










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
versión On-line ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.12 no.6 oct. 2007
Congenital granular cell tumor (congenital epulis): A lesion of multidisciplinary interest
Guilherme Costa Carvalho Silva1, Tainah Couto Vieira2, Janaina Couto Vieira3, Carlos Roberto Martins4, Edgard Carvalho Silva5
(1) DDS, MDS. Fellow, Masters Program in Dentistry, School of Dentistry, Catholic University of Minas Gerais
(2) DDS. Resident, Department of Pediatric Dentistry and Orthodontics, School of Dentistry, Universidade Federal de Minas Gerais
(3) MD. Resident, Otorhinolaryngology Section, Santa Casa Hospital of Belo Horizonte
(4) DDS, PhD. Professor of Oral Pathology, School of Dentistry, Catholic University of Minas Gerais
(5) DDS, PhD. Emeritus Professor and Chairman, Department of Oral Surgery and Pathology, School of Dentistry, Universidade Federal de Minas Gerais, Belo Horizonte, Brasil
ABSTRACT
Congenital granular cell tumor (CGCT), or congenital epulis, is an uncommon benign soft tissue lesion that usually arises from the alveolar mucosa of neonates and may cause respiratory and feeding problems. We report a case of a 3-day-old female newborn, who presented an intraoral tumor mass which was protruding from her mouth, compromising feeding. Under general anesthesia, the lesion was completely removed and the patient had an uneventful postoperative course. Clinical features and treatment approaches are presented and discussed, emphasizing the necessity of a multidisciplinary approach in such cases.
Key words: Congenital epulis, congenital granular cell tumor, Neumanns tumor, gingival tumor.
Introduction
Congenital granular cell tumor (CGCT), first described by Neumann (1) in 1871, is a benign soft tissue lesion of the neonate that almost always arises from the alveolar mucosa. It is also known as congenital epulis or Neumanns tumor. Lesions may be sessile or pedunculated, normally colored or reddish, varying in size from several millimeters to a few centimeters (2), it is typically seen protruding from the neonates mouth. Females are affected from 8 to 10 times more frequently than males (2,3), perhaps indicating a hormonal component in its development. The CGCT occurs more frequently in the maxilla (maxillary/mandibular ratio: 3:1), mainly on its anterior portion (2,3). Usually, it is presented as a single lesion, however multiples cases have been reported (3-6).
Surgical excision is advocated as the treatment of choice for CGCT, preferably immediately after detection, since spontaneous regression is rare and large tumors may cause airway obstruction and feeding difficulties (3-11). There are no reports showing CGCT recurrence or malignant transformation (3).
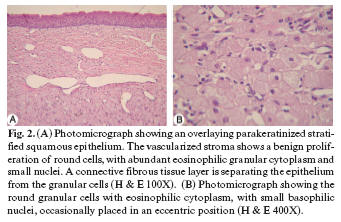
The histological picture shows large, round cells with abundant eosinophilic granular cytoplasm, and round or oval lightly basophilic nuclei (3,4,6-10). The histogenesis of this tumor has been investigated, although it remains controversial and inconclusive (3).
The aim of this paper is to report a case of CGCT in a 3-day-old girl, presenting the clinical and histological characteristics of the lesion and to point out the importance of a multidisciplinary approach to diagnosis and treatment.
Case report
A 3-day-old Caucasian girl, born at 40 weeks gestation weighing 2.95 kg, was brought by her mother for evaluation of a mass protruding from her mouth, which was causing feeding difficulties, but no airway obstruction. The infant was born by normal vaginal delivery, with uneventful prenatal and perinatal course, and was otherwise healthy. According to her mother she had already been examined by a pediatrician and an obstetrician, who were not able to diagnose the alteration.
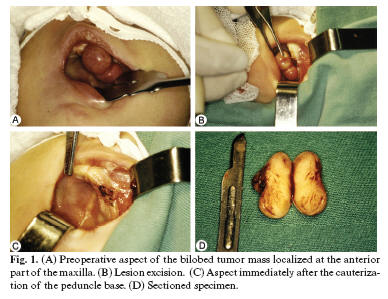
Intraoral examination revealed a bilobed and pedunculated tumoral mass, with color similar to the adjacent mucosa, arising from the alveolar mucosa on the left maxillary canine region. It was approximately 2 cm in diameter, had a smooth and firm surface and was protruding slightly from the mouth (Figure 1A). Based on the clinical features of the lesion, a CGCT diagnosis was considered and complete surgical removal of the lesion was recommended.
Under general anesthesia with nasotracheal intubation, the tumor was completely excised using electrocautery (Figures 1B and 1C). Bleeding was minimal and the infant recovered with no complications. Breast-feeding began three hours after the surgery. The excised material (Figure 1D) was sent for histological examination and the diagnosis was CGCT (Figures 2A and 2B).
Discussion
CGCT is usually referred as congenital epulis in the medical literature. However, epulis is a non-specific term used to designate hyperplastic gingival tissue or gingival tumor masses. Since there are cases which are not exclusively related to the gingiva (3,6), it seems that the term CGCT would be more appropriate.
It presents a wide range of differential diagnoses, such as granular cell tumor, fibroma and melanotic neuroectodermal tumor of infancy, among others. However, the clinical diagnosis is usually simple due to the typical occurrence in the maxillary alveolar mucosa of newborn girls.
Intrauterine images of the tumor may be obtained by ultrasonography (7,8-10) or even by magnetic resonance (10), mainly in the last weeks of pregnancy. Although there are studies that affirm successful prenatal diagnosis of CGCT (9,10), these studies actually obtained images of the tumor mass, suggesting CGCT, but the diagnosis could not be conclusive.
Prenatal imaging is important in the choice of delivery method, since large tumors may compromise a normal vaginal delivery and a cesarean operation may be necessary (9-11). Also, the identification of a tumor on a fetus may help the intervention planning, and allows the family to prepare psychologically for eventual procedures that will take place in the newborn. Unfortunately, prenatal ultrasound images of the patient were not obtained.
The treatment of choice is surgical excision, to be performed as soon as possible (2-11). The use of general anesthesia seems to be the recommended procedure in such cases (3,5,8). There are reports of lesion removal without the use of anesthesia (10), however this kind of procedure is not justified since these surgical interventions are elective. The CGCT removal under local anesthesia is also an alternative (7) when intubation is not possible (4) or in cases of small lesions. There is also the possibility of removal during the delivery, in cases where the lesion was detected during pregnancy (9). This approach may eliminate additional procedures such as anesthesia and intubation, and provides the newborn a free airway and an unobstructed oral cavity immediately after birth.
The CGCT diagnosis and management is of interest for the oral and maxillofacial surgeon, the radiologist, the anesthetist, the otorhinolaryngologist, the pediatrician and the obstetrician-gynecologist. Although several professionals are involved with prenatal and delivery care, sometimes a lesion such as the one reported may cause surprise and concern to the medical team. The interaction between professionals involved with the prenatal care and those involved in the treatment of oral and maxillofacial lesions and syndromes, would certainly optimize the diagnosis and treatment approaches in such cases.
References
1. Neumann E. Elin Fall von Congenitaler Epulis. Arch Heilk. 1871;12:189. [ Links ]
2. Fuhr AH, Krogh PH. Congenital epulis of the newborn: centennial review of the literature and a report of case. J Oral Surg. 1972 Jan;30(1):30-5. [ Links ]
3. Loyola AM, Gatti AF, Pinto DS Jr, Mesquita RA. Alveolar and extra-alveolar granular cell lesions of the newborn: report of case and review of literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997 Dec;84(6):668-71. [ Links ]
4. Parmigiani S, Giordano G, Fellegara G, Brevi B, Magnani C. A rare case of multiple congenital epulis. J Matern Fetal Neonatal Med. 2004 Nov;16 Suppl 2:55-8. [ Links ]
5. Canavan-Holliday KS, Lawson RA. Anaesthetic management of the newborn with multiple congenital epulides. Br J Anaesth. 2004 Nov;93(5):742-4. Epub 2004 Sep 3. [ Links ]
6. Yavuzer R, Ataoglu O, Sari A. Multiple congenital epulis of the alveolar ridge and tongue. Ann Plast Surg. 2001 Aug;47(2):199-202. [ Links ]
7. Song WS, Kim JW, Kim YG, Ryu DM. A case report of congenital epulis in the fetus. J Oral Maxillofac Surg. 2005 Jan;63(1):135-7. [ Links ]
8. Lapid O, Shaco-Levy R, Krieger Y, Kachko L, Sagi A. Congenital epulis. Pediatrics. 2001 Feb;107(2):E22. [ Links ]
9. Kumar P, Kim HH, Zahtz GD, Valderrama E, Steele AM. Obstructive congenital epulis: prenatal diagnosis and perinatal management. Laryngoscope. 2002 Nov;112(11):1935-9. [ Links ]
10. Nakata M, Anno K, Matsumori LT, Sumie M, Sase M, Nakano T, et al. Prenatal diagnosis of congenital epulis: a case report. Ultrasound Obstet Gynecol. 2002 Dec;20(6):627-9. [ Links ]
11. Roy S, Sinsky A, Williams B, Desilets V, Patenaude YG. Congenital epulis: prenatal imaging with MRI and ultrasound. Pediatr Radiol. 2003 Nov;33(11):800-3. Epub 2003 Sep 5. [ Links ]
![]() Correspondence:
Correspondence:
Dr. Guilherme Costa Carvalho Silva
Av Afonso Pena 4334
Belo Horizonte, MG, 30130-009, Brasil
E-mail: guilhermeccs@ufmg.br
Received: 16-08-2006
Accepted: 12-07-2007

