










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
versión On-line ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.12 no.5 sep. 2007
Maxillary lesion presenting as a first sign of multiple myeloma: Case report
Lucielma Salmito Soares Pinto1, Eduardo Bauml Campagnoli1, Jorge Esquiche Leon1, Márcio Ajudarte Lopes2, Jacks Jorge2
(1) PhD Student
(2) Associated Professor, Oral Semiology and Oral Pathology, Department of Oral Diagnosis, Dental School, University of Campinas (UNICAMP), Piracicaba, Sao Paulo, Brazil
ABSTRACT
Plasma cell neoplasia is a lymphoid neoplastic proliferation of B cells. This denomination encloses multiple myeloma (MM), solitary bone plasmacytoma and extramedullary plasmacytoma. MM consists of a clonal proliferation of plasma cells based in the bone marrow, with various degrees of differentiation. Neoplastic cells usually produce great amounts of monoclonal light or heavy chains of immunoglobulin that can be detected in serum or urine. The disease is more frequently in men and the average age at diagnosis is about 60 years. The diagnosis is established by blood and urine exams and medullary biopsy. Patients may present renal failure, bone pain, fatigue, recurrent infections and nervous system dysfunction. Oral manifestations may be the first sign of MM, highlighting the importance of the dentist in the early diagnosis of the disease. Treatment involves mainly irradiation and chemotherapy and the prognosis is generally poor. This paper reports a case of a 65 years old black female who had a complaint of a painful mass in the maxilla that prompted a MM diagnosis.
Key words: Plasmacytoma, multiple myeloma, jaw neoplasms.
Introduction
Plasma cell tumors are lymphoid neoplastic proliferations that have been grouped among B-cell peripheral lymphomas, according to the classification of the European-American International Lymphoma Study Group (1). They can affect a single bone, a condition called solitary plasmacytoma; or may involve only soft tissues, an extramedullary plasmacytoma. However, in approximately 95% of the cases, it involves several bones, when is called multiple myeloma (MM) (2, 3). MM is the most important symptomatic monoclonal gammopathy and represents approximately 1% of all cancers, and 10% of all hematological neoplasms (4, 5). It is characterized by numerous abnormal plasma cells permeating the bone marrow and overproduction of monoclonal light-chain or heavy-chain immunoglobulins that are identifiable in serum or urine (5). The etiology remains unknown, but some occupations, exposure to certain chemicals, overdose irradiation, viruses and genetic factors have been suggested as etiologic factors. The diagnosis of this pathology is established by histologic confirmation of a malignant proliferation of plasma cells, hematologic and biochemical findings, urine analysis and skeletal radiographic survey (3).
It occurs in all races, but rates are higher in African Americans and lower in Asian population. This neoplasia is more common among patients with a mean age of about 60 years, and men are more affected than women (5). Symptoms frequently result from lytic bone disease, anemia, renal failure and immunodeficiency (6). Complaints that are usually present at diagnosis are: bone pain (58%), fatigue (32%) and weight loss (24%) (5). Treatment involves irradiation, chemotherapy and more lately, autologous transplantation for young patients, and in addition, supportive measures may be used. Although the prognosis is generally poor, it may be affected by patients age, tumor site, renal involvement, and histological features (3).
Case report
A 65-year-old black woman was referred because of a painful maxillary mass for approximately 15 days. The patient was edentulous, and episodes of bleeding and pain were impairing the upper denture wearing. Her previous medical history revealed an episode of pneumonia two years earlier and there was no family history of cancer.
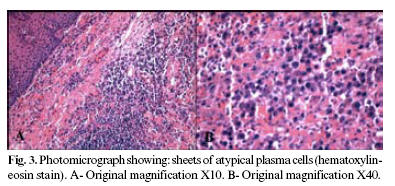
Lymphadenopathy was not observed. Intraoral examination disclosed a bluish-red swelling in the left canine area of the maxilla. It had a smooth surface and measured approximately one cm in its maximum diameter (Figure 1). Orthopantomogram survey was not worthwhile, while periapical radiograph showed a diffuse radiolucency (Figure 2). An incisional biopsy was taken under local anesthesia. The histological features were sheets of atypical plasma cells (Figure 3). The immunohistochemistry results were positive for EMA and negative for L26, AE1/AE3, HMB45 and S100. Monoclonal staining for kappa was positive whereas lambda was negative establishing the diagnosis of a malignant plasma-cell tumor (Figure 4). The patient was then referred for systemic evaluation. The serum electrophoresis revealed an IgG monoclonal gammopathy and bone marrow examination displayed more than 50% plasmocitosis. Other laboratorial findings were high serum level of ß-2 microglobulin, hypocalcemia, anemia and thrombocytopenia. Lactate dehydrogenase and creatinine levels were normal (Table 1).




There was no myeloma protein in the urine. The skeletal radiographic survey showed osteoporotic lesions in skull and punch-out osteolytic lesion in femur (Figure 5). According with these results, the diagnosis was MM stage IIIA (Durie and Salmon staging system). Oral chemotherapy included cyclophosphamide and prednisone. One month of chemotherapy prompted maxillary lesion regression (Figure 6); although the treatment was unsuccessful, and the patient died nine months latter.


Discussion
The first well-documented case of multiple myeloma was reported by Samuel Solley in 1844, and the term "Multiple Myeloma" was introduced by J. von Rustizky in 1873 (5, 7). It is a progressive malignant disease of plasma cells clones in various stages of differentiation. Bone marrow examination shows a high amount of these abnormal plasma cells. In 99% of patients, MM is a secretory condition and overproduction of monoclonal immunoglobulins in serum and/or light chains (Bence Jones proteins) in the urine can be detected (6).
MM is more often in patients between 50 and 80 years of age, with a mean age of 60 years and man are more affected than women (5). Systemic symptoms include bone pain and pathologic fracture, renal failure, hypercalcemia, weight loss, fatigue, weakness, shortening of the spine, fever, thrombocytopenia, neutropenia, diarrhea, orthostatic hypotension and infections (4, 8). Initial findings are bone pain in 68% of patients, anemia in 62%, renal insufficiency in 55%, hypercalcemia in 30%, palpable liver in 21%, and palpable spleen in 5% (9).
The oral manifestations of MM are the first sing of the disease in about 14% of the patients (10). They may include swelling, pain, numbness, bleeding, mobile teeth, xerostomia, amyloid deposits, root resorption and mobility, labial anesthesia and jaw radiolucencies and fractures, and the prevalence varies from 2% to 70% (4, 6, 8, 10, 11, 12). In this case report, a painful swelling was the initial complaint. Although mandibular and posterior lesions are more frequent (8), in this case, there was an anterior maxillary swelling.
Histologically, plasmacytomas exhibit monotonous proliferation of pure plasma cells, in various maturation stages (2). Immunohistochemistry stains must be done to confirm plasmacytoma. Up to 85% of plasma cell neoplasms are positive for EMA, an antibody against epithelial membrane antigen that recognizes the breast epithelial mucin complex. L26 stain, the favored "pan-B" cell antibody, represents CD20, which is expressed normally on mature B-cells and a subset of immature B-cells, follows the expression patterns in normal B-cell development; as a result plasmacytomas are usually negative for this antibody (13). Light chain restriction for Kappa or lambda is usually observed, and nearly 70% of plasma cell neoplasms are Kappa positive (13, 14). AE1/AE3, HMB45 and S100 immunoreactivity in plasmacytomas is generally considered rare and are done to exclude other pathologies. (15). In this case, both histological and immunohistochemistry led to the diagnosis of malignant plasma-cell lesion.
The diagnosis of MM may be established by laboratorial exams, such hematologic, biochemical findings, urine analysis and skeletal radiographic survey (3). The diagnostic criteria for MM include evidence of multiple osteolytic lesions, identification of an atypical plasma cell population on biopsy and abnormalities of immunoglobulin production (Table 2) (16).

Bone osteolytic lesions are frequently seen in 79% of the MM cases, and result from the osteoclastic activation by cytokines, increasing osteoclast numbers in areas invaded by malignant plasma cells and inhibiting bone formation (5). The most often involved sites are the vertebrae, skull, pelvic bones, ribs, humerus, and femur in this order of frequency. Jaws may be involved in 30% (2, 10). The radiographic appearance of the lesions is generally of punched-out osteolytic lesions (60%), although generalized osteoporosis may also be seen (30%) (6). Radiographic examination of the patient revealed osteolytic lesions in femur and skull, in agreement with previous studies.
Laboratorial tests for MM usually reveal anemia (73%), trombocytopenia (5%) and normal creatinine value (52%). High serum levels of ß-2 microglobulin can be seen in 75% of the patients reflecting the tumor mass (5); it is one of the most powerful prognostic factors currently available for MM and can be used alone or in combination with other variables for pretreatment stratification (17). These laboratorial results were also seen in our patients exams. Hypercalcemia is also a regular feature, although in our case it as not detected.
Serum eletrophoresis shows myeloma protein (M-protein) in about 93% of the patients. Approximately 70% of myelomas secrete immunoglobulin G, and in addition, kappa light chains are more common. In our case, serum protein electrophoresis showed an IgG monoclonal spike. Urine eletrophoresis may show M-protein around 60% of the patients, nevertheless no myeloma protein was detected in the urine of our patient (5). In nonsecretory myelomas, immunoglobulins can be detected within the cytoplasm of the malignant plasma cells but not in serum or urine (2).
Bone marrow examination levels of 10% or more of plasmocitosis are observed in 96% of patients. Medullary examination of our patient showed more than 50% plasma cells. The final diagnose was MM, stage IIIA (Durie and Salmon staging system), i.e. an active and symptomatic disease without renal failure. The treatment of MM consists of chemotherapy. Cyclophosphamide, an alkylating agent, associated with prednisone were used in our case (3). The prognosis is generally considered poor, as show by the evolution in our case. The patient died 12 months after the diagnosis, because of the disease. In this case, a maxillary lesion was the first sign of MM, reinforcing the fundamental role of the dentist in the recognition and early diagnosis of systemic conditions.
References
1. Seoane J, Aguirre-Urizar JM, Esparza-Gomez G, Suarez-Cunqueiro M, Campos-Trapero J, Pomareda M. The spectrum of plasma cell neoplasia in oral pathology. Med Oral 2003;8:269-80. [ Links ]
2. Lae ME, Vencio EF, Inwards CY, Unni KK, Nascimento AG. Myeloma of the jaw bones: a clinicopathologic study of 33 cases. Head Neck 2003; 25:373-81. [ Links ]
3. Ozdemir R, Kayiran O, Oruc M, Karaaslan O, Kocer U, Ogun D. Plasmacytoma of the hard palate. J Craniofac Surg 2005;16:164-9. [ Links ]
4. Currie WJ, Hill RR, Keshani DK. An unusual cause of maxillary tuberosity enlargement. Br Dent J 1994;177:60-2. [ Links ]
5. Kyle RA, Gertz MA, Witzig TE, Lust JA, Lacy MQ, Dispenzieri A et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc 2003; 78:21-33. [ Links ]
6. Gray ST, Antunovic DM, White AE. Non secretory multiple myeloma involving the maxilla: report of a case with update of biology and new approaches to management. Oral Oncol 1997; 33:136-40. [ Links ]
7. Kyle RA. Multiple myeloma: an odyssey of discovery. Br J Haematol 2000;111:1035-44. [ Links ]
8. Zachriades N, Papanicolaou S, Papavassiliou D, Vairaktaris E, Triantafyllou D, Mezitis M. Plasma cell myeloma of the jaws. Int J Oral Maxillofac Surg 1987;16:510-5. [ Links ]
9. Kyle RA. Multiple myeloma: review of 869 cases. Mayo Clin Proc 1975;50:29-40. [ Links ]
10. Epstein JB, Voss NJ, Stevenson-Moore P. Maxillofacial manifestations of multiple myeloma. An unusual case and review of the literature. Oral Surg Oral Med Oral Pathol 1984;57:267-71. [ Links ]
11. Mateo Arias J, Molina Martinez M, Borrego A, Mayorga F. Amyloidosis of the submaxillary gland. Med Oral 2003;8:66-70. [ Links ]
12. Reboiras Lopez MD, Garcia Garcia A, Antunez Lopez J, Blanco Carrion A, Gandara Vila P, Gandara Rey JM. Anaesthesia of the right lower hemilip as a first manifestation of multiple myeloma. Presentation of a clinical case. Med Oral 2001;6:168-72. [ Links ]
13. Hsi ED, Yegappan S. Lymphoma Immunophenotyping: A New Era in Paraffin-Section Immunohistochemistry. Advances in Anatomic Pathology 2001;8:218-39. [ Links ]
14. Bayer-Garner IB, Prieto VG, Smoller BR. Detection of clonality with kappa and lambda immunohistochemical analysis in cutaneous plasmacytomas. Arch Pathol Lab Med 2004;128:645-8. [ Links ]
15. Shin JS, Stopyra GA, Warhol MJ, Multhaupt HAB. Plasmacytoma with aberrant expression of myeloid markers, T-cell markers, and cytokeratin. The Journal of Histochemistry & Cytochemistry 2001;49:791–2. [ Links ]
16. Rosai J. Rosai and Ackermans Surgical Pathology. St Louis: Mosby Co.; 2004. p. 2099-105. [ Links ]
17. Durie BGM, Stock-Novack D, Salmon SE, Finley P, Beckord J, Crowley J et al. Prognostic Value of Pretreatment Serum X-2 Microglobulin in Myeloma: A Southwest Oncology Group Study. Blood 1990;75:823-30. [ Links ]
![]() Correspondence:
Correspondence:
Dr. Jacks Jorge
Faculdade de Odontologia de Piracicaba-UNICAMP
Av. Limeira, 901 – Areão - Caixa Postal 52 – CEP: 13414-903 –
Piracicaba/SP – Brazil
E-mail: jjorge@fop.unicamp.br
Received: 2-07-2006
Accepted: 5-11-2006

