










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
versión On-line ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.11 no.3 may./jun. 2006
Choice of ceramic for use in treatments with porcelain laminate veneers
Selección de la ceramica a utilizar en tratamientos mediante frentes laminados de porcelana
Antonio Fons Font 1, Mª Fernanda Solá Ruíz 2,
María Granell Ruíz 2,
Carlos Labaig Rueda 1, Amparo
Martínez González 2
(1) Assistant Professor
(2) Associate Professor. Prosthodontics and Occlusion
Teaching Unit. Department of Stomatology.
Valencia University Medical and Dental
School. Valencia (Spain)
Dirección para correspondencia
ABSTRACT
Porcelain laminate veneers (PLVs) have been used for over two
decades to treat esthetic and/or functional problems, particularly in the
anterior sector (1-3). A range of dental ceramic materials are presently
available on the market for these treatments, though with very different
characteristics in terms of the composition, optic properties and manufacturing
processes involved. As a result, selection of the material best suited for the
management of each individual patient may prove complicated.
The present study proposes a simple system for selecting the
most appropriate ceramic material, based on the two variables that most
influence the esthetic outcome: the intrinsic characteristics of the substrate
tooth, and the characteristics of the ceramic material in terms of resistance
and optic properties.
Key words: Dental ceramics, porcelain classification, porcelain laminate veneers, esthetic.
RESUMEN
El tratamiento mediante Frentes Laminados de Porcelana (FLP)
se utiliza desde hace más de dos décadas para el tratamiento de problemas
estéticos y/o funcionales, particularmente en el grupo anterior de las arcadas
dentarias (1,2,3). La actual oferta en el mercado de cerámicas dentales aptas
para este tipo de tratamiento, pero muy distintas en cuanto a composición,
características ópticas y sistema de elaboración, hace complicada la selección
del material más adecuado a cada paciente en particular.
Proponemos un sistema sencillo de elección de la cerámica
teniendo en cuenta las dos variables que más influirán en el resultado estético
final: de un lado las características propias del diente (sustrato en el que nos
apoyamos), y de otro las características propias del material cerámico en cuanto
a resistencia y propiedades ópticas.
Palabras clave: Cerámica dental, estética, clasificación porcelana, frentes laminados.
Introduction
Porcelain laminate veneers (PLVs), also known as porcelain facets, Horn-type facets or ceramic facets, were first introduced in 1938 by Charles Pincus (4), who developed porcelain facets that temporarily adhered to the vestibular surface of the anterior teeth. The development of enamel adhesion techniques in the fifties, comprising the use of enamel etching by Buonocuore and the introduction of bonding resins by Bowen (5), soon made it possible to apply such PLVs to teeth on a permanent basis. Finally, in 1983, Horn (6) proposed the use of porcelain facets to cover the vestibular surface of the anterior teeth as a definitive restoration technique.
Since then the indications of this procedure have continued to expand to the point where the use of PLVs is now common practice in dental clinics. In effect, evolution of the technique and materials used has led to gradual modifications in the indications of PLVs. Thus, while in the eighties the indications were limited to the restoration of slight alterations in tooth shape and/or color, the present broad range of indications of PLVs in the anterior sector to some degree reflects the reliability of such treatment (7-11):
- Correction of alterations in tooth shape or position
- Changes in morphology in patients with microdontia or tooth transposition
- Sealing of slight to moderate diastemas
- Fractures of the incisal third
- Extensive anterior dental restoration
- Abrasions of parafunctional origin
- Enamel alterations
- Alterations in tooth color
- Anterior guide rehabilitation
- Repair of crown or bridge fractures
However, this broad range of treatment possibilities gives rise to a problem, which the present studies attempts to resolve. In effect, when dealing with this great variety of clinical situations, not all ceramics behave as required. As an example, a material designed to resolve slight alterations in the color of an incisor will be of little help in the case of anterior guide restoration in a parafunctional patient.
In order to resolve the problem of which porcelain material to use in each concrete clinical case, we propose the methodology used in our Prosthodontics and Occlusion Teaching Unit (Valencia University Medical and Dental School, Valencia Spain), based on the characteristics of the different ceramic materials and on the needs of the specific clinical problem involved.
A brief review is required of the classification of ceramic materials in order to define the best option for each concrete type of patient. Of the three possible ceramic classifications, based on sinterization temperature, composition and the manufacturing technique involved, we will focus exclusively on the composition of the material, since it offers all the information needed to resolve the problem of correct ceramic choice.
Dental ceramics classification according to composition
Dental ceramics comprise a large family of inorganic non-metal materials (12-15), and are commonly divided into two groups: silicate ceramics and oxide ceramics.
1.- SILICATE CERAMICS
The common characteristic of silicate ceramics is the presence of quartz, feldspate and kaolin the basic component being silica dioxide. These are heterogeneous materials composed of crystals surrounded by a vitreous phase (16,17). Depending on the proportions of the different components and on the raw substance grain size, a broad spectrum of ceramic materials can be produced including gres ceramics, porcelain and glass.
Based on their composition, silicate porcelains can be classified as feldspates or alumina porcelains.
1.1.- Feldspates
The predominant element in this case is silica oxide or quartz in a proportion of 46-66% versus 11-17% of alumina. The feldspate porcelains in turn are subclassified as follows:
- Conventional feldspate porcelains. These offer very good esthetic effects but the main problem is that they are fragile (low fracture resistance: 56.5 MPa). Examples include d-SING, Vintage, Luxor, Duceram, Flexoceram, Vivodent PE, IPS Classic, Empress esthetic.
- High resistance feldspate porcelains. In this case we have the following materials:
(a) Feldspate porcelain reinforced with leucite crystals. The chemical composition in this case comprises quartz (68%) and aluminum oxide (18%). As a result of the pressing process used to manufacture these materials, porosity is reduced and adequate and reproducible fit precision is achieved. The perfect distribution of the leucite crystals within the glass matrix, observable during the cooling phase and after pressing, contributes to increase resistance without significantly diminishing translucency. The resistance to flexion is 160-300 MPa (19,20). Examples of this type of porcelain include IPS-Empress I, Optec HSP, Mirage, Finesse, Cergogold.
(b) Feldspate porcelain reinforced with lithium oxide. The chemical composition in this case comprises quartz (57-80%), lithium oxide (11-19%) and aluminum oxide (0-5%). The incorporation of these crystalline particles increases the flexion resistance to 320-450 MPa, thanks to their important volume (60%), homogeneous interlocking structure of densely distributed elongated crystals, and the increase in crystal size after pressing thereby yielding a more homogeneous microstructure. These porcelains are only used to manufacture the inner coping of the restorations; the latter are in turn covered with fluor-apatite ceramics (21). Examples of this type of porcelain include IPS Empress II, Style-Press (figure 1).

1.2.- Alumina porcelains
These porcelains contain an increased proportion of alumina (40-85%), while the silica oxide concentration is reduced from 60% to 15% (22). This group is the same as the Conventional alumina porcelains. The proportion of aluminum oxide in this case does not exceed 50%. These materials are indicated for the preparation of complete crowns and for porcelain coating with aluminum oxide and metal though facets can also be manufactured. Examples of this type of porcelain include Vitadur N, Alpha Vitadur, NBK 1000, Vita Omega 900.
2.- OXIDE CERAMICS
The oxide ceramics comprise both simple oxides such as aluminum oxide, zirconium dioxide and titanium dioxide, as well as complex oxides such as spinelle, ferrite, etc. Strictly speaking, oxide ceramics contain only oxidant components, though the same term is commonly used in reference to ceramics with blended oxide components (16). These are polycrystalline materials with little or no vitreous phase the latter representing the weak point of porcelain. Due to their great opacity, they are used as internal copings in ceramic restorations.
2.1.- Aluminum oxide ceramics
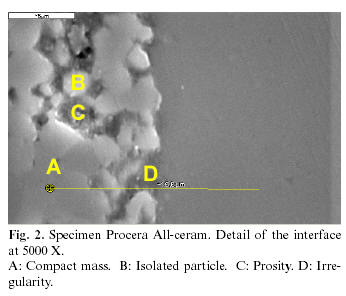
Examples of this type of porcelain include: (a) In-Ceram Alumina (85% aluminum oxide particles measuring 2-5 mm in diameter). This high alumina content affords a resistance to flexion of 400-600 MPa; (b) In-Ceram Spinelle, where the substitution of alumina with mixed magnesium and aluminum oxide affords increased porcelain coping translucency. This is attributable both to the crystalline origin of the spinelle, which confers isotropic optic properties, and to the low refraction index of the crystals; (c) In-Ceram Zirconium, comprising 67% aluminum oxide and 33% zirconium oxide and yielding a resistance to flexion of up to 600-800 MPa (23); and (d) Procera All-Ceram, developed in 1993 by Andersson and Odén (24). This material contains 99.9% aluminum oxides, with a fracture resistance of 680 MPa, and is in turn coated with conventional alumina ceramic (figure 2).
2.2.- Zirconium oxide ceramics
Zirconium oxide is a polycrystalline material with a tetragonal structure partially stabilized with yttrium oxide
The internal copings are formed by a mass of compacted and practically fused crystals thus giving rise to a near absence of porosities thanks to the core processing applied in the dental laboratory, based on CAD-CAM techniques (25-27) (figure 3).
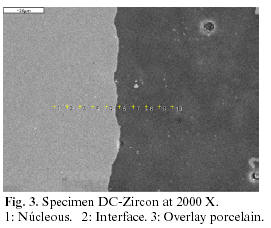
An example of this ceramic is DC-Zircon (DCS), pertaining to the CDS-Precident system and composed of 95% zirconium oxide and 5% yttrium oxide. The zirconium moreover reinforces the porcelain thanks to its great fracture modulus (900 MPa) and hardness (1200 Vickers units). Other available products are Lava and Everest.
Choice of ceramic material for manufacturing porcelain laminate veneers according to clinical indication
For correct ceramic choice, we first divide the patients in terms of the PLVs once placed in the mouth, and according to whether they are to be subjected to functional loading or not: (a) Type I patients: in these cases the facets are not exposed to functional loading, and are referred to as simple esthetic facets; (b) Type II patients: in these cases the facets are exposed to functional loading, and are referred to as functional esthetic facets.
In this context, type I patients are candidates for conventional ceramics, while type II patients require high resistance ceramics. However, this first division is incomplete, since it only contemplates aspects relating to resistance of the ceramic material without considering the optic characteristics, which are so important for ensuring good esthetic results. Type I patients are therefore in turn classified into two subgroups according to the background color characteristics of the treated teeth: (a) Type I-A patients: these are subjects programmed to receive simple esthetic facets where the substrate teeth present no color alterations. The only objective in this case is to apply PLVs for shape modifying purposes; (b) Type I-B patients: these patients are likewise programmed to receive simple esthetic facets, though in this case the substrate teeth present color alterations. Therefore, and independently of the need for shape modifications, the selected ceramic material must be able to hide the underlying substrate color.
Once the patients programmed for porcelain facet treatment have been classified, we only need to select the dental porcelain material best suited to the physical and optic requirements of each case, based on the above described material classification.
Type I-A patients
Since these are patients with facets that will not be subjected to functional loading and present a clear substrate, the material used only aims to solve problems relating to tooth shape. These are consequently favorable cases, since moreover only a small ceramic material thickness is required.
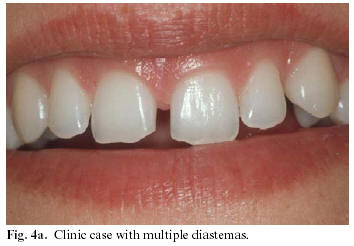
In these situations we therefore recommend the use of conventional feldspate ceramics, in view of their excellent optic characteristics that afford optimum esthetic results. The absence of occlusal stress in these cases, and the use of the currently available adhesion techniques (which improve resistance to fracture of these ceramics) contribute to ensure prolonged restoration survival (figures 4a y 4b).

The exception to the above is represented by cases in which the problem is medium or large (over 2 mm) interincisal diastemas in the presence of a clear dental substrate. In this setting it must be taken into account that as the porcelain extends beyond the adhesion zone, it loses the "protective" increase in elastic modulus afforded by the adhesion and composite resin. In these patients we therefore recommend the use of high resistance feldspate ceramics since their good esthetic qualities combine with adequate resistance to fracture.
Type I-B patients
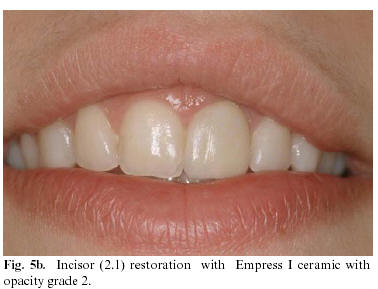
These patients present facets that will not bear functional loading but which show moderate to severe alterations in dental color that must be effectively masked by the restoration. In these situations both the porcelain and cement must present various degrees of opacity in order to hide the color alterations, and this in turn implies problems to secure the desired optic effects in terms of translucency and reflectance, and consequently also esthetic outcome (figures 5a and 5b).

Other characteristics to be taken into account in these cases refers to dental preparation, which will be more aggressive (0.8-1 mm), and to the finishing line which should be slightly subgingival and involving a curved chamfer in order to increase the ceramic thickness and prevent an overly notorious tooth-restoration transition zone (figure 6).

The materials indicated in such cases are ceramics offering the possibility of selecting the opacity of the base material, regardless of the degree of resistance.
Type II patients
In these cases the existence of functional loading in both the mandibular static position and during excursive movements requires the use of a material with great resistance to fracture. Accordingly, feldspate or alumina ceramics of high resistance, and oxide ceramics are indicated.
Consequently, we recommend the use of high resistance ceramics with the lost-wax casting technique (IPS Empress II, Style Press, IPS Empress I, Optec HSP, Mirage, Finesse, Cergogold y Empress esthetic), because of its esthetic properties and predictability, in long term studies, in the oral rehabilitation of the anterior guide (figures 7a and 7b).


Conclusions
The use of porcelain facets to solve esthetic and/or functional problems in the anterior sector has been shown to be a valid management option. Years of experience with both the technique and the materials employed offer satisfactory, predictable and lasting results.
The simple ceramic classification and definition of the types of patients amenable to ceramic facet application proposed in the present study will help the clinician to resolve the problem of selecting the ceramic material best suited to each individual case.
![]() Correspondence:
Correspondence:
Pof. Antonio Fons Font
Clínica Odontológica
C/ Gascó Oliag, 1
46010 Valencia
E-mail: Antonio.Fons@uv.es
Received: 10-11-2005
Accepted: 12-1-2006
References
1.Torrella F, Gascón F, Castañar F. Frentes Laminados de porcelana. AV Odontoestomatol 1987;3:5-15. [ Links ]
2. Calamia JR. Restauraciones de porcelana adherida de alta resistencia: anteriores y posteriores. Quintessence Int 1990;3:541-58. [ Links ]
3. Karlsson S, Landahl I, Stegersjo G, Milleding P. A clinical evaluation of ceramic laminate veneers. Int J Prosthodont 1992;5:447-51. [ Links ]
4. Pincus CR. Building mouth personality. J South Calif Dent Assoc 1938;14:125-9. [ Links ]
5. Bowen RL. Adhesive bonding of various materials to hard tooth tissues. II. Bonding to dentin promoted by a surface-active comonomer. J Dent Res 1965;44:895. [ Links ]
6. Horn HR. Porcelain laminate veneer bonded to etched enamel. Dent Clin North Am 1983;27:671-84. [ Links ]
7. Haga M, Nakazawa A. Estética dental. Carillas de porcelana. Caracas: Actualidades MédicoOdontológicas LatinoAmericanas 1991. [ Links ]
8. Cuthbirth S. Técnica indirecta de veneers de porcelana para la restauración de dientes con tinción intrínseca. J Esther Dent 1993;3:2-12. [ Links ]
9. Schmidseder J. Atlas de Odontología Estética. Barcelona: MASSON, S.A.;1999. p. 206-24. [ Links ]
10. Dumfahrt H. Facetas de porcelana. Evaluación retrospectiva después de 1-10 años de servicio: Parte I-Procedimiento clínico.Rev Int Prótesis Estomatol 2000;2:103-11. [ Links ]
11. Beltrán M, Bustos JL, González R, Solá MF. Facetas de porcelana. Revisión y actualización. Soprodent 1996;12:133-40. [ Links ]
12.Leinfelder KF, Lemons JE. Porcelain. Clinical Restorative Materials and Techniques. Philadelphia: Lea& Febiger; 1988. [ Links ]
13. Mclean JW. The Science and Arto of Dental Ceramics Vol II. Chicago: Quintessece Publ Inc; 1980. [ Links ]
14. Anglada JM, Salsench J, Nogueras J, Samsó J. Análisis de la composición de algunas cerámicas dentales. Arch Odontoest 1992;8:221-4. [ Links ]
15. Puchades O, Solá MF, Martínez A, Labaig C, Fons A, Amigó V. Estudio de la composición y estructura de las coronas completas de cerámica. Revista Internacional de Prótesis Estomatológica 2004;6:330-8. [ Links ]
16. Pröbster L. El desarrollo de las restauraciones completamente cerámicas. Un compendio histórico (I). Quintessence (ed. Esp.) 1998;11:515-9. [ Links ]
17. Tinschert J, Natt G., Mautsch W., Augthum M., Spiekermann H Fracture resistance of lithium disilicate, alumina and zirconia based three-unit fixed partial dentures: a laboratory study. Int J Prodthodont 2001;14:231-8. [ Links ]
18. Fons A, Solá MF, Martínez A, Casas J. Clasificación actual de las cerámicas dentales. RCOE 2001;6:645-56. [ Links ]
19.Wohlwend A, Schärer P. Die Empress Technik; Eine neue Möglichkeit Einzelkronen, Inalys und Verblendschalen Herzustellen. Quintessenz Zahntech 1990;16:960-78. [ Links ]
20. Bourrelly G, Prasad A. Le procédé Optec hsp concepts et mise en oeuvre au laboratoire. Les cahiers de protèse 1989;68:93-103. [ Links ]
21. Solá MF, Labaig C, Suarez MJ. Cerámica para puentes de tres unidades sin estructura metálica:Sistema IPS-Empress II. Rev Int Prótesis Estomatolog 1999;1:41-7. [ Links ]
22. McLean JW, Kedge MI. Cerámica aluminosa de colado fraccionado para restauración con coronas y puentes. Quintessence (ed esp) 1988;1:76-85. [ Links ]
23. Perelmuter S. Evolution du concept "In- Ceram". Les cahiers de protèse 1993;83:87-93. [ Links ]
24. Andersson M, Odén A. A new all-ceramic crown: A densely-sintered, high-purity alumina doping with porcelain. Acta Odontol Scand 1993;51:59-64. [ Links ]
25. Ashizula M, Kiyojara H, Okuno T, Kubota Y. Fatigue behaboir of tetragonal zirconio polycrystals (Y-TZP) containing 2 and 4 mol % Y2O3 ( Part 2). J Ceram Soc Jpn Inter Ed 1988;96:731-6. [ Links ]
26. Mörmann W.H., Bindl A. Cerec3- ein Quantensprung bei Computer-Restaurationen. Erste klinische Erfahrungen. Quintessenz.2000;51:157. [ Links ]
27. Riquier R., Girrbach K. Digident CAD/CAM para la mecánica dental. Quintessence técnica (ed. esp.). 2002;13;1:54-66. [ Links ]
28. Christensen GJ. Odontología estética a largo plazo. Quintessence Int 1990;3:45-51. [ Links ]
29. Fradeani M. Six-year follow-up with Empress veneers. Int J Perio Rest Dent 1998;18:217-25. [ Links ]
30. Dumfahrt H. Facetas de porcelana. Evaluación retrospectiva después de 1-10 años de servicio: Parte II-Resultados clínicos. Rev Int Prótesis Estomatol 2000;2:179-88. [ Links ]

