










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
versión On-line ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.11 no.6 nov./dic. 2006
Prosthetic assessment in cleft lip and palate patients: A case report with oronasal communication
Evaluación protésica en pacientes fisurados labiopalatinos. A propósito de un caso con comunicación oronasal
Silvia Sala Martí 1, Mª Dolores Merino Tessore1, Tomás Escuin Henar 2
(1) Licenciada en Odontología. Diploma de Postgrado en Rehabilitación y Prótesis Maxilofacial
(2) Profesor Titular de Oclusión y Prostodoncia. Director del Master en Rehabilitación y Prótesis Maxilofacial.
Facultat dOdontologia. Universitat de Barcelona
ABSTRACT
The cleft lip and palate patient is mainly characterized by the presence of an oronasal communication, malformation or agenesis of the teeth close to the cleft, and deficient sagittal and transverse growth of the maxilla.
These patients require various treatments involving a multidisciplinary team, which may include a maxillofacial surgeon, an orthodontist, a speech therapist, a paediatrician, a general dentist, a prosthodontist, an ENT specialist, a psychologist and all those professionals who can help provide functional, aesthetic and psychological improvement.
This report describes a case of prosthetic rehabilitation in a patient with cleft lip and palate and an oronasal fistula (communication) following surgery. Different prosthetic treatments are described, with emphasis being placed on the approach chosen after to discuss the various limitations which arose.
Key words: Cleft lip and palate patient, oronasal communication.
RESUMEN
El paciente fisurado labiopalatino se caracteriza principalmente por la presencia de una comunicación a nivel de la cavidad oronasal, la malformación o la agenesia de los dientes cercanos a la hendidura y un deficiente crecimiento sagital y transversal del maxilar.
Dadas estas características, este paciente precisa diferentes tratamientos en los que intervendrá un equipo multidisciplinario que podrá estar formado por el cirujano maxilofacial, el ortodoncista, el logopeda, el pediatra, el odontólogo general, el prostodoncista, el otorrinolaringólogo, el psicólogo y todos aquellos profesionales que colaboren en proporcionar una mejora funcional, estética y psicológica.
El objetivo de este artículo es exponer un caso clínico de rehabilitación protésica en un paciente que presenta fisura labiopalatina y una fístula (comunicación) oronasal tras tratamiento quirúrgico. Se expondrán posibles tratamientos para la solución protésica, haciendo principal hincapié en el tratamiento elegido para el caso, teniendo en cuenta las diferentes limitaciones que se han presentado.
Palabras clave: Fisurado labiopalatino, comunicación oronasal.
Introduction
The prevalence of cleft lip and palate among the general population depends on racial, ethnic and geographic origin, as well as on socio-economic status. It has been estimated to range from 1:500 to 1:2500 live births (1, 2). Cleft lip occurs in 20-30% of cases, cleft lip and palate in 35-50% and cleft palate alone in 30-45% (3).
The aetiology is complex and depends on genetic and environmental factors (1). Some authors (1, 3) argue that the cleft palate is caused by an alteration in the normal fusion process. They also identify other factors such as a defect in vascular supply to the region involved, a mechanical alteration in tongue size, intoxication with substances such as alcohol, drugs or toxins, and infections or lack of development. In contrast, some authors (3) attribute it to a serious defect produced by a mutant gene, or a small defect caused by several genes.
In terms of physiopathology several authors have found dental anomalies in these patients, and report a variation in the number of teeth and their position, as well as a reduction in teeth size (1, 2, 4-6), the presence of root and crown malformations, and even a delay in tooth development (5). As regards morphological anomalies there is a predominance of enamel hypoplasia (6).
In the cleft lip and palate patient who requires treatment for functional and/or aesthetic reasons, it is necessary to take into account the periodontal state of the teeth present in the mouth. The teeth next to the cleft often show an alveolar ridge defect and it can be difficult to correct the periodontal lesions (2,7). This situation is usually made worse by poor plaque control (8), the presence of gingivitis and the loss of bone support, which is heightened in patients with systemic problems or immune deficits; this is evident in the case described here, in which the patient suffered from cerebral palsy. Furthermore, the poor plaque control is determined by badly positioned teeth, a defect in arch length and a crossed bite, all of which are characteristic features of these patients.
The surgical repair of soft tissue creates a short lip that, together with the orthodontic treatment, may produce additional periodontal trauma for the remaining teeth (7).
The treatment of cleft lip and palate patients is multidisciplinary and requires the involvement of a surgeon, orthodontist, speech therapist, paediatrician, general dentist, prosthodontist, laboratory technician, ENT specialist and psychologist (4, 9, 10).
All these problems caused by abnormal growth and development require early medical and surgical intervention. Surgical treatment starts at around the age of two-to-three months, in order to shift the protruding premaxilla to a more distal position and thus aid sucking (10). At one or two years of age the cleft palate is repaired to reduce the joint abnormalities associated with speech, eating and drinking (3, 10). The stage of early mixed dentition is characterized by increased discrepancy in the size of the maxilla and the mandible, a palate collapsed resulting into a crossed bite, a retruded premaxilla due to a non-elastic lip, and a shallow palate caused by the inadequate tongue position (10).
Case report
We present a thirty-seven-year-old woman with cerebral palsy and a cleft lip and palate who has been treated surgically, but remains an oronasal fistula. Skeletal and dental class III malocclusion was observed; teeth 1.2, 1.1, 2.1 and 2.2 in the anterior sector and tooth 16 in the posterior were missing (Figure 1).

Prosthetic treatment involved two stages: a provisional treatment followed by a definitive prostheses.
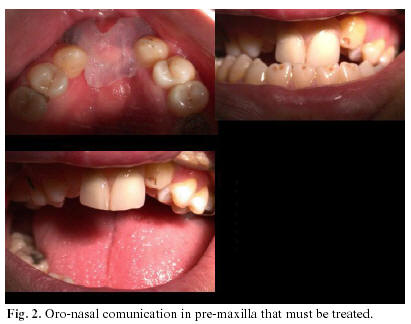
- Primary or provisional treatment (Figure 2)
The objective here was to seal the oronasal communication and stabilize the margins of the defect by inserting a temporary obturator, as well as replacing the missing teeth with provisional, partial and removable resin prostheses.
This was followed by an aesthetic and functional re-assessment, which revealed the passage of liquids through the nose. This problem was addressed by making a new impression with a tissue conditioner to improve the fit. After immersion in super-hard plaster the countercast was made to obtain a stone part like a flask box. Post-insertion monitoring showed a satisfactory level of watertightness.
The definitive therapeutic possibilities were:
Partial, removable metal prosthesis with a separated silicone obturator.
Fixed prostheses with abutment teeth in 1.4, 1.3, 2.3, 2.4 and 2.5 with a silicone obturator (separately).
Maryland bridge with a silicone obturator (separately): this was the chosen treatment.
- Definitive treatment (Figure 3)
Definitive silicone impressions were taken, without preparing the abutment teeth. The structure was then polished and tested once fitted in the mouth. Finally, the teeth were modelled in resin and cemented with a dual resin cement.

- Evolution of the case
Follow up at one year revealed that the resin veneer had come away from the first upper-right premolar, possibly due to excessive occlusal contact or lack of mechanical retention for the resin. Therefore, further retentions were made in the metallic structure and a composite veneer was created. The occlusion was also checked in order to avoid excessive occlusal contact.
When the patient attended for the eighteen-month follow-up the resin veneers had come away from the 1.1, 2.2 and 2.3 teeth. These veneers were rebuilt, after spraying the metallic structure with a priming agent and composite. The occlusion was once again monitored to avoid excessive contact.
In the final, two-year follow up, the patient presented with no veneers on the 1.2, 1.1, 2.2, 2.3 and 2.4 teeth, and these were subsequently repaired. The silicone obturator continued to be operative.
Discussion
Following surgery to close a cleft lip and palate, an oronasal fistula may remain in the palate (in the alveolar process or the labial vestibule) and cause problems with chewing, phonation, swallowing and breathing.
Normally, the alveolar cleft receives a bone graft during the mixed dentition stage (9, 11), prior to the emergence of the canine teeth and orthodontic closure. However, this closure was not done in this patient, and neither had Lefort I orthognatic surgery been performed (4, 11). This problem was resolved by using a silicone palate obturator to seal the communication (3, 4, 9).
A number of limitations were considered when fitting this obturator. Firstly, as it is a fixed bridge it was necessary to create enough space between the obturator and the pontic teeth to enable correct insertion and removal. Secondly, enough space was left to enable subsequent impressions to be taken in order to insert new obturators. And thirdly, the obturator was designed in such a way as to make it easy to insert, as the fact the patient suffered from cerebral palsy could influence the degree of treatment compliance. To resolve these problems the pontic region of the structure was given a concave shape, while the obturator was made of flexible material so that it was readily adaptable to the communication.
Prosthetic rehabilitation
Some authors (11-13) prefer a fixed prosthesis as the treatment of choice, despite the fact that removable prostheses are indicated in patients with various clefts (3, 5), and in those with a soft palate dysfunction or an uncoordinated nasopharyngeal response that produces hypernasal speech (5); overdentures are considered to be better than complete dentures as they have better retention and preserve the alveolar bone (12, 13).
In our patient a fixed bridge could have been fitted from the upper-right premolar to the upper-left premolar, with possible endodontic treatment of some of the affected teeth, in order to improve the skeletal class III malocclusion. However, given limiting factors such as the patients cerebral palsy, her lack of collaboration and the poor oral hygiene (8), and taking into account other factors such as her financial resources, another prosthetic solution had to be sought. Therefore, we opted for a modified Maryland resin bonded bridge, which offered the usual characteristics in terms of functionality and aesthetics. In cases of poor collaboration, patients often must to be sedated or receive a general anaesthesia in a dental hospital (14), but this was not required in the present case and thus was another reason why we chose this kind of prosthesis. The treatment was also chosen due to the ease of carrying out repairs in the event of fracture: they can be performed simply and directly in the mouth and in a single session.
Adhesive bridges may also be a suitable prosthetic treatment on occasions, when implants cannot be used due to the lack of alveolar bone (4, 15).
Some authors (15) have bonded Maryland bridges to the teeth next to the cleft in order to achieve skeletal stability, and this has produced acceptable results with correct stability, function and periodontal health. This approach has not been associated with a loss of cement from the adhered bridge, the weak point being the metal-composite interface.
In our patient the Maryland bridge and the silicone obturator helped to separate the oral from the nasal cavity, replaced missing teeth and improved the occlusal pattern.
References
1. Slayton RL, Williams L, Murray J, Wheeler JJ, Lidral AC, Nishimura CJ. Genetic Association Studies of Cleft Lip and/or Palate with Hypodontia Outside the Cleft Region. Cleft Palate-Craniofac J 2003;4:274-9. [ Links ]
2. Ohyama T. Prosthodontic considerations for patients with cleft lip and palate. Int Dent J 1986;36:140-5. [ Links ]
3. Abadi B, Johnson JD. The prosthodontic management of cleft palate patients. J Prosthet Dent 1982;48:297-302. [ Links ]
4. David M, Bou Saba S, Delatte M, De Clerck H. Multidisciplinary Treatment of an Adult Patient with a labiopalatal cleft. J Clin Orthod 2000;34:667-71. [ Links ]
5. Hochman N, Yaffe A, Brin I, Zilberman Y, Ehrlich J. Functional and esthetic rehabilitation of an adolescent cleft lip and palate patient.Quintessence Int 1991;22:401-4. [ Links ]
6. Shapira Y,Lubit E,Kuftinec MM,DStom.Congenitally missing second premolars in cleft lip and cleft palate children. Am J Orthod Dentofacial Orthop 1999;115:396-400. [ Links ]
7. Schultes G, Gaggl A, Kärcher H. Comparision of Periodontal Disease in Patients with Clefts of Palate and Patients with Unilateral Clefts of Lip, Palate, and Alveolus. Cleft Palate-Craniofac J 1999;36:322-7. [ Links ]
8. Gimenez-Prats MJ, Lopez-Jimenez J, Boj-Quesada JR. An epidemiological study of caries in with cerebral palsy. Med Oral 2003;8:45-50. [ Links ]
9. Reisberg D J. Dental and Prosthodontic Care for Patients with Cleft or Craniofacial Conditions. Cleft Palate-Craniofac J 2001;37:534-7. [ Links ]
10. Sapp B, Quinn Galen, Pickrell Kenneth.Treatment of cleft lip and palate patients.J Prosthet Dent 1972;28:66-75. [ Links ]
11. Jansma J,Raghoebar G,Batenburg R, Stellingsma C. Bone grafting of cleft lip and palate patients for placement of endosseous implants. Cleft Palate-Craniofac J 1999;36:67-72. [ Links ]
12. Wegscheider W, Bratschko R, Plischka G, Haas M, Permann R, Parsche E. The System of Prosthetic Treatment for Clap Patients. J Cranio Max Fac Surg 1989;17:49-51. [ Links ]
13. Pigno MA, Blackman RB, Cronin RJ, Cavazos E. Prosthodontic management of ectodermal dysplasia: A review of the literature. J Prosthet Dent 1996;76:541-5. [ Links ]
14. Yilmaz S, Özlü Y, Ekuklu G. The effect of dental training on the reactions of mentally handicapped childrens behavior in the dental office. J Dent Children 1999;66:188-92. [ Links ]
15. Holtgrave E.A, Subotic V, Krüger E, Drescher D, Lücke M. Stabilization of maxillary segments and dental arch after puberty, in cleft lip and palate cases. J Cranio Max Fac Surg 1989;17:45-8. [ Links ]
![]() Correspondence:
Correspondence:
Dra. Silvia Sala Martí
Facultat dOdontologia. Universidad de Barcelona.
c/ Feixa Llarga s/n. 08907 LHospitalet de Llobregat. Barcelona
E-mail: tomasescuin@ub.edu.
Received: 16-01-2005
Accepted: 5-09-2006

