










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
On-line version ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.11 n.6 Nov./Dec. 2006
Assessment of PFA-100 system for the measurement of bleeding time in oral surgery
Valoración del sistema PFA-100 para la determinación del tiempo de hemorragia en cirugía oral
Juan José Arrieta Blanco1, Begoña Bartolomé Villar 2, Antonio Juzgado3, Rosa Mourelle Martínez4
(1) Stomatologist. Associate Chief of Stomatology Service
(2) Stomatologist. Associate Professor of Odontology of the Universidad Europea
(3) Odontologist UCM. Post-graduate in Medicine and Oral Surgery, Stomatology Service, Fundación Jiménez Díaz
(4) Stomatologist. Associate Professor of Odontopediatrics Universidad Complutense. Madrid
ABSTRACT
The common diagnostic methods to know primary hemostasis have been classified as invasive, depending on the operator, difficult to reproduce and at times not very reliable. Thus, different systems have been proposed to assess bleeding time, one of them being the PFA-100 device, which we present in this paper.
Objective: Compare specificity between the traditional Ivy method with the PFA-100 system to measure bleeding time.
Material and method: We obtained a sample of 33 patients between the age of 24-80 years receiving anti-platelet treatment who needed to undergo oral surgery. Bleeding time was obtained by the Ivy method, an INR by an analysis done on the same day and a Coagucheck one hour before surgery as well as measurement of bleeding time with the PFA-100 system.
Results: Mean value of bleeding time through the Ivy method was 406.36 sec.. Mean bleeding time with the PFA-100 system for the collagen/epinephrine cartridge was 226.91 sec. and for the collagen/ADP cartridge was 110.27 sec.. All these values were within normality. We observed very high standard deviations with the Ivy method and more regular ones for the PFA-100 system, indicating its greater specificity. We also obtained a large correlation between collagen/epinephrine cartridge and acetylsalicylic acid.
Conclusions: We found greater specificity of the analyzer of PFA-100 platelet function for the measurement of bleeding time in relationship with the traditional Ivy method.
Key words: PFA, bleeding time.
RESUMEN
Los métodos diagnósticos habituales para conocer la hemostasia primaria han sido calificados como cruentos, dependientes del operador, de difícil reproducción y en ocasiones no muy fiables. Es por ello que se han propuesto diferentes sistemas para valorar el tiempo de hemorragia, siendo uno de ellos el dispositivo PFA-100, el cual presentamos en este trabajo.
Objetivo: Comparar la especificidad entre el método tradicional Ivy con el sistema PFA-100 para la determinación del tiempo de hemorragia.
Material y método: Obtuvimos una muestra de 33 pacientes de entre 24-80 años en tratamiento antiplaquetario a los cuales se debía realizar una cirugía oral. Se les realizó un tiempo de hemorragia mediante el método Ivy, un INR mediante una analítica realizada el mismo día y un Coagucheck una hora antes de la cirugía así como la determinación del tiempo de sangrado mediante el dispositivo PFA-100.
Resultados: El valor medio del tiempo de hemorragia mediante el método Ivy fue de 406.36 sg. El tiempo de hemorragia medio con el sistema PFA-100 para el cartucho de colágeno/epinefrina fue de 226.91 sg. y para el cartucho de colágeno/ADP fue de 110.27 sg. Todos estos valores se encuentran dentro de la normalidad. Observamos desviaciones típicas muy altas con el método Ivy y más regulares para el sistema PFA-100 indicando una mayor especificidad del mismo. Obtuvimos también una gran correlación entre el cartucho colágeno/epinefrina y el ácido acetil salicílico.
Conclusiones: Encontramos una mayor especificidad del analizador de función plaquetaria PFA-100 para la medición del tiempo de hemorragia en relación con el método tradicional Ivy.
Palabras clave: PFA, tiempo de hemorragia.
Introduction
Currently, and thanks to the increase of well-designed randomized clinical studies that establish their indication, optimum dose and duration of administration, efficacy of the platelet antiaggregant agents has been confirmed in the prevention and treatment of thromboembolic disease (1). In the last decade, the treatment regime with aspirin has become enormously popular (2, 3). The number of patients who come to our out-patient clinic with antiaggregant treatment as therapy for cardiovascular and peripheral vascular diseases, such as, for example, ischemic heart disease, valvular prosthesis, venous thrombosis, etc., is increasingly greater. Furthermore, there is an increasing majority opinion not to suspend anticoagulant or platelet antiaggregant treatment before the surgical intervention in the oral cavity (3-5). Thus, when certain odontologic procedures are done, it is very important to measure bleeding times of these patients in order to predict the possibilities of future bleeding and thus if this oral procedure should be done or not.
In recent years, the protocols on oral surgery procedures have undergone significant variations, modifying the medical treatments of the patients based on the surgery times obtained from an analysis: bleeding time, protombin time, tissue thromblastin time and INR. It must be added to this that the usual diagnostic methods to know primary hemostasis do not offer a simple, rapid and reproducible possibility on the platelet function (6-9). Assessment of primary hemostasis is very important not only for the diagnosis and management of patients with platelet disorders but also to measure the efficacy of antiaggregant therapy.
Bleeding time is that used to determine platelet function. The usual platelet tests are laborious and take time to do. The most frequent procedure used is the Ivy method (6). However, this is an invasive procedure that may be affected by different factors, that is not always well-accepted by the professionals and patients and that has many deficiencies (6, 9). That is why we present the Platelet Function Analyzer PFA-100 capable of measuring bleeding time in a few minutes, that can be an effective and comfortable alternative to the traditional methods as it is a simple method for the investigation of primary bleeding (10).
Platelet activation
They are several factors involved in the regulation of platelet thrombus formation. After the vascular lesion, platelets adhere to the subendothelium exposed through the von Willebrand factor that is bond to the glycoprotein Ib (GPIb) of the platelet membrane. After the adhesion and subsequent activation, they secrete the content of their granules, producing platelet aggregation. This is a metabolic process in which the agonists released (thrombin or ADP) bind to their receptors on the surface of the platelets and stimulate them to expose binding sites for fibrinogen through GPIIb/IIIa. This also causes activation of the nearby platelets (3).
Furthermore, the modified membrane of the activated platelets is exposed as a surface where the coagulation process takes place, generating thrombin as a final result which is, in turn, a powerful activator of the platelets. Finally, another important fact in clot formation is the production of thromboxane A2 by the platelets, a result of arachidonic acid metabolism, a potent vasoconstrictor and platelet agonist.
The inhibitors of platelet function or antiaggregants block some or several of the previously mentioned mechanisms.
Presentation of PFA-100 system
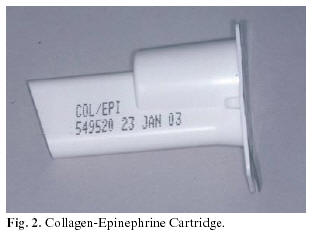
This is an improved device of Thrombostat 400 originally developed by Kratzer and Born in 1985 (8, 11-13). The platelet function analyzer PFA-100 (Fig. 1) simulates in vitro primary hemostasis in peripheral blood by a lesion of the membrane with collagen/ADP or collagen/epinephrine. This membrane, coated by approximately 50 mg of ADP and 10 mg of epinephrine, is protected in some cartridges perfectly identified with the initials COL/EPI or COL/ADP (Fig. 2). Collagen, epinephrine and ADP are, under in vivo physiological conditions, substances that favor platelet adhesion and aggregation.

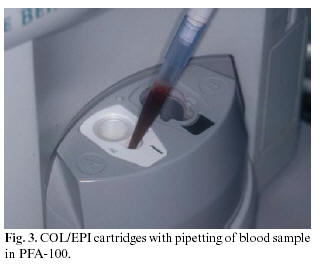
The system makes it possible two place both cartridges or one alone. Eight ml of the uncentrifuged blood sample must be pipetted in the smallest aperture of the cartridge, whole blood that should be collected in sodium citrate at 3.8%-3.2%, used as anticoagulant (Fig. 3). When the device begins to process the sample, the blood is aspirated through a capillary towards the membrane (with a lesion of approximately 150 mm of aperture), crossing the orifice located in its center at an elevated speed (5000-6000/s). The analyzer calculates the time it takes to close the membrane lesion (CT) and thus measures the platelet function. The results are seen on the analyzer display and on printed paper that comes from the upper part of the apparatus.
Maximum times for the closure of the membrane lesion are between 94-180 sec. for the collagen/epinephrine cartridge and between 71-119 sec. for the collagen/ADP one.
Above these maximum times, the patients platelet function would be altered. Thus, PFA can measure if the platelet function is normal, altered or even if it does not finally produce any closure. Closure times for healthy children are generally longer than in adults but are not significant. However, neonates have significantly lower times than healthy children (6). The times in hemophilic patients are normal, indicating that factors 8 and 9 of coagulation are not involved in the formation of platelet plug formation (6, 14).
The typical pattern in patients antiaggregated with aspirin, of which the system is very specific, is: prolonged collagen/epinephrine and normal collagen/ADP (6, 8, 9, 11, 12). Thus, the col/epi cartridge is generally used to detect congenital platelet dysfunctions (e.g.: Von Willebrand disease) and patients under treatment with aspirin while the col/ADP cartridge generally confirms dysfunction not due to ASA (15).
Basically, the strongest factor involved in this system will be factor vW, primarily producing platelet adhesion by the Wf/FPIb system and later on the formation of the plug would involve vWF interaction with GPIIb/IIIa.
Most of the studies reviewed agree that PFA-100 is a simple, real and reproducible method to measure in vitro platelet function (6, 8, 9, 11, 12, 14, 16-18): Only Marshall et al. do not observed any advantage over the traditional method (13). Furthermore, PFA-100 is useful to evaluate platelet function in adults and above all in children. It is an excellent method of screening in patients with von Willebrand disease and in patients antiaggregated with aspirin.
Objectives
Compare the traditional method of Ivy with the PFA-100 device in order to determine which one is most specific when analyzing the platelet function.
Discover if the specific pattern of aspirin in the PFA-100 analyzer is valid for any other platelet antiaggregant.
Material and methods
A protocol was established to study the influence of platelet antiaggregants in oral surgical procedures, assessing bleeding time with two different methods: the traditional Ivy method and the PFA-100 system. The study was conducted in the Stomatology Service of the Fundación Jiménez Díaz on 33 patients whose ages ranged from 24-80 years in whom an oral surgical intervention had to be done. The patients were randomly distributed into two groups: one control group that interrupted antiaggregant treatment seven day before surgery and an experimental group that continued the therapy regularly. All the interventions were always done by the same surgeon.
- The enrolment criteria were:
The patient should receive antiaggregant therapy regularly and continuously regardless of his/her age, gender, race, antiaggregant type or treatment dose.
Patient who, fulfilling the previous condition, had to undergo a surgical act in the oral cavity.
- The exclusion criteria were:
Patients who also receive anticoagulant therapy.
Patients in whom an abnormality is detected in coagulation time, that is, INR greater than 1.15.
Patients with anemia with hemoglobin values under 100g/l.
All the patients who agreed to collaborate in the study had to sign the corresponding informed consent. In the presurgical visit, a complete clinical history was obtained, including routine blood and biochemistry analyses, orthopantomography and intraoral x-rays in order to assess the surgery type and provide pre-operative guidelines.
The prophylactic measures necessary were adopted based on the patients general condition. If bacterial endocarditis prophylaxis was necessary, 2 grams of oral amoxicillin were administered one hour before the surgical procedure. Patients allergic to penicillin received 600 mg of oral Clindamycin one hour before surgery.
Bleeding time and INR were obtained in all the patients one hour before the surgical procedure. Bleeding time was measured with the Ivy method and PFA-100 system. The INR was measured with an analysis conducted on the same day of the surgery and with the Coagucheck device one minute before the operation. The Ivy method was conducted in the Hematology Service of the Fundación Jiménez Díaz, making a small incision in the anterolateral surface of the forearm with an automated template, maintaining a pressure of 40 mmHg with the sphingomanometer. A filter paper was used every 15 to 30 seconds to collect the blood from the incision, but without entering into contact with it. Normal was considered to be between 180-540 sec (3-9 mn). All the data were recorded in the corresponding record of the patient
- Statistical method: The study of the discreet endpoints was done by frequency measured by contingency tables. We applied Pearsons Chi-square to observe the existence or non-existence of significant differences in the different tables and correlations studied. Significance level is for p<0.05.
Results
The study sample was made up of 33 patients, 7 women and 26 men, whose ages ranged from 24 to 80 years with mean age of 67.12 years (68.33 years in the control group and 66.66 years in the experimental group). Both groups can be considered homogeneous regarding the patients age (p= 0.756).
In regards to the type of platelet antiaggregant, only one patient (3%) was receiving treatment with acetylsalicylic acid (ASA) 100, 2 patients (6.1%) with ASA 150, 20 patients (60.6%) with ASA 300, 5 patients (15.2%) with clopidogrel and 5 other patients with ticlopidine. The patients also had a homogeneous distribution in both groups in regards to the type of antiaggregant they were taking (p= 0.238).
Bleeding time, measured with the Ivy method, had a mean value of 406.36 seconds (6.77 minutes): 353.33 seconds (5.88 minutes) in the control group and 426.25 seconds (7.10 minutes) in the experimental group. Although, as was to be expected, bleeding time according to the Ivy method was greater in the experimental group, its values were found to be within the normality parameters (180-540 seconds: 3-9 minutes). The statistical difference between the two groups was not significant (p=0.200).
Mean collagen/epinephrine bleeding time was 226.91 seconds: 176 seconds in the control group and 246 seconds in the experimental group (both within normality parameters: 94-180 seconds). The difference between the two groups was significant (p=0.016). Mean collagen/ADP bleeding time was 110.27 seconds: 99.44 in the control group and 114.33 seconds in the experimental group (normality parameters between 71-119 seconds).
Both in the control group and experimental one, we found very low and very high Ivy times. On the one hand, its p is equal to 0.200 (p>0.05), that is, the difference between both groups in relationship to bleeding time obtained by the Ivy method is not significant. Thus, we can state, a priori, that the Ivy method is not an adequate system when measuring bleeding time. It is a method with little specificity.
In table 1, we can see how the standard deviation is not as high for the bleeding times measured in both groups with the collagen/epinephrine cartridges. The times tend to be within normal parameters for the control group and above the maximum value considered as normal in the experimental group. After the statistical analysis, we found p=0.016 (p<0.05), that is, it is a very specific system to measure bleeding time. Regarding bleeding time measured with collagen/ADP cartridges, the mean values in both groups were within normal parameters.
In regards to the correlations, we found the most important correlation between the times obtained with collagen/epinephrine and collagen/ADP. When the time obtained with the col/epi cartridge is low or within normal limits, the time obtained with the col/ADP one would follow the same line. However, when the col/epi time is high (above the maximum considered normal), the col/ADP time will continue to be within normal parameters, although closer to the maximum limit. This correlation becomes more obvious when only those patients under treatment with ASA are included in the chart (Table 2).
When the same charts are done including in one of them only those patients under treatment with clopidrogel and in the other only those treated with ticlopidine, we observe that there is a tendency to follow the same pattern as for aspirin, although the number of patients in the study under treatment with these two antiaggregants is still scarce.
Discussion
PFA-100, as we have described, is a method that has been demonstrated to be effective fundamentally for the assessment of antiaggregated patients and for the diagnosis of hereditary platelet dysfunctions: von Willebrank disease, Glanzmann thrombasthenia and Bernard-Soulier syndrome (18-21) but less effective in patients with unknown hemostatic disorders, bleeding time being even more sensitive in these (20). The protein most involved in platelet aggregation by this system is factor vW. This interacts with the platelet glycoprotein Ib/IX and IIb/IIIa receptors. Meanwhile, it has been demonstrated how fibrinogen practically does not exert any function (8, 12, 14, 15, 18, 22), perhaps due to the elevated speeds acquired through the membrane (5000-6000/s).
For the study of bleeding time, we have not found any study whose objective is to assess the repercussion of the antiaggregants in the oral surgical procedures by using the PFA-100 system. The studies and cases consulted (3, 5, 23-26) use the traditional methods, fundamentally the Ivy method. However, there are abundant studies applied to other fields of medicine that consider PFA as a rapid method, a simple one that does not require qualified operators, with low cost and with extensive advantages: use of whole blood, obtaining of results in real time (approximately 10 mm), accuracy of measurements and use of small amounts of blood (0.8 ml per cartridge), which makes it very useful in pediatric patients (6, 8, 12, 22). Compared to this, the disadvantages presented by the traditional methods have been indicated. These are: being extremely dependent on the operator, being invasive (difficulty in pediatric patients), they may not predict bleeding time in presurgical patients, they may offer normal values in presence of severe abnormalities and may be difficult to reproduce (6,9). Thus, the PFA has been indicated as a useful screening method, although it may have certain limitations. Blood should only be treated with citrate and not with PRP. The results may vary according to the citrate concentrations (closure time decreases when the citrate concentrations are lower) or according to the grade of the calcium chelate of the anticoagulant (11), existence of a correlation between hematocrit and closure time with epinephrine (9) and low hematocrits (<30%) and that decreased platelet counts (<50 109/1) could result in a prolongation of closure time (14). Furthermore, it may not be as sensitive in detecting ADP platelet antagonists (27), showing a relative utility in this field, being a mere complement to the aggregometry (21).
In our study, after analyzing the results, we agree with other authors that the Platelet Function Analyzer is more specific and reliable than the Ivy method to determine bleeding time (6, 8, 9, 11-14, 16-19, 28). However, authors such as Marshall et al. find equal sensitivity and reproducibility of PFA in relationship with the Ivy method. They also claim that the device may provide slightly superior results than those expected, which they interpret as false positives (13). Another study (29) states how a significant proportion of patients under treatment with ASA show a normal platelet function measured by PFA, the elderly and women being the most prone to show a decreased therapeutic response to aspirin.
We also agree that the typical pattern in patients antiaggregated with ASA is prolonged col/epi and col/ADP within the normality limits (6, 8, 11, 12). However, it must be stated that mean time of collagen/epinephrine in the control group patients (whose treatment was temporally interrupted) was very close to the maximum parameter. This could explain why the antiaggregant was withdrawn 7 days before the extraction. However, we know that these drugs produce an irreversible action on the platelets, whose half life is 9-10 days. An alteration in the col/APD cartridge in patients treated with aspirin would indicate a platelet alteration having high severity (12).
In spite of the limited sample of our study regarding patients who took clopidogrel (5 patients) and ticlopidine (5 more), we observe that there is a tendency to follow the same pattern as acetylsalicylic acid. Some authors (11, 30) do not find significantly altered values in patients treated with ASA/Ticlopidine or ticlopidine alone in the PFA method. However, they do find a prolongation in platelet aggregation with ADP. However, a longer closure time with clopidrogel was found with the PFA system (30).
Conclusions:
- The platelet function analyzer PFA-100 is more specific and less invasive to measure bleeding time than the traditional method of Ivy.
- The PFA-100 is a very specific device for ASA, with which a characteristic pattern is followed.
- Investigation should continue in relationship to its efficacy in patients treated with other platelet antiaggregants other than ASA and its response pattern regarding them should be identified.
References
1. Bañas Llanos. Nuevas prespectivas en el tratamiento antitrombótico. Información Terapeútica del Sistema Nacional de la Salud 2001; 25: 93-104. [ Links ]
2. Bada MA, Zudaire MT, Etayo A, Palomero R. Manejo en cirugía oral del paciente con tratamiento anticoagulante o antiagregante. Archivos de Odontoestomatología 2001;17:43-6. [ Links ]
3. Ardekian L, Gaspar R, Peled M, Brener B, Laufer D. Does low-dose aspirin therapy complicate oral surgical procedures? JADA 2000;131:331-5. [ Links ]
4. Vicente Barrero M, Knezevic M, Tapia Martin M, Viejo Llorente A, Orengo Valverde JC, García Jiménez F, et al. Oral Surgery in patients unergoing oral anticoagulant therapy. Med Oral 2002;7:63-6, 67-70. [ Links ]
5. Gaspar R, Ardekian L, Brenner B, Peled M, Laufer D. Ambulatory oral procedures in patients on low-dose aspirin. Harefuah 1999;136:108-10. [ Links ]
6. Carcao MD, Blanchette VS, Dean JA, He L, Kern MA, Stain AM, et al. The Platelet Function Analyzer (PFA-100): a novel in vitro system for evaluation of primary haemostasis in children. Br. J Haematol 1998;101:70-3. [ Links ]
7. De Caterina R, Lanza M, Manca G, Strata GB, Maffei S, Salvatore L. Bleeding time and bleeding: an análisis of the relationship of the bleeding time test with parameters of surgical bleeding. Blood 1994;84:3363-70. [ Links ]
8. Harrison P, Robinson MSC, Mackie IJ, Joseph J, McDonald SJ, Liesner R, et al. Performance of the platelet function analyzer PFA-100 in testing abnormalities of primary haemostasis. Blood Coagulation and Fibrinolysis 1999;10:25-31. [ Links ]
9. Francis J, Francis D, Larson L, Helms E, García M. Can the Platelet Function Analyzer (PFA-100) test substitute for that template bleeding time in routine clinical practice?. Platelets 1999;10:132-6. [ Links ]
10. Mimidis K, Papado poulos V, Kartasis Z, Baka M, Tsatlidis V, Bourikas G, et al. Assessment of platelet adhesiveness and aggregation in mild and acute pancreatitis using the PFA-100 system. JOP 2004;5:132-7. [ Links ]
11. Kottke-Marchant K, Powers JB, Brooks L, Kundhu S, Christie DJ. The effect of antiplatelet drugs, heparin and preanalytical variables on platelet function detected by the Platelet Function Analyzer (PFA-100). Clin Appl Thrombosis/Hemostasis 1999;5:122-30. [ Links ]
12. Kundhu SK, Heilman EJ, Sio R, García C, Davidson RM, Ostgaard RA. Description of an in vitro Platelet Function Analyzer PFA-100. Seminars in Thrombosis and Hemostasis 1995;21:106-112. [ Links ]
13. Marshall PW, Williams AJ, Dixon RM, Growcott JW, Warburton S, Armstrong J, et al. A comparison of the effects of aspirin on bleeding time measured using the Simplate method and clousure time measured using the PFA-100, in healthy volunteers. Br J Clin Pharmacol 1997;44:151-5. [ Links ]
14. Fressinaud E, Veryradier A, Truchaud F, Martin I, Boyer-Neumann C, Trossaert M, et al. Screening for von Willebrand disease with a new analyzer using high shear stress: A study of 60 cases. Blood 1998;91:1325-31. [ Links ]
15. Hézard N, Metz D, Nazeyrollas P, Droulle Ch, Elaerts J, Potron G, et al. Use of the PFA-100 apparatus to asses platelet function in patients undergoing PTCA during and after infusion of cE3 in the presence of other antiplatelet agents. Thromb Haemost 2000;83:540-4. [ Links ]
16. Kundu SK, Akkerman J, Christie D, Comp P, Fressinaud E, Greenberg C, et al. Clinical performance of the Platelet Function Analyzer PFA-100. Blood 1996;88:52. [ Links ]
17. Kundu SK, Heilmann EJ, Sio R, García C, Ostgaard RA. Characterization of an in-vitro Platelet Function Analyzer PFA-100. Clin. Appl. Thrombosis/Hemostasis 1996;2:241-9. [ Links ]
18. Poujol C, Nurden A, Paponneau A, Heilmann E, Nurden P. Ultrastructural analysis of the distribution of von Willebrand factor and fibrinogen in platelet aggregates formed in the PFA-100. Platelets 1998;9:381-9. [ Links ]
19. Posan E, Mc Bane RD, Grill DE, Motsko CL, Nichols WL. Comparison of PFA-100 testing and bleeding time for detecting platelet hypofunction and von Willebrand disease in clinical practise. Thromb Haemost 2003;90:483-90. [ Links ]
20. Quirogat T, Goycoolea M, Munoz B, Morales M, Aranda E, Panes O, et al. Template bleeding time and PFA-100 have low sensibility to screen patients with hereditary mucocutaneous hemorrhages: comparative study in 148 patients. J. Thromb Haemost 2004;2:892-8. [ Links ]
21. Reber G, Boehlen F, Fontana P. Study of primary hemostasis in vitro with the platelet function analyser (PFA-100). Rev Med Suisse Romande 2003;123:491-4. [ Links ]
22. Madan M, Berkowitz SD, Christie DJ, Jennings LK, Smit AC, Sigmon KN, et al. Rapid assessment of glycoprotein Iib/IIIa blockade with the platelet function analyzer (PFA-100) during percutaneous coronary intervention. Am Heart J 2001;141:226-33. [ Links ]
23. Lemkin SR, Billesdon JE, Davee JS, Leake DL, Kattlove HE. Aspirin induced oral bleeding: correction with platelet transfusion. Oral Surg 1974;37:498-501. [ Links ]
24. Thomason JM, Seymour RA, Murphy P, Brigham KM, Jones P. Aspirin-induced post-gingivectomy haemorrhage: a timely reminder. J Clin Periodontol 1997;24:136-8. [ Links ]
25. McGaul T. Postoperative bleeding caused by aspirin. J Dent 1978;6:207-9. [ Links ]
26. Foulke CN. Gingival haemorrhage related to aspirin ingestion. J Periodontol 1976;47:355-7. [ Links ]
27. Golanski J, Phita J, Baraniak J, Watala C. Limited usefulness of the PFA-100 for the monitoring of ADP receptor antagonists- in vitro experience. Clin Chem Lab Med 2004;42:25-9. [ Links ]
28. Caiappa R, Nilhite TR, Parvin CA, Luchtman-Jones L. Comparison of PFA-100 and bleeding time testing pediatric patients huir suspected hemorrhagic problems. J Pediatr Hematol Oncol 2003;25:474-9. [ Links ]
29. Alberts MJ, Bergman DL, Molner E, Jovanovic BD, Ushiwata I, Teruya J. Antiplatelet effect of aspirin in patients with cerebrovascular disease. JAMA 2003;289:2947-57. [ Links ]
30. Van der Planken MG, Claeys MJ, Vertessen FJ, Dilling D, Bosmans JM, Berneman ZN et al. Comparison of turbidimetric aggregation and in vitro bleeding time (PFA-100) for monitoring the platelet inhibitory profile of antiplatelets agents in patients undergoing stent implantation. Thromb Res 2003;111:159-64. [ Links ]
![]() Correspondence:
Correspondence:
Dr. Juan José Arrieta Blanco
C/ Clara del Rey 79,3º B
28002-Madrid
E-mail: jjarrieta@fjd.es
Received: 29-07-2005
Accepted: 3-06-2006

