










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
versión On-line ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.12 no.8 dic. 2007
Program for coordinated dental care under general anaesthesia for children with special needs
M. Joaquín de Nova García1, M. Rosa Mourelle Martínez2, Carmen Martín Sanjuán3, Nuria E. Gallardo López2, Esther Carracedo Cabaleiro4, Yolanda Alonso García5
(1) Prof. Titular de Odontopediatría. Departamento de Estomatología IV (Facultad de Odontología Universidad Complutense de Madrid). Director de Título Propio de la UCM: Especialista en atención odontológica integral en el niño con necesidades especiales
(2) Profª. Asociada Departamento de Estomatología IV (UCM). Profesora del TP de la UCM: Especialista en atención odontológica integral en el niño con necesidades especiales
(3) Médico-odontopediatra de la Unidad de Salud Bucodental para Niños Discapacitados del SERMAS
(4) Enfermera de la Unidad de Salud Bucodental para Niños Discapacitados del SERMAS
(5) Ayudante del Departamento de Estomatología IV (UCM). Profesora del TP de la UCM: Especialista en atención odontológica integral en el niño con necesidades especiales
ABSTRACT
Aim: To draw up a program for coordination of dental care for children with special needs between the Course at the Universidad Complutense de Madrid (UCMC) (Specialisation in holistic dental care for children with special needs), and the Disabled Childrens Oral Health Unit (DCOHU) within the Madrid Health Service (SERMAS).
Material and methods: UCMC Protocol for children with special needs. Design of a clinical pathway based on consensus amongst the professionals involved.
Results: Algorithm for dental care for children with special needs. Matrix covering all activities and timing for full dental diagnosis in such patients (general health, oral health and behaviour) to facilitate proper referral of patients requiring general anaesthesia. Inclusion in the matrix of those responsible for each activity.
Conclusions: Improved team work (University – primary health care) in patient evaluation, in provision of information to parents and guardians and in health care quality. From the teaching point of view, students learn to adopt a systematic approach in the decision-making process.
Key words: Dental care pathway, dentistry in children with special needs, holistic dentistry, dentistry under general anaesthesia.
Introduction
Clinical practice has been seen to vary greatly with regard to the use of health care resources and the results obtained, partly because different centres and institutions provide different services, but mostly because services are not always provided to patients correctly (1).
It therefore became necessary to create tools to reduce the variability in health care, to use resources properly and to increase the quality of patient care. As a result, in the 1980s, protocols and guides for clinical practice started to be drawn up, providing clinicians and health care authorities with a tool for providing more efficient, consistent care. Such recommendations were based on consensus and extensive scientific evidence. They assisted professionals in decision-making and helped to improve health care quality, reducing variability (2). In fields such as hospital care where coordination amongst the different professionals is necessary to guarantee systematic, multidisciplinary care, clinical pathways started to be adopted as a means of adapting clinical practice guides to actual practice in order to improve care (3,4).
Dentistry, which previously had followed a purely mechanical approach, now includes thorough analysis of the information available in the development of its own guides and protocols, backed by maximum scientific evidence, while recognising its limitations, most of which are related to random biological factors (5). The practice of dentistry tends to be very individualistic and mostly takes place in dental clinics so there has been little experience in activities to provide coordinated care. In our opinion, however, some areas of dental care could be optimised by the introduction of the type of coordination methods already in use in other areas of health care.
For children with special needs (disabled and/or with a medical condition), additional resources are often needed in dental care. General anaesthesia has to be used in children who do not collaborate and who need extensive treatment (6, 7). In Spain, it is now becoming increasingly common for such care to be provided through the regional health care systems. This is beneficial for patients but is complex because of the coordination needed amongst all the professionals involved (8).
In order to coordinate dental health care for children with special needs, we drew up Clinical Pathways (CP). These were conceived for common medical procedures with a high risk or high cost or requiring cooperation amongst many professionals. Since our aim was to facilitate coordination amongst the different departments providing dental services to children with special needs, we selected from a number of synonymous terms including all-inclusive care, multidisciplinary care, etc. that of coordinated health care.
This was based on Clinical Pathways, which are plans drawn up for clinical processes with foreseeable results, aiming to facilitate systematic, multidisciplinary care for patients (9-10). They define the sequence, duration and responsibilities involved in the process and are based on scientific evidence and consensus amongst all the professionals involved. They help systematise the process and the evaluation of results by means of periodic analysis of indicators and comparison with benchmarks (9-11). A detailed description of all activities from patient admission to discharge makes it possible to coordinate the care provided by the different professionals, ensures standardisation of information and may reduce the cost of prolonged hospital stays (4, 12, 13). Clinical pathways help to achieve on-going improvement by establishing regular evaluation of certain key indicators in the process, thus identifying areas and opportunities for improvement (3, 12). They were appropriate in our study because they are based on the idea that any health problem that is likely to change should follow a protocol.
Our objectives were:
- To coordinate the health care activities carried out by different professionals, defining tasks and responsibilities;
- To offer evidence-based patient care;
- To inform the patient and family members of the health care process;
- To set up a powerful educational tool, in our case for students on the UCM course, by providing an overview of the care plan and of the decision-making process on the basis of the information available;
- To simplify and systematise the recording of information in clinical pathway documents that form part of the patients clinical history;
- To provide a common framework for examining the effectiveness of measures to unify conditions in which care is provided;
- To reduce the frequency of the adverse effects of hospitalisation and instrumentation and, in our case, of inappropriate referrals;
- To reduce costs, as outlined above.
The benefits expected were (14):
- Reduced variability in patient care with statements on what is to be done, avoiding inefficiency, redundant information and delayed or premature decisions.
- Inclusion of the documents in the patients clinical history to provide a source of information for check-ups, for evaluating the care provided, for promoting on-going evaluation;
- Clear definition of the roles and responsibilities of all the professionals involved, thus improving teamwork;
- Promotion of interdisciplinary work;
- A reliable forecast of each clinical process.
Only those disadvantages affecting our situation were considered,namely, lack of a culture of teamwork – in our case between the University and the Primary Health Care Services - and the difficulties arising from lack of experience and of publications on clinical pathways in dentistry (although we are aware that such a clinical pathway is being drawn up by the DCOHU).
After initial adoption or a pilot test, it is important to review applicability, find areas for improvement and correct any problems (2).
The aim of such a systematic approach is to help make the process a dynamic one, with proper adaptation and feedback on any problems arising so that corrections can be made.
Stages (15):
1. Identification of the process.
2. Creating the team of persons involved in the process.
3. Design of the clinical pathway.
4. Pilot test and preliminary analysis of results.
5. Review and adjustment.
6. Definitive implementation.
The starting point was the Course at the Universidad Complutense de Madrid (Specialisation in holistic dental care for children with special needs) and our links with the Disabled Childrens Oral Health Unit (DCOHU) for children aged 6-18, which forms part of Primary Health Care Area 2 in the Madrid Health Care Service. We established two main objectives:
- To evaluate certain criteria which would help in decisions on referring patients for treatment under general anaesthesia. Such referral criteria can serve as guidelines for the different professionals involved while helping to ensure proper referral.
- To establish, together with the DCOHU, a tool to improve care quality (better diagnosis, fewer delays in treatment under anaesthesia, lower costs, pre-operation study of patients in their own environments, etc.). (As many as 59% of patients treated by the DCOHU do not need treatment with general anaesthesia, in which cases referrals would be incorrect).
The latter objective is the subject of this publication.
Materials and methods
On the basis of our protocol for dental care for children with special needs (Table 1), the global process can be divided into three stages:
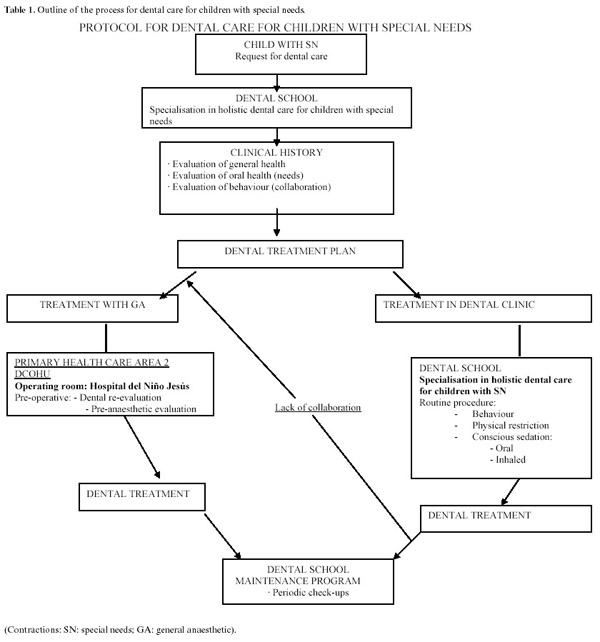
1) Diagnosis. Carried out in the UCM Dental School, starting with admission of the patient by the Reception Department and ending with the dental treatment, stating where treatment is to be given.
2) Treatment, either as out-patients (in the Dental School clinics) or as in-patients (with general anaesthesia in the DCOHU).
3) Check-up. After treatment (as an out-patient or with general anaesthesia), the child receives a personalised oral health maintenance plan from the Dental School or the DCOHU.
If these stages for clinical pathways are adapted to the protocol for patients referred to the DCOHU, they stand as follows:
1) The process to be coordinated under this protocol is dental care under general anaesthesia for children with different special needs.
2) The people involved as the members of the two institutions in which care is provided are:
Dental School:
- Reception Department.
- Radiodiagnosis Department.
- Course on specialisation in holistic dental care for children with special needs.
Primary health care area 2:
- Disabled Children Childrens Oral Health Unit (DCOHU)
3) We draw up the coordinated program, with a classic matrix covering activities / timing. The X axis is for time in columns per day (not necessary consecutive days), and patient location. The Y axis is for actions, activities and information, as required.
4) The program was applied from early 2005, and the results presented cover the first six months.
Based on a consensus reached amongst the professionals involved, we drew up a clinical pathway matrix (Table 2), divided into days for the overall dental diagnosis, with all the activities carried out on patients from admission to the Dental School to referral to the DCOHU for treatment with general anaesthesia.
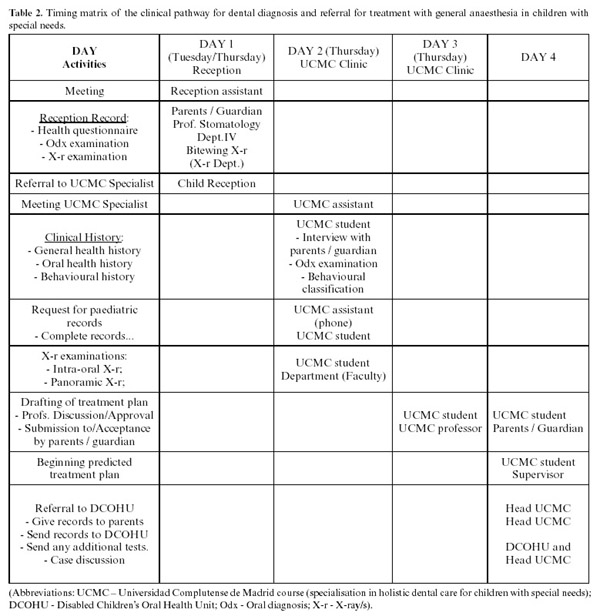
Dental care for our children with special needs is based on the three pillars of a clinical history – general health, oral health and behaviour. We then draw up the personalised dental treatment plan for the patient, determining how and where treatment is to be given. This approach is useful both for patients to be treated in the dental clinic (in the UCM Dental School) and for those to be referred for treatment under general anaesthesia.
As a result, in a short period of just 3 days (counting only those on which the child attends the Dental School), we are able to obtain detailed information leading to more precise selection of children needing general anaesthesia. This is then sent on to the Unit which is to provide the treatment.
The following gives greater detail on the activities to be carried out and the person responsible for them:
Day 1: Admission to the Dental School
Activities:
- Meet the patient as planned; Assistant, Reception Department
- Fill in a health questionnaire; Parents / Guardian
- Complete childs reception documents; Professional, Reception Department
- Refer the patient to the Specialist Course; Professional, Reception Department
Day 2: Admission to the Specialist Course
Activities:
- Meet the patient and parents / guardian; Assistant, Specialist Course
- Request paediatric/medical records; Assistant, Specialist Course
- Allocate to a Specialist Course student; Professional, Specialist Course
- Draw up the clinical history: allocated Specialist Course student
- General health history: Parents: - Interview the parents
- Family background
- Personal background
- Current History. Medication.
- Photocopy of medical records.
- Oral health history: Parents:- Background
- Reason for consultation
Patient:
- Clinical examination
- Complete dental chart
- Complete WHO form X-ray examination
- Bitewing / periapical X-ray
- Panoramic X-ray (if possible)
- Behavioural history:
Parents: -Questionnaire/prediction
Patient: - Evaluation of disability, waiting room
- Cooperation during examination
Day 3: Drafting of the treatment plan
Neither the patient nor the parents / guardian are required to be present.
Activities:
Specialist Course student
- Complete the clinical history:
- General health history: + medical reports;
- Oral health history: + X-ray (Bitewing/periapical/panoramic);
- Behavioural history.
- Draw up the optimum treatment plan for the patient;
- Determine how and where treatment is to be provided;
- Submission/discussion and authorisation; Professional,
Specialist Course
- Determine where treatment is to be provided.
- Complete the report for referral to the DCOHU, if necessary
Day 4: Submission and approval of the treatment plan
Activities: If treatment is to be given in a dental clinic
- Submission and approval of the plan by parents / guardian
- Begin the treatment.
Draw up the report for referral to the DCOHU and submit to parents
Activities: If treatment is to be given under general anaesthesia
- Complete a referral report, with data on:
- Affiliation
- General health history: summary of diagnosis / current medication
- Oral health history: photocopy of dental chart / WHO form + X-ray records
- Behavioural history
State the reasons for referral and explain the reason for any missing documents.
- Hand the report to the parents and inform them how to contact the DCOHU;
- Send the report to the DCOHU (by fax, or e-mail)
- Discuss the clinical case with the head of the DCOHU
Results
The program was adopted in early 2005. During the first six months 27 patients followed the protocol out of 31 called in initially and referred to the Specialisation Course. Of them, 9 (6 boys and 3 girls) were referred to the DCOHU for their dental treatment (Table 3).

In 2 patients (numbers 1 and 5), it was not possible to complete the dental diagnosis because of very negative behaviour and violent movements preventing reliable examination for the purpose of establishing a treatment plan prior to general anaesthesia. In another 2 patients (numbers 2 and 6), in whom it was only possible to complete a clinical diagnosis, treatment was begun in the dental clinic but they were then referred for completion of the treatment under general anaesthesia.
In the remaining 5 patients, clinical diagnosis was carried out and, in patients 4 and 7, this was completed with panoramic X-rays and in patients 3 and 9 with some periapical X-rays.
With regard to the number of days required for the diagnosis stage, the children were required to be present for a minimum of 2 days (days 1 and 2) although for most 3 days were needed (day 3). Although in principle the third day was for drawing up and discussing the treatment plan with the teachers, in practice it turned out to be advisable to complete the examination and carry out the panoramic X-ray where possible. Day 1 can be omitted if the patient is seen directly on the Specialist Course, avoiding any bureaucratic and/or teaching complications, and on Day 4 – except for children who we consider can receive treatment in the dental clinic - only the parents are required to attend to receive information and the referral report.
The main reasons for referral were behaviour and extensive, complex treatment needs. In view of the small number of patients, it was not possible to associate reasons for referral with the medical diagnoses.
After application of the protocol during the 2005/06 academic year, we are currently evaluating the results with a view to final adoption. The professionals involved consider that the experience has led to improvements in various areas. Our dealings with families have been more open and direct and, although this cannot be measured, we note that theyare pleased to be granted access to this Department. The parents satisfaction survey is applied by the DCOHU in all patients referred to it at the end of treatment, but only covers the care received in the Unit.
In addition, we have improved follow-up of patients, which we hope will result in fewer recall visits.
There have also been improvements in the training process for students who endeavour to collect the information on patients to be referred in a more systematic, thorough way. The fact that the need for general anaesthesia in dental treatments has to be explained and justified helps motivate students.
We provide the DCOHU with information on the dental treatment to be given under general anaesthesia and we select the patients, thus avoiding routine, indiscriminate and even unnecessary use of anaesthesia.
Conclusions
We drew up and implemented (as a pilot study) in our Dental School a working philosophy based on a clinical pathway in order to coordinate care for children needing general anaesthesia in a Primary Health Care Unit. We established all the perioperative actions, based on an algorithm for dental care in children with special needs.
References
1. Delgado R. La variabilidad de la práctica clínica. Revista de Calidad Asistencial 1996;11:177-86. [ Links ]
2. Bonafont X, Casasín T. Protocolos terapéuticos y vías clínicas. En: Bonal J, Domínguez-Gil A, Gamundi MC, Napal V, Valverde E, eds. Farmacia Hospitalaria: Planificación y organización. Sociedad Española de Farmacia Hospitalaria. 3ª Ed.2002.p.81-100. Disponible en Internet:http://www.medicinainformacion.com/farmaciahospital_libros.htm [ Links ]
3. García J, Díez J, Chamorro L, Navas A, Franco A, Arribas JL. Vías clínicas. Med Prev 1999;5:28-39. [ Links ]
4. De Dios del Valle R, Franco Vidal A, Chamorro Ramos L, Navas Acien A, Garcia Caballero J. Clinical pathways in primary care. Aten Primaria. 2001 Jun 15;28(1):69-73. [ Links ]
5. Posibilidades de predicción de resultados en odontología, basadas en la evidencia científica. Consejo General de Colegios de Odontólogos y Estomatólogos de España. Fundación Dental Española 2004. Madrid. [ Links ]
6. Vargas-Roman Mdel P, Rodriguez-Bermudo S, Machuca-Portillo G. Dental treatment under general anesthesia: A useful procedure in the third millennium (II). Med Oral. 2003 Aug-Oct;8(4):281-7. [ Links ]
7. Vargas Roman Mdel P, Rodriguez Bermudo S, Machuca Portillo G. Dental treatment under general anesthesia: a useful procedure in the third millennium? (l). Med Oral. 2003 Mar-Apr;8(2):129-35. [ Links ]
8. Limeres Posse J, Vazquez Garcia E, Medina Henriquez J, Tomas Carmona I, Fernandez Feijoo J, Diz Dios P. Pre-assessment of severely handicapped patients suitable of dental treatment under general anesthesia. Med Oral. 2003 Nov-Dec;8(5):353-60. [ Links ]
9. Valiño C, Serrano A, Alcalde J, Abael A, Morales C, Ibarra A y cols. Diseño de una vía clínica para el tratamiento quirúrgico del carcinoma gástrico a partir del análisis del proceso. Rev Calidad Asistencial 2005; 20:256-70. [ Links ]
10. Gutiérrez Dueñas JM, Lozano FJ, Díez Pascual R, Ardela Díaz E, García Arcal D, Domínguez Vallejo FJ. Acute appendicitis. Usefulness of a evidence-based critical pathway. Cir Pediatr. 2002 Oct;15(4):156-61. [ Links ]
11. Jovell AJ, Navarro-Rubio MD. Evaluation of scientific evidence. Med Clin (Barc). 1995 Dec ;105(19):740-3. [ Links ]
12. Pérez-Blanco V, Morant C, García-Caballero J, Vesperinas G, Cos-Blanco AI, Royo C y cols. Desarrollo e implantación de una vía clínica para la cirugía bariátrica. Rev Calidad Asistencial 2004; 19:250-60. [ Links ]
13. Lau C, Cartmill T, Leveaux V. Managing and understanding variances in clinical path methodology: a case study. J Qual Clin Pract. 1996 Jun;16(2):109-17. [ Links ]
14. Walker K. Pathways in paediatrics. En: Pathways of care. Ed Johnson Sue. Blackwell Oxford; 1997. p. 91-119. [ Links ]
15. Plsek PE. Tutorial: quality improvement project models. Qual Manag Health Care. 1993 Winter;1(2):69-81. [ Links ]
![]() Correspondence:
Correspondence:
Dr. M. Joaquín de Nova García,
Departamento de Estomatología IV.
Facultad de Odontología Universidad Complutense de Madrid
Plaza de Ramón y Cajal s/n
Ciudad Universitaria
28040-Madrid. Spain
E-mail: denova@odon.ucm.es
Received: 4-1-2007
Accepted: 23-10-2007

