










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkEnfermería Global
versão On-line ISSN 1695-6141
Enferm. glob. vol.21 no.65 Murcia Jan. 2022 Epub 28-Mar-2022
https://dx.doi.org/10.6018/eglobal.482971
Originals
Risk of type 2 diabetes mellitus and its determinants
1 Estudiante de Doctorado en Ciencias de Enfermería de la Facultad de Enfermería, Universidad Autónoma de Nuevo León. México. marielherediam@gmail.com
2 PhD, Profesora de la Facultad de Enfermería, Universidad Autónoma de Nuevo León. México.
Objective:
Describe the relationship between social determinants of health and risk of type 2 diabetes mellitus in Mexican population.
Methods:
This was a cross-sectional descriptive correlational study of a sample of 256 individuals from a rural community in Sinaloa, Mexico. Data collection was carried out from October 2020 to February 2021. A snowball non-probability sampling method was used. The Instruments used were the International Physical Activity Questionnaire (IPAQ), short version, the IPAQ-A for adults, the IPAQ-C for children, and a sociodemographic, anthropometric, and clinical data sheet.
Results:
The most frequent risk indicators for T2DM for adults are hypertension (81.7%) and overweight/obesity (68.6%); in children, it was overweight/obesity (34.9%). The risk of T2DM increased according to age (r = .560, p < .01) but decreased as education level increased (r = −.127, p < .05)
Conclusions:
The approach to T2DM risk factors from the perspective of social determinants of health allows strategic healthcare planning that considers the contextual factors associated with a lifestyle that reinforces the actions of healthcare providers.
Keywords: Social determinants of health; type 2 diabetes mellitus risk; Mexicans
INTRODUCTION
Type 2 diabetes mellitus (T2DM) is a worldwide public health problem. Its impact is even more severe in developing countries where the disparities in health opportunities are profound. T2DM is among the ten main causes of death globally, with an increase of 70% since the year 2000 1. The world prevalence of T2DM is 9.3%. In 2019, more than four million adults died from the disease, and cases in children and adolescents are increasing 2. In Mexico, the panorama is not different. According to official data from 2018, the prevalence of T2DM was 10.3%, and it was the third cause of death 3. Considering the aforementioned, the percentage of undiagnosed individuals with T2DM is little more than 50%, a finding that highlights the need for timely diagnosis to provide adequate care to delay potential disease consequences in individuals, families, and society in general (1.
Chronic noncommunicable diseases (NCD) such as T2DM are complex and represent a worldwide challenge for society and health systems. The global prevalence of T2DM has been attributed to a complex set of socioeconomic, demographic, and environmental factors and an increase in the risk factors for developing the disease related to unhealthy lifestyles, such as overweight/obesity and low physical activity levels. T2DM requires a deep understanding that considers the biological factors of individuals and the social context in which they develop (1.
Social determinants of health (SDH) provide an opportunity to approach T2DM from a wider perspective. SDH is a concept born from the need to consider health conditions beyond the human biopsychic nexus in which diseases with a large social impact like T2DM develop. The World Health Organization, through the Commission of Social Determinants of Health (CSDH), created the Conceptual Social Determinants of Health Framework, which depicts that health inequalities are distributed in structural and intermediate determinants that affect the health and well-being of the population 4, and also that health inequality has a social cause that precedes and originates it.
SDH is a set of social, political, economic, and biological circumstances in which individuals are born, grow, and develop during their lives. They consist of structural and intermediary determinants. Structural determinants are a complex socioeconomic and political block that determines health conditions in the country. Intermediary determinants include biological, behavioral, genetic, psychological, and lifestyle factors that individuals experiment at every stage of the life cycle 4.
T2DM is a complex disease in which different sociodemographic (structural determinants) and behavioral (intermediary determinants) factors interact. There is scientific evidence that relates SDH with T2DM. On the one hand, there are structural determinants such as being a woman (6, having more than 45 years (7, and failing to screen for chronic noncommunicable diseases (CNCD) (8. On the other hand, there are intermediary determinants, such as low physical activity (9, a high body mass index (BMI) ≥ 25 kg/m2 (10, and low access to health services (11. The need to consider structural and intermediary variables in the appearance of illness is relevant in healthcare. In this sense, we ask: what is the relationship between social determinants of health and risk of type 2 diabetes mellitus in Mexican population?
METHODS
Design, sample, and sampling
This was a descriptive, cross-sectional, correlational study. The total sample was 256 individuals from a rural community in Sinaloa, Mexico, interviewed from October 2020 to February 2021. Snowball nonprobability sampling was performed.
The selection criterion was individuals with a cell or land phone that could receive phone calls. Individuals with a diagnosis of T2DM, defined verbally or by medication and less than six years of age, were exclusion criteria.
Data collection
First, a population with medium and low social inequality 12 was selected to allow a comparison between them. Later, a systematic tour of the community was performed to identify points of reunion (e.g., stores, churches) and distribute flyers that invited people to participate in the study; at the same time, a digital invitation was placed on Facebook to try to reach the greatest number of people. The flyer contained the research objective and a contact number of the researchers so the potential candidate could make a phone call, text, or WhatsApp message to establish first contact.
Patient recruitment began with the first call from the researcher to the participant. The corresponding questionnaires and the sociodemographic, anthropometric and clinical data sheet were applied by telephone and physically completed by the researchers. After finishing the survey, participants were asked to invite third parties to create a response chain to reach more people.
Instruments and measures
The International Physical Activity Questionnaire (IPAQ)-short form for individuals over 15 years of age and two versions for adolescents and children, the IPAQ-A 14) for adolescents 12 to 14 years and the IPAQ-C 15 for children 6 to 11 years were applied. Also, a sociodemographic, anthropometric and clinical data record sheet was applied. All instruments and measures were performed only by phone due to COVID 19 restrictions.
The IPAQ is a seven-item questionnaire that evaluates physical activity according to intensity (mild, moderate, and vigorous), frequency (days), and duration (hours, minutes). Frequency and duration are answered by the number of days and hours-minutes of physical activity per day. Calculations were made automatically on a predetermined Excel spreadsheet provided by the official IPAQ website (www.ipap.ki.se). The reliability of the psychometric properties was assessed with a test-retest, obtaining a correlation coefficient of r = .76 (95% CI, .73-.77) (16). High scores indicated a higher level of physical activity.
The IPAQ-A is a questionnaire that determines the frequency of physical activities carried out by the adolescent in the last seven days. It contains 25 items and has a Likert-type response scale. The final score of the questionnaire ranges from 1 to 5 points and results from the mean of the items. High scores indicate a higher level of physical activity. Regarding the psychometric characteristics reported for the instrument, reliability was .83 with Cronbach's alpha, and validity was .73 (95% CI) using an interclass correlation coefficient 14.
The IPAQ-C is almost identical to the IPAQ-A described above, including the score and interpretation. The only difference is that the IPAQ-C has an additional question about the physical activity that the child performs during recess. The psychometric characteristics of the IPAQ-C were reliability with a Cronbach's alpha of .74 and validity analyzed with a confirmatory factor analysis where factor loadings ranged from .26 to .72 15.
The sociodemographic and anthropometric data record sheet collected data on age, gender, education, activity/employment, completion of a T2DM detection program, completion of an OW/OB detection program, health services affiliation, and the use of health services in the last three months. The anthropometric measures were self-informed. The body mass index was calculated according to the World Health Organization standards with the formula weight/height*height.
Variables
Result variables
Risk of T2DM. A risk index was constructed to evaluate the potential development of T2DM in adults and minors. For adults, this index consisted of six factors: BMI, normal weight (≤ 24.9 kg/m2), overweight/obesity (≥ 25 kg/m2); history of T2DM in parents and/or siblings, yes, no; risk according to age, with risk (≥ 45 years), without risk (18-44 years); Presence of hypertension, yes, no; history of polycystic ovaries (women of reproductive age), yes, no; history of macrosomic infants, yes, no 7. For minors, the risk index consisted of four factors: BMI, normal weight, overweight/obesity (OW/OB); history of T2DM in parents and/or siblings, yes, no; the presence of acanthosis nigricans, yes, no; history of polycystic ovaries in girls (12 to17 years of age), yes, no (17.
Explanatory variables
Structural determinants. These consisted of two variables: Completion of T2DM detection (adults ≥ 20 years), performed, not performed. Completion of OW/OB detection (no age limit) is the completion of detection in the public health sector, performed, not performed.
Intermediary determinants. Composed of three variables: Physical activity (PA), the performance of activities that uses the musculoskeletal system for energy consumption. PA was measured with the IPAQ (≥ 15 years of age), the IPAQ-A (12-14 years), and the IPAQ-C (6-11 years), low, moderate, and vigorous physical activity. Health services affiliation is registration with a public health service, yes, no. Use of health services is the type of health service that the person attended in the last three months, public, private, or not used.
Covariables
The categorical variables were gender, men, women; occupation/activity, no salary (student, housewife, does not work-does not study, works-studies), basic activities (field, construction, and housework), salaried employee (driver, electrician, store clerk, factory worker), and professionals (professionals and retirees). Continuous variables were education and age.
Data analysis
SPSS version 21 in Spanish was used for the statistical analysis. The normality of the study variables was determined with the Kolmogorov-Smirnov test. Pearson's correlation was used to determine the correlation between variables. Categorical variables were expressed as frequencies and percentages.
Ethical aspects
This study was carried out according to the regulations of the General Health Law in Health Research Matters of Mexico (18. It was approved by the Research Committee and the Ethics and Research Committee of the School of Nursing of the Autonomous University of Nuevo Leon. Informed consent was by telephone (audio recording) for adults and by consent for minors.
RESULTS
Demographic characteristics. The results correspond to 256 residents of a rural community in Ahome, Sinaloa. Mean age was 35.75 years (SD = 17.12) and 50.4% (n = 129) were women; the education level was 8.95 years (SD = 3.65) equivalent to basic education (primary and/or secondary school). The most frequent occupation/activity was no salary (student, housewife, does not work-does not study, works-studies) (46.1%, n = 118).
Structural determinants. It was found that 23.8% (n = 61) completed T2DM detection and 45.3% (n = 116) OW/OB detection.
Intermediary determinants. The PA that predominated was low in 40.2% (n = 103). Of the study group, 67.6% (n = 173) were affiliated with a public health institution, and 66.8% (n = 177) did not attend a health service in the last three months. Detailed data can be found in Table 1.
Table 1. Descriptive data of the individuals.

Source: IPAQ-short version, IPAQ-A, IPAQ-C, and a sociodemographic, anthropometric, and clinical data record sheet.
Result variable. T2DM risk indicators with the greatest frequency in adults were hypertension 81.7% (n = 174) and OW/OB 68.6% (n = 174). The predominant risk factor in underage individuals was OW/OB in 34.9% (n = 15) (Table 2).
Table 2. T2DM risk indicators by age group.
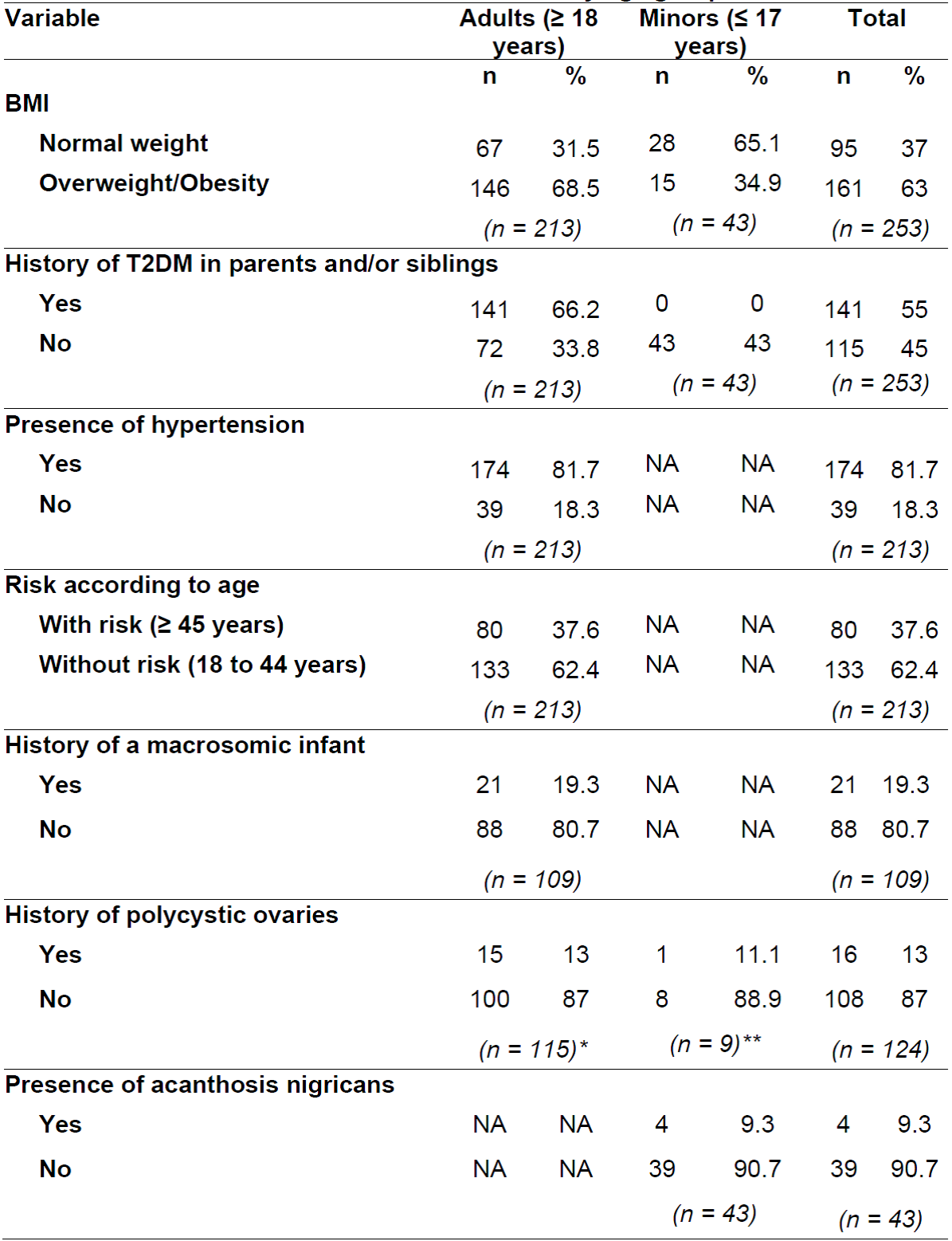
Source: Created by authors. Note: N = 256 (n = 213 adults, n = 43 minors). NA: Not applicable to age group. *Reproductive age women. **Women 12 to 17 years of age.
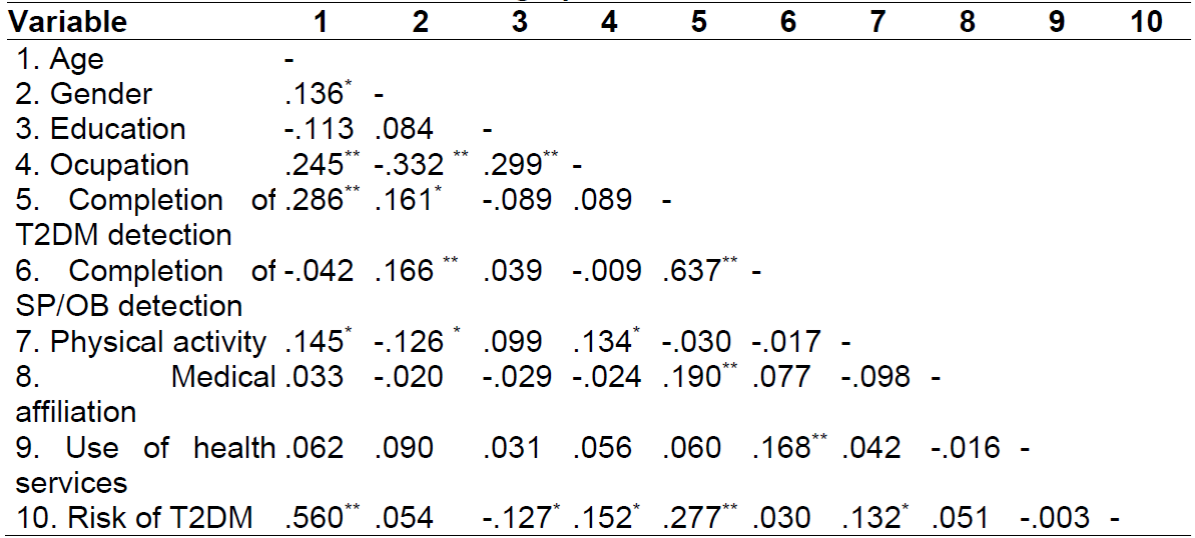
In correlations for structural variables, it was found that with greater age, completion of T2DM detection was more frequent (r = .286, p < .01). Being a woman was positively related with completion of T2DM (r = .161, p < .05) and OW/OB detection (r = .166, p < .01). It was found that the greater the completion of detection of OW/OB, greater was the completion of T2DM detection (r = .637, p < .01). In the relationship of intermediary variables, it was found that the greater the age, the greater the performance of physical activity by the individuals (r = .145, p < .05). People with a public health affiliation underwent T2DM detection more frequently (r = .190, p <.01), and those who used the health services more frequently had more frequent OW/OB detection (r =. 168, p <.01).
Finally, the risk of T2DM increased with age (r = .560, p <.01) but decreased with a greater education level (r = -.127, p <.05). See Table 3.
DISCUSSION
The risk of T2DM is a current public health problem that represents a priority in global health systems. Identifying T2DM risk factors is of great importance to avoid the potential individual, family, and social complications that these entail. Their management, according to SDH, allows knowing if the socioeconomic, political, and biological behavioral context is related to the risk of developing the disease. This study found that more than half of the population did not attend T2DM and OW/OB detections in the last year (although they are offered free of charge by the public health sector). This finding can be explained in part by the fact that a large number of people do not have a public medical affiliation which would involve an extra cost in personal spending added to the confinement caused by the COVID-19 pandemic that led many people to not visit the public and private health services of the country.
As part of the government's strategy to reduce the incidence of T2DM, in Mexico, T2DM and OW/OB detections were implemented free of charge in the public health sector. This research shows that T2DM and OW/OB detections are more frequent as age advances and that women are the main users, coinciding with what was reported by the INEGI in 2018 19. On the one hand, this situation is attributed to the fact that men perceive themselves to be at less risk of getting ill than women 20, which leads them to attend screenings less frequently. On the other hand, there could be a disparity in the gender role. In the economically active population of Mexico, men almost double the economic participation with respect to women, segregating them to carry out unpaid activities such as those of the home, allowing women to go more easily to disease detection tests 21.
Physical activity is key to T2DM prevention. International recommendations emphasize that all age groups perform PA to result in short and long-term benefits. This research found that as age increased, people did more physical activity; however, the physical activity most frequently performed was not enough to lead a healthy life. This situation could create a false perception of health in people that put their health at risk.
Different authors have shown how inequities in medical affiliation and the use of health services affect individual health and can even lead to poverty 22,23. According to official Figures in our country, eight out of ten people have access to health services 18. Part of what was found in this work shows how affiliation and access to public health services favor T2DM and OW/OB detection, partly because these detections are carried out mainly in the public health sector. In this sense, a gradual reduction in T2DM and OW/OB incidence would be expected; however, these diseases continue to increase 24. This finding highlights the importance of adopting a new approach in NCD management, where the government reinforces activities to prevent and control them, using health personnel to transmit recent scientific evidence to the general population 25.
Regarding the risk factors for T2DM, variables such as age and education have been previously studied 26. Our findings coincide with what was found, reinforcing the idea that the risk of T2DM is closely related to people's age and that a high education acts as a protective factor that delays the onset of the disease. Although age is an uncontrollable factor, in this sense, carrying out activities to prevent T2DM should consider educating the population groups so the information provided is completely understood by its recipients 25. Likewise, the high percentage of hypertension and OW/OB in adults and minors found in this research represent highly important predictive factors for the appearance of T2DM in the future, since the appearance of clinical symptoms of T2DM can take years or be associated with other diseases.
Finally, the main limitation of this study was that the non-probabilistic sampling used affects external validity. When extrapolating the results to other populations, similarity in the sample characteristics must be considered.
CONCLUSION
The approach to T2DM risk factors from the perspective of SDH provides an opportunity to propose health strategies that consider simultaneous contextual lifestyle factors that reinforce the actions of health personnel to reduce the morbidity and mortality caused by NCD such as DMT2. This research concluded that the main risk factors for T2DM for adults were suffering from hypertension, while OW/OB is a risk factor shared by adults and minors.
REFERENCIAS
1. Organización Mundial de la Salud. Las diez principales causas de defunción [Internet]. 2021. [Citado 02 mayo 2021]. Disponible en https://www.who.int/es/news-room/fact-sheets/detail/the-top-10-causes-of-death [ Links ]
2. Federación Internacional de Diabetes. Atlas de la diabetes de la FID [Internet]. [Citado 06 mayo 2021]. 2019. [Citado 02 mayo 2021]. Disponible en https://www.diabetesatlas.org/upload/resources/material/20200302_133352_2406-IDF-ATLAS-SPAN-BOOK.pdf [ Links ]
3. Encuesta Nacional de Nutrición y Salud (ENSANUT). Resultados nacionales [Internet]. 2018. [Citado 03 mayo 2021] Disponible en https://ensanut.insp.mx/encuestas/ensanut2018/doctos/informes/ensanut_2018_informe_final.pdf [ Links ]
4. Comisión de Determinantes Sociales en Salud. A conceptual framework for action on the social determinants of health. Social Determinants of Health Discussion Paper 2. WHO Document Production Services. 2010. [Internet]. [Citado 05 mayo 2021]. Disponible en https://apps.who.int/iris/handle/10665/44489 [ Links ]
5. Laurell, A. C. La salud-enfermedad como proceso social. [Internet]. 1982. [Citado 09 mayo 2021]. 2(1): 7-25. Disponible en https://www.terceridad.net/SP3/Biblio%20SPIII_2011_I%20manolo/Laurell-LA%20SALUD%20ENFERMEDAD%20COMO%20PROCESO%20SOCIAL.pdf [ Links ]
6. De Fronzo R A. From the triumvirate to the ominous octet": a new paradigm for the treatment of type 2 diabetes mellitus. Clinical Diabetology [Internet]. 2009. [Citado 11 mayo 2021]. 10(3): 101-128. Doi 10.2337/db09-9028 [ Links ]
7. American Diabetes Association. Standars of care [Internet]. 2021. [Citado 11 mayo 2021]. Disponible en https://care.diabetesjournals.org/content/suppl/2020/12/09/44.Supplement_1.DC1 [ Links ]
8. Aparecida M, Horner B, Guerreiro, D. Atención primaria a las personas con diabetes mellitus desde la perspectiva del modelo de atención a las condiciones crónica. Revista Latino América [Internet]. 2017. [Citado 12 mayo 2021]. 25(1). Doi 10.1590/1518-8345.1474.2882 [ Links ]
9. Leiva A M, Martínez M A, Petermann F, Garrido-Méndez A, Poblete-Valderrama F, Díaz-Martínez X, Celis-Morales C. Factores asociados al desarrollo de diabetes mellitus tipo 2 en Chile. Nutrición Hospitalaria [Internet]. 2018. [Citado 16 mayo 2021]. 35(2): 400-407. Doi https://dx.doi.org/10.20960/nh.1434 [ Links ]
10. Berkowitz S A, Berkowitz T S, Meigs J B, & Wexler D J. Trends in food insecurity for adults with cardiometabolic disease in the United States: 2005-2012. PloS one [Internet]. 2017. [Citado 17 mayo 2021]. 12(6): e0179172. Doi 10.1371/journal.pone.0179172 [ Links ]
11. Pérez Rodríguez A, Berenguer Gouarnaluses M. Algunos determinantes sociales y su asociación con la diabetes mellitus de tipo 2. MEDISAN [Internet]. 2015. [Citado 18 mayo 2021]. 19(10): 1268-1271. ISSN 1029-3019. [ Links ]
12. Consejo Nacional de Evaluación de la Política de Desarrollo Social (CONEVAL). Índice de reza?g?o social 2015 a nivel nacional, estatal y municipal [Internet]. 2015. [Citado 18 mayo 2021] Disponible en https://www.coneval.org.mx/Medicion/IRS/Paginas/Indice_Rezago_Social_2015.aspx [ Links ]
13. International Consensus Group (IPAQ). Cuestionario internacional de actividad física [Internet]. 1996. [Citado 19 mayo 2021]. Disponible en www.ipaq.ki.se [ Links ]
14. Manchola-González J, Bagur-Calafat C, Girabent-Farrés M. Fiabilidad de la versión española del cuestionario de actividad física PAQ-C. Revista Internacional de Medicina y Ciencias de la Actividad Física del Deporte [Internet]. 2017. [Citado 19 mayo 2021]. Doi http://dx.doi.org/10.15366/rimcafd2017.65.008 [ Links ]
15. Moore J B, Hanes J C, Barbeau P, Gutin B, Treviño R P, Yin Z. Validation of the Physical Activity Questionnaire for Older Children in children of different races. Pediatric Exercise Science [Internet]. 2007. [Citado 19 mayo 2021]. 19(1): 6-19. Doi 10.1123/pes.19.1.6 [ Links ]
16. Mantilla-Toloza S M, Gómez-Conesa A. El Cuestionario Internacional de Actividad Física. Un instrumento adecuado en el seguimiento de la actividad física poblacional. Revista Iberoamericana de Fisioterapia y Kinesiología [Internet]. 2007. [Citado 20 mayo 2021]. 10(1): 48-52. Disponible en https://www.elsevier.es/es-revista-revista-iberoamericana-fisioterapia-kinesiologia-176-articulo-el-cuestionario-internacional-actividad-fisica--13107139. ISSN 1138-6045 [ Links ]
17. Norma Oficial Mexicana NOM-015-SSA2-2010. Para la Prevención, Tratamiento y Control de la Diabetes Mellitus [Internet]. 2010. [Citado 19 mayo 2021]. Disponible en: http://www.dof.gob.mx/normasOficiales/4215/salud/salud.htm [ Links ]
18. Reglamento de la Ley General de Salud en Materia de Investigación para la Salud [Internet]. 2014. [Citado 20 mayo 2021] Disponible en http://www.dof.gob.mx/nota_detalle.php?codigo=5339162&fecha=02/04/2014 [ Links ]
19. Instituto Nacional de Estadística Geografía e Informática. Encuesta Nacional de Salud y Envejecimiento en México [Internet]. 2018. [Citado 16 mayo 2021]. Disponible en https://www.inegi.org.mx/contenidos/saladeprensa/boletines/2020/ENASEM/Enasem_Nal20.pdf [ Links ]
20. Academia Nacional de Medicina de México. El hombre y la mujer enferman en forma diferente [Internet]. 2014. [Citado 01 junio 2021]. Disponible en http://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=S0026-17422014000200053 [ Links ]
21. Encuesta Nacional de Ocupación y Empleo [Internet]. 2021. [Citado 01 junio 2021]. Disponible en https://www.inegi.org.mx/contenidos/saladeprensa/boletines/2021/iooe/iooe2021_03.pdf [ Links ]
22. Balandrán-Duarte D A, Mújica Ó J, Narro-Robles J R, López-Cervantes M, Gutiérrez J P, Durán-Arenas J L, Fajardo-Dolci G E. Desigualdad social en México en el uso de servicios de tamizaje en adultos: un análisis de las encuestas nacionales de salud 2006 y 2012. Salud Pública de México [Internet]. 2020. [Citado 03 junio 2021]. 62(5): 511-520. Doi https://doi.org/10.21149/10413 [ Links ]
23. Padovani Clemente S, Pazos San Martín, E., Padovani Cantón A M, Ruano Ortega M. Determinantes sociales de la salud y sistema de gestión de la calidad en servicios estomatológicos. Revista Habanera de Ciencias Médicas [Internet]. 2014. [Citado 04 junio]. 13(5): 757-768. ISSN 1729-519X [ Links ]
24. Centro de Investigación en Alimentación y Desarrollo. La pandemia de diabetes en México. Oficina de Prensa y Colaboradores [Internet]. 2020. [Citado 04 junio 2021]. Disponible en https://www.ciad.mx/notas/item/2450-la-pandemia-de-diabetes-en-mexico [ Links ]
25. Organización Mundial de la Salud. Enfermedades crónicas y promoción de salud. Prevención de enfermedades crónicas [Internet]. 2021. [Citado 04 junio 2021]. Disponible en https://www.who.int/chp/chronic_disease_report/part1/es/ [ Links ]
26. Pinilla A, Barrera M, Rubio C, Devia C. Actividades de prevención y factores de riesgo en diabetes mellitus y pie diabético. Acta médica colombiana [Internet]. 2014. [Citado 04 junio 2021]. 39(3): 250-257. Disponible en http://www.scielo.org.co/pdf/amc/v39n3/v39n3a08.pdf [ Links ]
Received: June 09, 2021; Accepted: September 14, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
