










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.22 n.70 Murcia Apr. 2023 Epub June 26, 2023
https://dx.doi.org/10.6018/eglobal.516121
Reviews
Oral hygiene care to the orotracheally intubated patient: influencing factors. Systematic review
1Nurse at the Algarve University Hospital Center, Faro, Portugal
2Comprehensive Health Research Center (CHRC), Portugal
2Department of Nursing at the University of Évora. Évora, Portugal
Aims:
Identify factors that interfere in the provision of oral hygiene care, developed by nurses, to orotracheally intubated patients in intensive care units, on primary scientific evidence.
Methods:
A systematic literature review study, developed according to the Joanna Briggs Institute protocol. To obtain the articles, a search on B-On( and PubMed( was made. The terms used in the search took into account the vocabulary indexed to the Medical Subject Headings (MeSH) database, having been structured according to Boolean operators, with the following combination in English: “Oral Hygiene” AND “Pneumonia, Ventilator-Associated” OR “Pneumonia, Ventilator Associated” AND “Critical Care Nursing”. Articles published between December 2017 and December 2020, in English, Portuguese and Spanish, available in full, published in peer-reviewed scientific journals (peer review) and which fit the PICO question developed for the study, were defined as limiting.
Results:
After applying the inclusion and exclusion criteria, eight articles of a primary and qualitative nature were included in the review that address the factors that influence the provision of oral hygiene care by nurses to patients undergoing orotracheal intubation.
Conclusions:
The oral hygiene care practices provided to users under orotracheal intubation, by nurses, are influenced by their knowledge, attitudes, available resources, training and institutional policies, as well as by factors related to the user that are mainly related to difficulties in access to the oral cavity.
Key words: Oral Hygiene; Intratracheal intubation; Pneumonia Ventilator-Associated; Critical Care Nursing; Intensive Care Units
INTRODUCTION
The presence of orotracheal intubation is a constant in patients hospitalized in Intensive Care Units (ICU) for the need to maintain the permeable airway, either by the nature of the critical disease, or by the need for sedation, which make it impossible to breathe independently1. However, by allowing mechanically assisted ventilation, the presence of an orotracheal tube predisposes patients to an increased risk of developing pneumonia associated with intubation, by hindering access to the mouth, facilitating biofilm accumulation1 and, on the other hand, by reducing the body's natural defense barriers, such as the cough reflex and the closure of the epiglottis, which ultimately facilitate the entry of microorganisms into the lower airway2. Pneumonia associated with intubation is defined as pneumonia that appears in the person with an orotracheal tube for more than 48 hours or in a person who has been extubated for less than 48 hours3. It is considered the most common3,4) and most deadly healthcare-associated infection in Intensive Care Units (ICU)4, contributing significantly to increased morbidity, mortality, increased days of hospitalization and a significant increase in associated health costs5.
Because it is a global problem, due to its high prevalence and the prognosis associated with pneumonia associated with intubation, a set of intervention bundles have been developed by several countries that aim to prevent it. Oral hygiene is one of the strategies present in these bundles, which occupies a central place in their prevention, by allowing the reduction of the accumulation of dental plaque, biofilms and consequent bacterial load in the oral cavity of the patient under intubation1) significantly reducing the risk of these microorganisms being taken to the lower airways. Despite the guidelines and the known benefits of this action, it is not always considered a priority by institutions and nursing teams, being mostly developed heterogeneously and inconsistently6. Therefore, nursing care plays a central role in the development of highly complex and extremely relevant practices. In this sense, the present systematic literature review (SLR) arises, whose objective is to identify the factors that interfere with oral hygiene care practices developed by nurses to orotracheal intubated patients in the ICU. Their knowledge will make them known in the places of care, allowing the subsequent development of strategies aimed at promoting safe care, based on scientific evidence.
METHODS
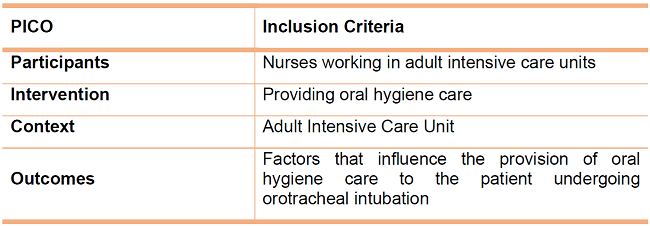
Considering the relevance of the theme, a systematic literature review was carried out according to the guidelines of The Joanna Briggs Institute7. Thus, the respective review protocol was designed, which began with the research question, formulated according to the PICO method: P (Population) -Nurses; I (Intervention) - Provision of oral hygiene care to the patient under orotracheal intubation; C (context): Adult Intensive Care Unit; O (Outcome = Results) - Factors that influence. After the design of the PICO method, the research question was defined: What are the factors that influence oral hygiene care to the patient under orotracheal intubation, provided by nurses in intensive care units?
After the review question was formulated and the objective of the research was structured, the inclusion criteria of the studies were defined, summarized in Table 1.
The research strategy included only published studies and was carried out in three steps. First, a generalist search was performed in the databases Google Scholar, PubMed( and Online Knowledge Library (B-On() that allowed identifying all keywords and descriptors used. Subsequently, a second survey was conducted, with vocabulary indexed to the Medical Subjetct Headings database (MeSH() on April 17, 2021, in the search engines: Biblioteca do Conhecimento Online (B-On() and PubMed(. For this research were used the limiters: articles published between December 2017 and December 2020; available in full text; peer review; published in academic journals and available in Portuguese, English and Spanish.
The terms used in the search were structured according to Boolean operators, with the following combination in English: “Oral Hygiene” AND “Pneumonia, Ventilator-Associated” OR “Pneumonia, Ventilator Associated” AND “Critical Care Nursing”.
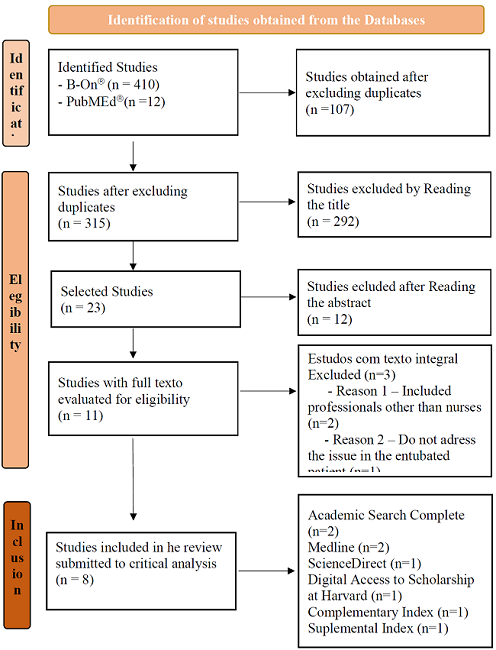
In the third step, articles were selected for inclusion in the systematic review. From the research, 422 articles (410 via B-On( and 12 via PubMed() were obtained. After the removal of duplicates (n=107) resulted in 315 articles. By reading the title, 23 articles were selected (292 excluded). Through reading the abstract, 12 articles were excluded because they did not answer the research question, did not answer the research question in the outlined context or did not present an appropriate methodology, leaving the sample with 11 articles for full text analysis. From these, after evaluation, only primary studies were selected, remaining 8 articles for the systematic review of the literature, belonging to the databases: Academic Search Complete (2 articles), Medline (2 articles), ScienceDirect (1 article), Digital Access to Scholarship at Harvard (DASH) (1 article), Complementary Index (1 article) and Suplemental Index (1 article). This process was carried out independently and autonomously by 2 reviewers, and the selected studies were obtained by their consent. In the flowchart performed (Figure 1), it was possible to systematize the selection process of the studies.
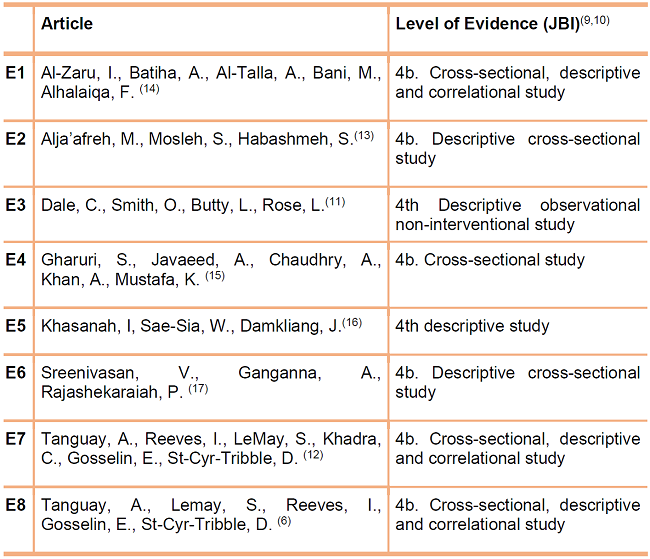
The evaluation of the methodological quality of the selected studies was performed according to the criteria defined by The Joanna Briggs Institute7,8,9 using the levels of evidence according to the characterization of the studies (Table 2) and the instrument “Critical Appraisal Checklist for Analytical Cross-sectional Studies”7, assuming as studies of correct methodology and proven quality those who gathered at least 7 affirmative answers in 8.
RESULTS
The extraction of data from each article was performed by creating a Table (Table 3) that included, for each study, the following information: authors, title, place, year, objective of the study, intervention developed, period of time, type of participants and main results. The presentation of data in a Table is recommended by JBI7 and its main objective is to conduct the narrative process and summaries of the data found.
The articles included in the systematic literature review were published between the years 2017 and 2020 and include nurses and intubated patients, with samples ranging from 28 to 375 nurses and 47 to 428 patients. The context concerns Intensive Care Units (ICU). In its entirety, are descriptive studies, mostly cross-sectional, which used the questionnaire as the main data collection strategy. Regarding the demographic origin of the studies, these were performed in different countries: Canada6)(10)(11, Jordan12,13, Pakistan14, Thailand15 and India16.
Through the analysis and rigorous interpretation of the studies included in this review, we identified that most articles focus on knowledge6)(12)(13)(14)(16, attitude6)(12)(13)(14)(16 and oral hygiene care practice of nurses to intubated patients13)(14)(11)(16. Some of them address the influence of sociodemographic data6,11, resources11)(13)(14)(16 and the existence of standardized instruments of action (guidelines, norms and/or protocols)6)(11)(12)(13)(15)(16 in the practice of care. Other included studies also address the factors related to the difficulty of access to the oral cavity of users for the provision of hygiene care10)(14)(16.
Table 3: Summary of studies obtained - Factors that interfere in the provision of oral hygiene care to patiens undergoing orotracheal intubation.
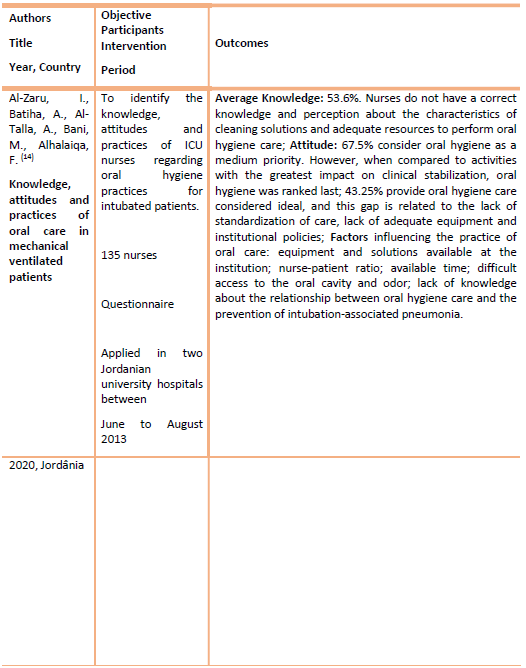
Table 3 (cont.): Summary of studies obtained - Factors that interfere in the provision of oral hygiene care to patiens undergoing orotracheal intubation.
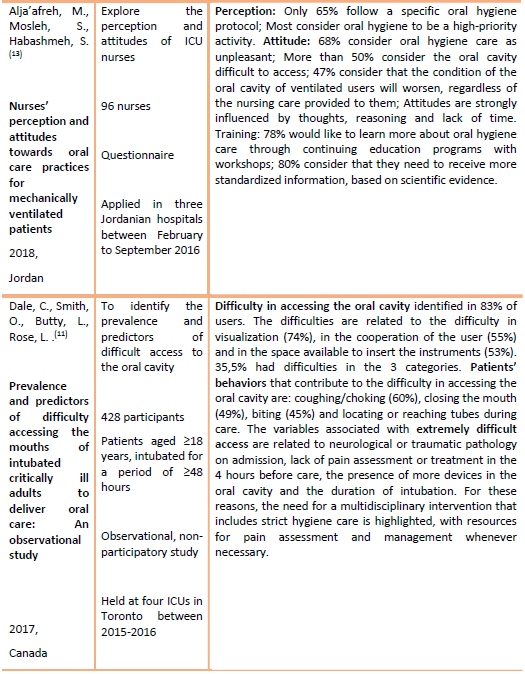
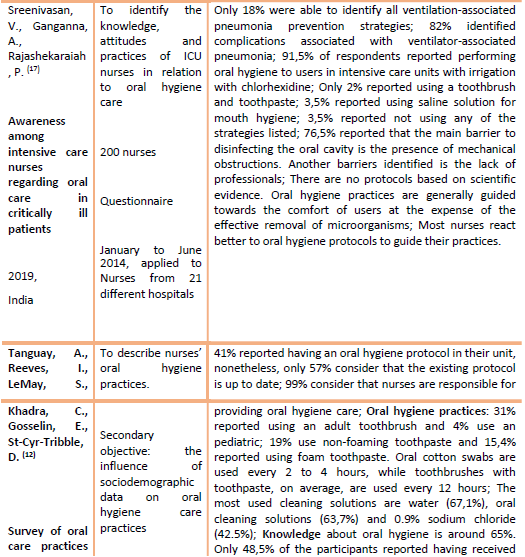
Table 3 (cont.): Summary of studies obtained - Factors that interfere in the provision of oral hygiene care to patiens undergoing orotracheal intubation.
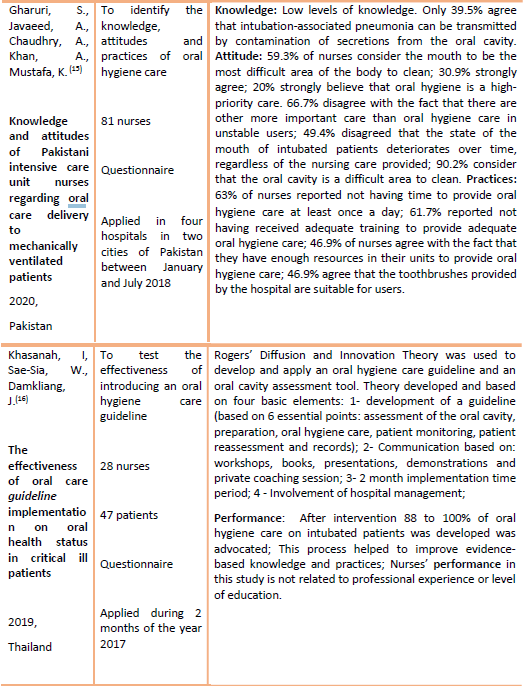
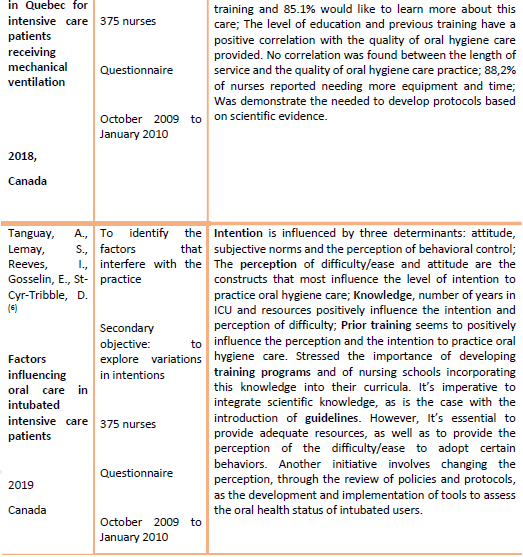
Table 3 (cont.): Summary of studies obtained - Factors that interfere in the provision of oral hygiene care to patiens undergoing orotracheal intubation.
DISCUSSION
In the studies analyzed, although all of them are directed to the practice of oral hygiene care to intubated users, the knowledge of nurses was evaluated in relation to their knowledge of the correct practice of oral hygiene11)(12)(13, the mechanisms of transmission14 and strategies to prevent pneumonia associated with intubation16, since all these are related. In the analyzed samples, the knowledge of nurses is considered median/low11)(12)(13. In the study by Al-Zaru, Batiha, Al-Talla, Bani & Alhalaiqa13, the results indicate that nurses do not have adequate knowledge about the correct care practice, nor a clear perception of the ideal characteristics of the cleaning solutions used in the oral cavity (ranging from the use of chlorine-hexidine, sodium chloride, hydrogen peroxide and sodium bicarbonate).
Al-Zaru et al 13 also show that nurses are unaware of the appropriate equipment for the removal of dental plaque, since they identify as the main resources to be used for this function, the foam sticks and oral swabs (80% of respondents)13) to the detriment of the use of small and soft bristle brushes17)(18)(19 preferably with an incorporated suffocation system, defined in the literature as the appropriate resource18). These data meet the study developed by Tanguay, Reeves, LeMay, Khadra, Gosselyn & Cry-tribble11, which identified that the knowledge of nurses in relation to the correct practice of oral care is considered low, and by the study conducted by Alja'afreh et al, 201812, in which most respondents do not correctly identify the indicated frequency for oral cavity aspiration and only 63% identify the correct frequency for the use of toothbrush.
Guari, Javaeed, Chaudry, Khan & Mustafa14 evaluated the knowledge of nurses regarding the mechanisms of transmission of pneumonia associated with intubation and despite considering that in general nurses have good knowledge, Regarding the practice related to oral hygiene care, only 40% of respondents agree that the disease can be transmitted by contaminated oropharyngeal secretions. This fact is corroborated by Al-Zaru et al13, since they identified that there is a lack of knowledge of nurses about the relationship between oral hygiene care and the prevention of pneumonia associated with intubation.
Sreenivasan, Gangana & Rajashekaraiah16 evaluated nurses' knowledge of strategies to prevent pneumonia associated with intubation and only 18% of nurses correctly identified the listed strategies. However, 82% of respondents were able to identify the consequences associated with pneumonia associated with intubation listed by the questionnaire (increased days of hospitalization; increased mortality; increased costs associated with hospitalization).
Regarding the origin of nurses' knowledge in relation to the practice of oral hygiene, Al-Zaru et al13, report that the majority of senior nurses transmit them, followed by nursing schools.
There are a number of factors, identified by the studies, that interfere with the attitude of nurses in relation to oral hygiene care. These mainly involve the prioritization of oral hygiene in relation to other care provided by nurses12)(13)(14, thoughts and reasoning associated with care12,14, and evaluation (favorable/unfavorable, ease/difficulty) that professionals make the act of sanitizing the mouth of orotracheal intubated users, which ultimately influences their level of intention to practice care 6.
In general, nurses surveyed by the studies identified consider oral hygiene care as a high priority activity12,14. However, Al-Zaru et al13, were more incisive in their analysis and identified that nurses consider the oral hygiene of the intubated user as a median priority, when compared to other daily activities such as the physical evaluation of the user, respiratory kinesiterapy, alternation of decubitus, hygiene care and bed comfort, among others. However, when comparing oral hygiene with activities that are related to the clinical stabilization of the patient, such as the administration of oxygen therapy, aspiration of secretions, administration of therapy, admission of users in the Intensive Care Unit, and the maintenance practices of catheters, which was classified as last13.
Concerning the thoughts and reasoning associated with this care, in the studies identified by Alja'afreh et al12 & Gharuri et al14, a large percentage of nurses believe that the state of mouth of orotracheal intubated patients shall worsen, regardless of the care given. Being the oral cavity of the intubated patients considered by 90,2% of the respondents in the study of Guari et al14 as an area of the body difficult to sanitize. Alja'afreh et al12 adds that this task is considered by 68% of nurses as unpleasant. Since odor is one of the factors identified by Al-Zaru et al13, which contributes most to this association. Tanguay et al6 add that the perception of the ease/difficulty to perform a given task and the favorable/unfavorable evaluation to adopt it are the constructs that most influence the level of intention of oral care practice. Several authors emphasized that the involvement of hospital institutions, along with teaching institutions, plays a key role in the transmission of knowledge and the inherent construction of knowledge, thoughts and associated reasoning6)(12)(15)(16.
In the studies analyzed, the practice of oral hygiene care to intubated patients is considered heterogeneous16) and of low quality11)(12)(13, being mainly a task considered for the comfort and well-being of users, to the detriment of the effective removal of microorganisms(13.16). This relates to knowledge (already stated), resources, time, experience, need for adequate training and institutional policies.
In terms of resources, the practice is influenced by the widespread lack of adequate means for the provision of oral hygiene care13,16 and the equipment provided by institutions6)(11)(13)(14.
In relation to time, most nurses surveyed in the studies report not having adequate time to provide oral hygiene care6)(11)(12)(13)(14)(16 and this factor is greatly influenced by the ratios (nurse-user) in the services11,13,16. Being highlighted by the study conducted by Guauri et al14, 63% of nurses reported not having time to provide oral hygiene care at least once a day.
Regarding the influence of sociodemographic data in the practice of oral hygiene care, Tanguay et al11 & Al-Zaru13 report that nurses with more years of experience in ICU tend to provide oral hygiene care 11,13 and to perform structured oral cavity evaluations more frequently11. However, in the only correlational study found in the sample, no correlation was found between the length of service in the ICU and the quality of oral hygiene practice11. Tanguay et al 11 referred that the only positive correlation found in the quality of care is related to the level of education and previous training of nurses.
Specific training programs are identified by many of the nurses surveyed in the studies as a pressing need6)(11)(12)(14. Thus, the importance of the involvement of hospital institutions is also praised6)(12)(13)(16, through the development of educational programs directed to the needs of nurses6)(12)(15 that facilitate the introduction of scientific knowledge in the practice of care12 and that contradict the data found in the study of Al-Zaru et al13, which identify as the main source of knowledge of this practice, the transmission made by senior nurses. Another measure involves the introduction of standardized instruments, through updated protocols or guidelines6)(11)(13)(16, since most nurses react better to standardized information available in the work areas to guide their practices, increasing their commitment to oral hygiene care to intubated patients12,16. As these measures, the development of comprehensive educational programs and the introduction of instruments that guide the performance of professionals in oral hygiene care, one of the recommendations presented in several articles and experts' opinions that address this issue1)(2)(18.
Regarding the presence of action protocols or guidelines in the sample studies, their presence is quite variable. Alja'afreh et al12 reported that in the three hospitals analyzed in Jordan, 65% of respondents reported having protocols of action. Tanguay et al11, in their study conducted in two university hospitals in Canada, highlight that only 41% of respondents have protocols of action, however, 57% consider them outdated. On the other hand, Sreenivasan et al16 developed their study in India, in 21 hospitals, and report that the protocols are non-existent.
The influence of the introduction of training programs and protocols is quite noticeable in the study developed by Khasanah, Sae-Sai and Samkliang15, in Thailand. After the elaboration of a structured teaching program (with workshops, presentations, and private coaching sessions), with development and introduction of a Guideline and support of hospital management over two months, they obtained a performance of 88 to 100% of the nurses included in the sample, during the oral hygiene care contemplated in the Guideline developed, with significant increases in the state of oral health of the users. Nevertheless, Alja'afreh et al12 emphasize that it is not enough to develop training programs and standardize care. These are one of the ways identified by studies to increase nurses' knowledge and influence them in the acquisition of perceptions and attitudes that may influence practice, based on scientific evidence6,12. It is also necessary to monitor the practice of care12, so that it is possible to raise awareness of them and to implement strategies aimed at improving them.
Some of the studies analyzed identify as influencing factor of oral hygiene care practices the great difficulty in accessing the oral cavity of intubated users10)(14)(16. Since the main difficulties encountered are related to visualization10, the space available to insert instruments10,16 and the lack of cooperation of the user10. These difficulties are amplified when users have neurological or traumatic pathology on admission (to the detriment of medical pathologies), when they have more than one device in the oral cavity, more days of intubation and present periods of agitation and pain in the four hours preceding oral hygiene care10. Users' behaviors that contribute most to access difficulties include coughing/choking, closing the mouth, biting, and locating or reaching devices during care. In this way, the importance of a multi-disciplinary approach, including the provision of rigorous oral hygiene care, using the assessment and management of agitation and pain, whenever necessary, is highlighted10.
This study has some limitations, because it was limited to the selected languages, the lack of consensus in the questionnaires used by the authors and some lack of consensus definition in the terms used as: attitude, perception and knowledge. Another limitation is the lack of characterization of oral care practice considered appropriate for each reality, when there are no protocols or institutional guidelines.
CONCLUSION
Ensuring that the practice of oral hygiene care to users under orotracheal intubation is successful implies an effective and joint work of institutions, nurses and a multidisciplinary and holistic approach to the user. To answer the question of research formulated, it is possible to conclude that the practice of oral hygiene care of nurses to users under orotracheal intubation is influenced by their knowledge, attitude, resources available, time available, training and institutional policies, as well as, by factors related to the user, which are mainly related to difficulties in accessing the oral cavity.
The articles studied present convergent results, and point out as an urgent need the development of educational and training programs aimed at increasing the know-how of nurses regarding the mechanisms of transmission and prevention strategies of pneumonia associated with intubation, highlighting the need for correct oral hygiene practice. These programs should be directed to nurses and seek the transmission of knowledge based on updated scientific knowledge, aimed at demystifying erroneous thoughts and reasoning, often associated with these practices. These should seek the change of practice, currently based on the comfort and well-being of the user, for a safe and sustained practice that seeks the effective removal of microorganisms and prevention of their arrival in the lower airways. Another of the institutional measures identified is the introduction of updated standardized instruments of action (in the form of guidelines or protocols) that guide the performance of the nursing team and increase their commitment to oral care, and is also necessary for its monitoring. However, it is not enough to bet on the transmission of knowledge and consequent change of attitudes, an active role is essential on the part of health institutions that aim to provide services with adequate resources. These resources include the availability of adequate equipment for the provision of safe oral hygiene care, as well as professionals, increasing the nurse-user ratio and allowing greater time availability for the provision of oral hygiene care.
The literature also points to the need for a multidisciplinary approach to the user who seeks to increase their comfort and well-being, reducing the difficulties of access, visualization of the oral cavity and cooperation of the user, passing these measures, evaluation and management of agitation and pain, allowing the provision of safe oral hygiene care.
This study is relevant, current and convincing of the emerging need for institutions and health professionals to unite in the path of continuous improvement of oral hygiene care practice, with a significant impact on the health of patients under orotracheal intubation.
REFERENCIAS
1. Wainer C. The importance of oral hygiene for patients on mechanical ventilation. Br J Nurs. [Internet]. 2020 [citado 2021 Abr 22]; 29(15): 862-863. Available at: https://www.magonlinelibrary.com/doi/epub/10.12968/bjon.2020.29.15.862 [ Links ]
2. Gershonovitch R, Yarom N, Findler M. Preventig Ventilartior-Associated Pneumonia in Intensive Care unit by improved oral care: a review of randomized control trials. SN Compr. Clin. Med. [Internet]. 2020. [citado 2021 Abr 25]; 2: 727-733. Available at: https://link.springer.com/article/10.1007/s42399-020-00319-8 [ Links ]
3. Direção-Geral da Saúde. "Feixes de Intervenções" de Prevenção de Pneumonia Associada à Intubação. DGS [Internet]. 2017 [citado 2021 Abr 22]. Available at: https://www.dgs.pt/directrizes-da-dgs/normas-e-circulares-normativas/norma-n-0212015-de-16122015-pdf.aspx [ Links ]
4. Kovacs CS, Modi AR. Hospital acquired and ventilator-associated pneumonia: Diagnosis, management and prevention. Clev Cli J Med. [Internet]. 2020 [citado 2021 Abr 22]; 87 (10): 633-639. Available at: https://www.ccjm.org/content/ccjom/87/10/633.full.pdf [ Links ]
5. Luckraz H, Manga N., Senanayake E, Mahmoud A, Gopal S, Charman SC, Giri R, Oppong R, Andronis L. Cost of treating ventilator associated pneumonia post cardiac surgery in the National Health Service: results from a propensity-matched cohort study. J Intensive Care Soc. [Internet]. 2018 [citado 2021 Mar 15]; 19 (2): 94-100. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5956688/ [ Links ]
6. Tanguay A, LeMay S, Reeves I, Gosselin É, St-Cyr-Tribble D. Factors influencing oral care in intubated care patients. Nurs Crit Care. [Internet]. 2019 [citado 2021 Abr 22]; 25: 53-60. Available at: https://pubmed.ncbi.nlm.nih.gov/31305004/ [ Links ]
7. Joanna Briggs Institute. The JBI Critical Appraisal tools for use in JBI Systematics Reviews - Checklist for Analytical Cross-Sectional Studies. JBI [Internet]. 2021 [citado 2021 Abr 22]. Available at: https://wiki.jbi.global/display/MANUAL/Appendix+7.5+Critical+appraisal+checklist+for+analytical+cross-sectional+studies [ Links ]
8. Page M, McKenzie J, Bossuyt P, Boutron I, Hoffmann T, Mulrow C, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ [Internet]. 2021 [citado 2021 Abr 22]; 372(71). Available at: https://www.bmj.com/content/372/bmj.n71 [ Links ]
9. Joanna Briggs Institute. Developed by the Joanna Briggs Institute Levels of Evidence and Grades of Recommendation Working Party October 2013. JBI [Internet]. 2013 [citado 2021 Abr 22]. Available at: https://jbi.global/sites/default/files/2019-05/JBI-Levels-of-evidence_2014_0.pdf [ Links ]
10. Joanna Briggs Institute. The Joanna Briggs Institute Levels of Evidence and Grades of Recommendation Working Party*. Supporting Document for the Joanna Briggs Institute Levels of Evidence and Grades of Recommendation. JBI [Internet]. 2014 [citado 2021 Abr 22]. Available at: https://jbi.global/sites/default/files/2019-05/JBI%20Levels%20of%20Evidence%20Supporting%20Documents-v2.pdf [ Links ]
11. Dale CM, Smith O, Burry L, Rose L. Prevalence and predictors of difficulty accessing the mouths of intubated critically ill adults to deliver oral care: an observational study. Int J Nurs Stud [Internet]. 2018 [citado 2021 Abr 22]; 80: 36-40. Available at: https://www.sciencedirect.com/science/article/abs/pii/S0020748917302845?via%3Dihub [ Links ]
12. Tanguay A, Reeves I, LeMay S, Khadra C, Gosselin E, St-Cyr-Tribble D. Survey of oral care practices in Quebec for intensive care patients receiving mechanical ventilation. Canadian Journal of Critical Care Nursing. [Internet]. 2018 [citado 2021 Abr 22]; 29(3): 39-44. Available at: https://www.caccn.ca/files/CJCCN/29-3-2018%20CJCCN.pdf#page=39 [ Links ]
13. Alja'afreh MA, Mosleh SM, Habashmeb SS. Nurses' perception and attitudes towards oral care practices for mechanically ventilated patients. Saudi Med J [Internet]. 2018 [citado 2021 Abr 22]; 39(04): 379-385. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5938652/ [ Links ]
14. Al-Zaru I, Batilha AM, Al-Talla AA, Bani YM, Alhalaiqa FN. Knowledge, attitudes, and practices of oral care in mechanical ventilated patients. Prakticky´ Le´kar [Internet]. 2020 [citado 2021 Abr 22]; 100: 5-11. Available at: https://www.researchgate.net/publication/345368721_Knowledge_Attitudes_and_Practices_of_Oral_Care_in_Mechanical_Ventilated_Patients [ Links ]
15. Ghauri, SK, Javaeed A, Chaudhry A, Khan AS, Mustafa KJ. Knowledge and attitudes of Pakistani intensive care unit nurses regarding oral care delivery to mechanically ventilated patients. J Pak Med Assoc [Internet]. 2020 [citado 2021 Abr 22]; 70(7): 1203-1208. Available at: https://pubmed.ncbi.nlm.nih.gov/32799274/ [ Links ]
16. Khasanah IH, Sae-Sai W, Damkliang J. The effectiveness of oral care guideline implementation on oral health status in critically ill patients. SAGE Open Nursing. [Internet]. 2019 [citado 2021 Abr 22]; 5: 1-9. Available at: https://journals.sagepub.com/doi/full/10.1177/2377960819850975 [ Links ]
17. Sreenivasan VP, Gangana A, Rajashekaraiah PB. Awareness among intensive care nurses regarding oral care in critically ill patients. J Indian Soc Periodontal. [Internet]. 2018 [citado 2021 Abr 22]; 22: 541-545. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6305093/ [ Links ]
18. Doshi M. Mouth Care Matters - A guide for hospital healthcare professionals - second edition. NHS - Health Education England [Internet]. 2019. [citado 2021 Abr 25]. Available at: http://mouthcarematters.hee.nhs.uk/wp-content/uploads/sites/6/2020/01/MCM-GUIDE-2019-Final.pdf [ Links ]
19. Collins T, Plowright C, Gibson V, Staut L, Clarke S, Caisley J, et al. British Association of Critical Care Nurses: Evidence-based consensus paper for oral care within critical care units. Nurs Crit Care. [Internet]. 2020 [citado 2021 Abr 25]; 1-10. Available at: https://doi.org/10.1111/nicc.12570 [ Links ]
20. Grap MJ, Martin B, Munro C. American Association of Critical-Care Nurses Practice Alert - Oral care for acutely and critically ill patients. Crit Care Nurse. [Internet]. 2020 [citado 2021 Abr 25]; 37(3): 19-21. Available at: https://doi.org/10.4037/ccn2017179 [ Links ]
Received: March 20, 2022; Accepted: October 13, 2022
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
