










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 Espanhol (pdf)
Espanhol (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
versão On-line ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.12 no.1 Jan. 2007
Immunohistochemical profile of canalicular adenoma of the upper lip: a case report
Michele Conceição Pereira, Alessandro Antônio Costa Pereira, João Adolfo Costa Hanemann
Department of Pathology and Stomatology, Alfenas Dentistry and Pharmacy School, Alfenas, Minas Gerais, Brazil
ABSTRACT
Canalicular adenoma is an uncommon benign salivary gland neoplasm that has a marked predilection for occurrence in the upper lip. It is composed of columnar cells arranged in branching and interconnecting cords of single or double cell thick rows. This tumor has an excellent prognosis after conservative surgical treatment in all locations. In the present report we describe, using immunohistochemistry, the expression of cytokeratins (CK), S-100 protein and EMA in a canalicular adenoma that arose in the upper lip of a 55-year-old female. Cells of the canalicular adenoma showed an immunohistochemical profile that indicates an excretory duct origin: most of these cells positively expressed AE1/AE3 cytokeratins and S100 protein. A comparison of the immunohistochemical features of canalicular adenoma with other salivary gland neoplasms that share similar histological features is discussed.
Key words: Canalicular adenoma; salivary gland tumours, immunohistochemistry.
Introduction
Salivary gland tumours are relatively uncommon and represent 2-3% of head and neck neoplasms (1-3). Canalicular adenoma (CA) is a benign neoplasm that can manifest from minor salivary gland ductal tissue throughout the oral cavity and infrequently in the parotid gland. A high proportion of canalicular adenomas occur in the upper lip, a predilection not evident in other salivary gland tumours (4). We described the immunohistochemical expression of some antibodies in a case of canalicular adenoma arising from upper lip. The main purpose was to contribute to the literature regarding the origin of oral canalicular adenoma based in its immunohistochemical profile.
Case report
The patient, a 55-year-old female, presented to the Stomatology Clinic with the primary complaint of an enlarging nodule on the upper lip of twelve months duration. The nodule was neither painful nor associated with bleeding. Her medical history was positive for cigarette smoking and hypertension. Intra-oral examination revealed a 1.0X1.0 cm nodule fluctuant to palpation of the left side of upper lip. The overlying mucosa was normal in color and non-ulcerated (Figure 1). Under local anesthesia the patient underwent surgery for excision of the nodule. Three years after surgery the patient is well without evidence of disease.

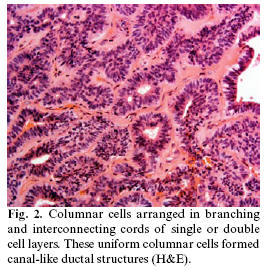
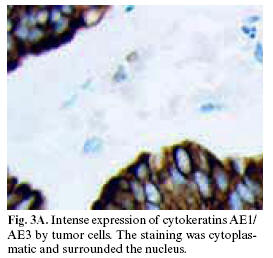
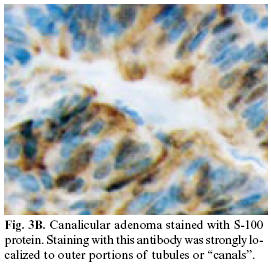
Microscopically, the tumour was composed of columnar cells arranged in branching and interconnecting cords of single or double cell layers. These uniform columnar cells formed canal-like ductal structures (Figure 2). The tumour cells were supported by a loose and highly vascular connective tissue stroma. A thin fibrous capsule surrounded the tumour. Cellular pleomorphism and mitoses were not observed. These microscopic findings were interpreted as a canalicular adenoma. Immunohistochemically, most of the cells were positive for AE1/AE3 cytokeratins (Figure 3A) and S-100 protein (Figure 3B) and very focally for epithelial membrane antigen (EMA). The staining was cytoplasmatic and surrounded the nucleus. No staining was observed with carcinoembryonic antigen (CEA), calponin and p63 antibodies.
Discussion
Salivary gland tumors carry a wide spectrum of histopathological features, which may share a common single-cell origin, from the epithelial progenitor basal duct cells and have a different tendency of malignant progression (2). Based on ultrastructural and histochemical aspects, some authors have suggested that possibly the canalicular adenoma has an excretory duct origin, although an intercalated duct origin has also been indicated (5). Histologically, this lesion can be confused with malignant salivary gland tumours, including adenoid cystic carcinoma, ameloblastoma and adenocarcinoma (6-9). To minimize possible diagnostic errors, studies using immunohistochemistry have led to the development of panels of antibodies that allow distinction between lesions that present common features.
Cells of the canalicular adenoma, in the case reported, showed an immunohistochemical profile that signalized to an excretory duct origin: most of these cells positively expressed AE1/AE3 cytokeratins and S100 protein, thus confirming previous studies (5,10). However, it is now well established that S100 protein is not a specific myoepithelial marker (11).
In 135 normal salivary glands, Prasad et al (11) observed that only the myoepithelial cells surrounding the acini and intercalated ducts reacted to calponin. These aspects were also noted in all 17 canalicular adenomas. This fact confirms that antibody to be highly specific marker of normal and neoplastic myoepithelium.
Our immunohistochemical findings, regarding CEA and EMA, are in agreement with Ferreiro (7) who reported that the canalicular adenomas are CEA negative and only infrequently EMA positive. We were unable to demonstrate any p63 staining in canalicular adenoma. This is in agreement with Edwards et al (12), who showing an absence of myoepithelial differentiation in canalicular adenoma both via immunohistochemical and ultrastructural studies, and is consistent with this tumors putative ductal luminal cell differentiation.
In summary, in the present case, the strong and frequent staining for S100 protein represents the main characteristic of canalicular adenoma. The epithelial nature was determined by the high positivity for related cytokeratins and the absence of any reactivity for calponin rules-out a myoepithelial origin of this lesion.
References
1. Allen CM, Damm D, Neville B, Rodu B, Page D, Weathers DR. Necrosis in benign salivary gland neoplasms. Not necessarily a sign of malignant transformation. Oral Surg Oral Med Oral Pathol 1994;78:455-61. [ Links ]
2. Weber A, Langhanki L, Schutz A, Gerstner A, Bootz F, Wittekind C et al. Expression profiles of p53, p63, and p73 in benign salivary gland tumors. Virchows Arch 2002; 441:428-36. [ Links ]
3. Ledesma-Montes C, Garces-Ortiz M. Salivary gland tumours in a Mexican sample. A retrospective study. Med Oral; 2002;7:324-30. [ Links ]
4. Smullin SE, Fielding AF, Susarla SM, Pringle G, Eichstaedt R. Canalicular adenoma of the palate: case report and literature review. Oral Surg Oral Med Oral Pathol 2004;98:32-6. [ Links ]
5. Machado de Sousa SO, Soares de Araujo N, Correa L, Pires Soubhia AM, Cavalcanti de Araujo V. Immunohistochemical aspects of basal cell adenoma and canalicular adenoma of salivary glands. Oral Oncol 2001;37:365-8. [ Links ]
6. Batsakis JG. Oral monomorphic adenomas. Ann Otolo Rhinol Laryngol 1991;100:348-50. [ Links ]
7. Ferreiro JA. Immunohistochemical analysis of salivary gland canalicular adenoma. Oral Surg Oral Med Oral Pathol 1994;78:761-5. [ Links ]
8. Harmse JL, Saleh HA, Odutoye T, Alsanjari NA, Mountain RE. Recurrent canalicular adenoma of the minor salivary glands in the upper lip. J Laryngol Otol 1997;111:985-7. [ Links ]
9. Furuse C, Tucci R, Sousa SOM, Carvalho YR, Araujo VC. Comparative immunoprofile of polymorphous low grade adenocarcinoma and canalicular adenoma. Ann Diagn Pathol 2003;7:278-80. [ Links ]
10. Zarbo RJ, Prasad AN, Regezi JA, Gown AM, Savera AT. Salivary gland basal and canalicular adenomas- immunohistochemical demonstration of myoepithelial cell participation and morphogenetic considerations. Arch Pathol Lab Med 2000;124:401-5. [ Links ]
11. Prasad AN, Savera AT, Gown AM, Zarbo RJ. The myoepithelial phenotype in 135 benign and malignant salivary gland tumors other than pleomorphic adenoma. Arch Pathol Lab Med 1999;123:801-6. [ Links ]
12. Edwards PC, Bhuiya T, Kelsch RD. Assessment of p63 expression in the salivary gland neoplasms adenoid cystic carcinoma, polymorphous low-grade adenocarcinoma, and basal cell and canalicular adenomas. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;97:613-9. [ Links ]
![]() Correspondence:
Correspondence:
Dr. João Adolfo Costa Hanemann, DDS, PhD
Departamento de Estomatologia.
Escola de Farmácia e Odontologia de Alfenas.
Rua Gabriel Monteiro da Silva, 714.
Alfenas, Minas Gerais, Brasil.
37130-000
E-mail: jachanemann@uol.com.br
Received: 2-07-2005
Accepted: 23-10-2006

