julia B y R Abizanda-Campos. Ansiedad, depresión y malestar emocional en los profesionales sanitarios de las Unidades de Cuidados Intensivos. Anales de Psicología. 2015; 31, (2): 743-750. [ Links ]
14. Julián-Jiménez A, Lizcano-Lizcano A, Carrasco-Vidoz CA y S. Estébanez-Seco. Residentes, guardias en el servicio de Urgencias y síndrome de Burnout. An. Sist. Sanit. Navar. 2015; 38 (3): 453-455. [ Links ]
15. Guerrero-Barona E, García-Baamonde E, Moreno-Manso JM y P González-Rico. Estrés laboral e inteligencia emocional en el servicio de urgencias y emergencias 112. Emergencias 2016; 28:353-355. [ Links ]
16. Sánchez Alonso P y Sierra Ortega, VM. Síndrome de Burnout en el personal de enfermería en UVI. Enfer Glob 2014; 33: 252-266. [ Links ]
17. Nespereira-Campuzano T y Vázquez-Campo M. Inteligencia emocional y manejo del estrés en profesionales de Enfermería del Servicio de Urgencias hospitalarias. Enferm Clin. 2017; 27 (3): 172-178. [ Links ]
18. Ríos Risquez MI, Godoy Fernández C, Peñalver Hernández F, Alonso Tovar AR, López Alcaraz F, López Romera A, et al. Estudio comparativo del burnout en personal de enfermería de Cuidados Intensivos y Urgencias. Enfermería Intensiva. 1 de enero de 2008;19(1):2-13. [ Links ]
19. Leal-Costa C, Tirado-González S, van-der Hofstadt CJ, Rodríguez-Marín J. Creación de la Escala sobre Habilidades de Comunicación en Profesionales de la Salud , Introducción Fase I?: Definición del constructo a evaluar y relaciones entre sus componentes y otros constructos externos. Juicio de expertos. An Psicol. 2016;32(1):49-59. Disponible en: http://dx.doi.org/10.6018/analesps.31.3.184701 [ Links ]
20. Leal-Costa C, Tirado-González S, Rodríguez-Marín J, vander-Hofstadt-Román CJ. Psychometric properties of the Health Professionals Communication Skills Scale (HP-CSS). Int J Clin Heal Psychol. 2016;16(1):76-86. Disponible en: http://dx.doi.org/10.1016/j.ijchp.2015.04.001 [ Links ]
21. Gil-Monte PR. Factorial validity of the Maslach Burnout Inventory (MBI-HSS) among Spanish professionals Validação fatorial de Maslach Burnout Inventory (MBI-HSS) para profissionais espanhóis. Rev Saúde Pública. 2005;39(1):1-8. Disponible en: www.fsp.usp.br/rsp [ Links ]
22. Sanjuán-Suárez P, Pérez-García AM, Bermúdez-Moreno J. Escala de autoeficacia general: Datos psicométricos de la adaptación para población española. Psicothema. 2000;12(SUPPL. 2):509-13. [ Links ]
23. Ley Orgánica 3/2018, de 5 de diciembre, de Protección de Datos Personales y garantía de los derechos digitales. BOE. 2018; 294: 119788-119857. [ Links ]
24. Sánchez Romero, S. Prevalencia del Sindrome de Burnout en profesionales de Enfermería de las Unidades de Cuidados Críticos y Urgencias del Hospital Médico-Quirúrgico de Jáen. Enfermería del Trabajo. 2014; 4: 115-125. [ Links ]
25. Castaño MB, Gelaber M, Terol-Cantero MC. La autoeficacia y su relación con la salud psicosocial ocupacional en médicos de urgencias hospitalarias. UCMalue, Revista Académica. 2017;75-91. [ Links ]
26. Yuguero O, Forné C, Esquerda M, Pifarré J, Abadías MJ, Viñas J. Empathy and burnout of emergency professionals of a health region: A cross-sectional study. Medicine (Baltimore). 2017;96(37): e8030. [ Links ]
Received: May 30, 2019; Accepted: September 18, 2019
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
