










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkPharmacy Practice (Granada)
versión On-line ISSN 1886-3655versión impresa ISSN 1885-642X
Pharmacy Pract (Granada) vol.4 no.4 Redondela oct./dic. 2006
| Original Research |
Opinions of West Texas pharmacists about emergency contraception
Gary SUTKIN, Brenda GRANT, Brian K. IRONS, Tyrone F. BORDERS.
| ABSTRACT Background: The pharmacists role in dispensing emergency contraception (EC) has become controversial due to the intersection of personal and professional ethics. Therefore, to examine the issue of EC availability, we surveyed a sample of West Texas pharmacists. West Texas is a religiously and politically conservative region where no methods of EC have been made available. Key words: Contraception, Postcoital. Pharmacists. Ethics, Pharmacy. United States. | RESUMEN Antecedentes: El papel del farmacéutico dispensando contraceptivos de emergencias (CE) es controvertido debido a la intersección de la ética personal y profesional. Así que para examinar el problema de la disponibilidad de CE investigamos una muestra de farmacéuticos de West Texas. West Texas es una región religiosa y políticamente conservadora donde no están disponibles métodos de CE. Palabras clave: Contracepción postcoital. Farmacéuticos. Ética, farmacia. Estados Unidos. |
Gary SUTKIN. MD, MBA Assistant Professor, Departments of Obstetrics and Gynecology. University of Pittsburgh, Magee-Womens Hospital, Pennsylvania (USA).
Brenda GRANT. Resident, Department of Family Medicine, University of Iowa at Cedar Rapids. Iowa (USA).
Brian K. IRONS. Associate Professor, Pharmacy Practice at the Texas Tech University Health Sciences Center. Texas (USA).
Tyrone F. BORDERS. Associate Professor, Department of Health Policy and Management, Fay W. Boozman College of Public Health, University of Arkansas for Medical Sciences. Arkansas (USA).
INTRODUCTION
Hormonal emergency contraception (EC), also called post-coital contraception, is used after unprotected intercourse to prevent pregnancy. Recent controversy has stemmed from news reports of pharmacists refusing to dispense EC due to their right to exercise their conscience to refuse to dispense a prescription in morally objectionable situations.1-3 Some of the controversy may be a result of that fact that the mechanism of action of EC is not precisely known.4 While the prevailing evidence suggests that it prevents conception by preventing or delaying ovulation5-7 there is some evidence to support that it may also work to prevent implantation.8,9
This controversy has caught the attention of professional organizations,10 pharmacists,11 ethicists2, and legislators.12 Physicians,13 midwives,14 and patients15,16 have been surveyed regarding their beliefs, and reports have been generated about pharmacist participation in statewide collaborative drug therapy agreements in Washington and Minnesota.17,18 Yet we are aware of only one survey of the knowledge and beliefs of American retail pharmacists. The survey was from New Mexico, and EC was already widely available at the time it was conducted.19
We undertook our survey in order to ascertain EC beliefs and knowledge from a group of pharmacists in West Texas, which is a religiously and politically conservative region where EC is not available. Lubbock county has approximately 207,000 residents. 27% are Hispanic or Latino, and 9% are black. Another 600,000 West Texas residents live in the surrounding counties.20 We are not aware of any pharmacies in Lubbock county or in the surrounding West Texas counties that carry Preven or Plan B (proprietary forms of EC).
Our objective was to survey a sample of pharmacists in West Texas about their experience, beliefs, and knowledge of EC both before and after a presentation of the current literature about EC.
METHODS
This study was approved by both the West Texas Pharmacists Association (WTPA) and the Texas Tech University Health Sciences Center Institutional Review Board. The WTPA is a professional organization with 400 to 500 members. Its membership includes approximately 20% of the pharmacists practicing in West Texas. The average age of its members is approximately 50 years old, and 85-90% of members are male. The majority of members practice in independent retail pharmacies.
One of the authors (GS) was invited to give a presentation on EC, the biologic studies examining its mechanism of action, and the clinical studies examining its efficacy and safety at the WTPA meeting on September 22, 2003. Prior to and after listening to a 40 minute presentation of the current literature on EC and with informed consent, all 75 attendees of the presentation were given a written survey assessing demographic variables and their experience with, knowledge of, and beliefs about EC. The survey was created by the authors. Participation in the survey was anonymous and voluntary. Demographic variables and answers to the survey questions were calculated using simple frequencies. We tested for differences in the proportions of respondents answers before and after the talk by conducting chi-square analyses. Because the surveys were completed anonymously, we did not have the ability to match pre- and post-answers.
RESULTS
Sixty-four (85%) of the 75 pharmacists who attended the WTPA meeting completed the questionnaire. Table 1 lists characteristics of the 64 respondents, who had a mean age of 60 (range 36-86; mean age of male respondents was 64; mean age of female respondents was 47). 77% of our respondents were from Lubbocks surrounding counties, i.e.: primarily rural areas of West Texas. Of the 11 respondents who stated their practice is ten or more miles from the next pharmacist, 10 (91%) work in independent retail pharmacies and 1 (9%) gave no response. Of the 52 who stated their practice is less than ten miles from the next pharmacist, 21 (40%) work in independent retail pharmacies, 15 (29%) work in chain retail pharmacies, and 16 (31%) work in hospitals or other institutions. One gave no response.
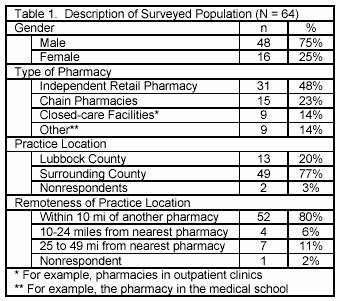
None of the 64 respondents carries any form of proprietary EC (in the form of Preven and Plan B) in his or her pharmacy, has been asked by either a patient or a physician about EC in the previous 12 months, nor have they ever filled a prescription for EC. Yet when asked about their exposure to potential candidates for EC, 8 (13%) had seen a woman reporting a recent rape, 15 (23%) had seen a woman reporting a broken condom, and 60 (94%) had seen a woman report missing some oral contraceptive pills. Five respondents (8%) worked for a pharmacy with a policy on the provision of post-coital contraception with a prescription, even though EC was not carried.
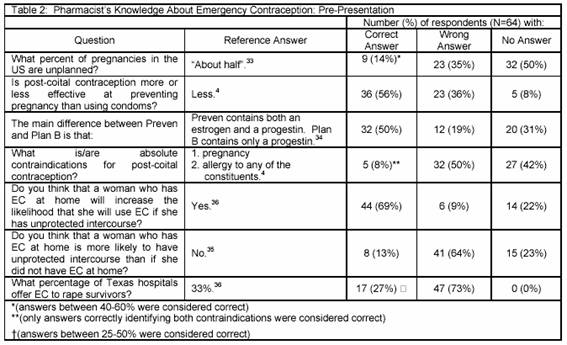
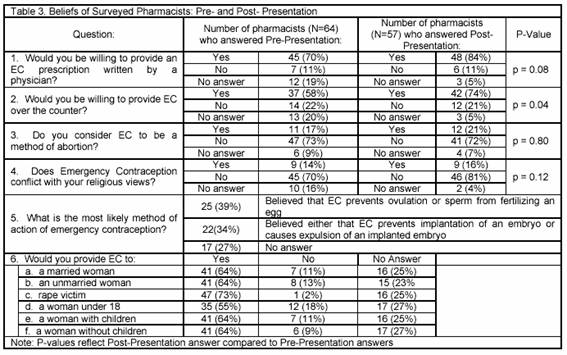
Table 2 summarizes the knowledge of our surveyed pharmacists before the talk. Table 3 summarizes the beliefs of our surveyed pharmacists before and after the talk. Before the presentation, seven of the 45 that would fill a prescription written by a physician would not give it OTC. Seven out of the 14 not willing to provide EC over the counter (OTC) indicated a religious objection. The other 7 had no religious objection to EC. All of the 45 who did not object to EC on religious grounds were willing to fill EC prescriptions written by a physician. 39 of these 45 would also give EC OTC. Only 73% of respondents indicated they would give EC to a rape victim. The presentation did not significantly change their beliefs with exception of an increased willingness to provide EC OTC (p=0.04).
DISCUSSION
This is the first survey that we are aware of that has asked pharmacists in a region where EC is not widely available about their experience with, knowledge of, and beliefs about EC. These pharmacists were generally uninformed about EC and did not carry EC. Many women they saw were candidates for EC but never asked the pharmacist about it. Despite West Texas lack of EC availability, it is not unreasonable to assume that these pharmacists have been exposed to these controversies in the local media. It is interesting that five respondents (8%) worked for pharmacies with a policy on the provision of post-coital contraception but did not actually carry EC. It would have been interesting to hear specific information about those policies, as this dichotomy by itself is an indication of conflicting values.
A survey of pharmacists in New Mexico, where EC is more widely available, generally showed positive attitudes and beliefs about EC.19 Those that participated in a state-approved EC prescribing training program had higher knowledge scores about EC. A survey of Thai pharmacists also showed generally poor knowledge of EC.21 A survey of United Kingdom pharmacists revealed that despite its a wide availability, only 44% had received training in EC.22
Fourteen percent of our pharmacists said that EC conflicts with their religious views, and we were not surprised that our presentation did not significantly alter their beliefs. Pharmacists who object to dispensing an EC prescription believe they have the right not to fill prescriptions that violate their beliefs.1 Yet others feel this type of conscientious objection to fill a valid prescription is not in a patients best interest or safety.23 In Washington State, where pharmacists are allowed to enter into collaborative prescribing agreements with physicians, the majority of surveyed pharmacists indicated that they derive a high satisfaction from providing EC.17 The most common reason given was meeting patients needs. Six states currently protect a patients right to receive EC from a pharmacist, and four states currently allow a pharmacist to refuse to fill an EC prescription.24 In 2005, sixteen states introduced some type of legislation to permit either pharmacists or pharmacies to refuse to fill a valid prescription based on personal beliefs.2,25 Both the American Society of Health System Pharmacists and the American Pharmacists Association endorse referring patients to other pharmacists or pharmacies in cases where filling the prescription conflicts with a pharmacists religious or moral values.1,26
We were surprised that the presentation significantly increased the percentage of pharmacists who would provide EC over the counter. Minnesota also has a collaborative prescribing agreement, but about half of the surveyed pharmacists had reservations about dispensing EC over the counter. Cited reasons included discouraging regular contraceptive use, personal or moral objections to EC, patient safety, lack of knowledge about EC, and liability concerns.18
EC is available OTC in India, Norway, and Sweden.
Because EC is more effective the sooner it is used27 and because privacy issues discourage some women from visiting a physician,28 some have theorized that OTC access to EC would prevent more unwanted pregnancies than if it was only available by prescription.29 One randomized trial demonstrated that pharmacy access (specifically, the ability to obtain EC from a pharmacy without prescription) did not decrease the pregnancy rate, nor did it increase sexual activity.30 This contradicts those who have suggested that wider availability of EC will encourage adolescents to practice risky sexual behavior31 or discourage physicians from screening for sexually transmitted diseases.32 The FDA has approved EC for behind-the-counter distribution to women 18 or older.
Our study is limited by the fact that we surveyed a convenience sample of pharmacists who may have been influenced by a recall bias regarding patient encounters. Furthermore, our survey sample may not be representative of the entire population of West Texas pharmacists. Our survey was not tested for validity or test-retest reliability. Many of our calculations did not reach statistical significance. A larger survey group might give more power to our study.
Our survey also had many non-answers to several questions. Did the pharmacists who did not answer the knowledge questions (i.e.: the 31% who did not know the difference between Preven and Plan B) prefer not to answer, or was that an indication that they did not know the correct answer? We also had many non-answers to the more sensitive questions regarding beliefs. For example, when asked if they would be willing to provide OTC EC, 20% did not answer. Did these 13 object to the question? Did they not understand the question or believe the issue to be more complex than stated? Were they just unsure about the implications of selling EC over the counter? We only gave them yes or no choices and will never know.
CONCLUSION
We surveyed a sample of pharmacists from West Texas about EC. We found a general lack of knowledge about the biology, safety, and efficacy of EC. Fourteen to seventeen percent of our respondents were opposed to EC in general. Although a presentation did increase the percentage that would be willing to provide EC over the counter, it did not significantly change their beliefs.
| References |
1. Cantor J, Baum K. The limits of conscientious objection – may pharmacists refuse to fill prescriptions for emergency contraception? N Engl J Med 2004;351:2008-12. [ Links ]
2. Charo, RA. The celestial fire of conscience – refusing to delivery medical care. N Engl J Med 2005;352:2471-3. [ Links ]
3. Knecht L, Myrick M. Protesters fight pharmacy. Available at: http://www.ntdaily.com/vnews/display.v/ART/2004/02/03/40/401f3ebb7558e. Accessed February 5, 2004. [ Links ]
4. Glasier A. Emergency postcoital contraception. N Engl J Med 1997;337:1058-64. [ Links ]
5. Swahn ML, Westlund P, Johannisson E, Bygdeman, M. Effect of postcoital contraceptive methods on the endometrium and the menstrual cycle. Acta Obstet Gynecol Scand 1996;75:738-44. [ Links ]
6. Marions L, Cekan SZ, Bydgeman M, Gemzell-Danielsson K. Effect of emergency contraception with levonorgestrel or mifepristone on ovarian function. Contraception 2004;69:373-7. [ Links ]
7. Gemzell-Danielsson K, Marions L. Mechanisms of action of mifepristone and levonorgestrel when used for emergency contraception. Hum Reprod Update 2004;10:341-8. [ Links ]
8. Kahlenborn C, Stanford JB, Larimore WL. Postfertilization effect of hormonal emergency contraception. Ann Pharmacother 2002;36:465-70. [ Links ]
9. Trussell J, Ellertson C, Dorflinger L. Effectiveness of the Yuzpe regimen of emergency contraception by cycle day of intercourse: implications for mechanism of action. Contraception 2003;67:167-71. [ Links ]
10. Emergency Oral Contraception. ACOG Practice Bulletin 2001; No 25. In: 2001 Compendium of Selected Publications. The American College of Obstetricians and Gynecologists 2001; pp 462-33. [ Links ]
11. Calis KA. Pharmacists and emergency contraception. N Engl J Med 2005;352:942-3. [ Links ]
12. Davey M, Belluck P, Hart A, et al. Pharmacies balk on after-sex pill and widen fight. The New York Times. 2005 Apr 19;Sect A:1 (col. 1). [ Links ]
13. Harrison T. Availability of emergency contraception: a survey of hospital emergency department staff. Ann Emerg Med 2005;46:105-10. [ Links ]
14. Beckman, LJ, Harvey M., Sherman CA, Petitti DB. Changes in providers views and practices about emergency contraception with education. Obstet Gynecol 2001;97:942-6. [ Links ]
15. Foster DG, Landau SC, Monastersky N, Chung F, et al. Pharmacy access to emergency contraception in California. Perspectives on Sexual and Reproductive Health 2006;38:46-52. [ Links ]
16. Aiken AM, Gold MA, Parker AM. Changes in young womens awareness, attitudes, and perceived barriers to using emergency contraception. J Pediatr Adolesc Gynecol 2005;18:25-32. [ Links ]
17. Sommers SD, Chaiyakunapruk N, Gardner JS, Winkler J. The emergency contraception collaborative prescribing experience in Washington State. J Am Pharm Assoc 2001;41:60-6. [ Links ]
18. Kumar AS, Hall LC, LePage A, Lim, PC. Providing emergency contraceptive pills behind-the-counter: opinions among Minnesota healthcare providers. Contraception 2003;68:253-9. [ Links ]
19. Borrego ME, Short J, House N, Gupchup G, et al. New Mexico pharmacists knowledge, attitudes, and beliefs towards prescribing oral emergency contraception. J Am Pharm Assoc 2006;46:33-43. [ Links ]
20. U.S. Census Bureau. Available at: http://www.census.gov/popest/cities/SUB-EST2004-4.html. (Accessed January 5, 2006). [ Links ]
21. Ratanajamit C, Chongsuvivatwong V. Survey of knowledge and practice on oral contraceptive and emergency contraceptive pills of drugstore personnel in Hat Yai, Thailand. Pharmcoepidemiol Drug Saf 2001;10:149-156. [ Links ]
22. Ralph SG, Preston A, Clarke J. Over-the-counter advice for genital problems: the role of the community pharmacist. Int J STD AIDS 2001;12:513-5. [ Links ]
23. Greenberger M, Vogelstein R. Pharmasict refusals: A threat to womens health. Science 2005;308:1557-8. [ Links ]
24. Summary Of State Actions Related To Pharmacist Refusals. Available at: http://www.plannedparenthood.org/pp2/portal/files/portal/media/factsreports/fact-050418-pharmacist-refusals.xml. (Accessed January 5, 2006). [ Links ]
25. State policies in brief: Refusing to provide health services. New York: Alan Guttmacher Institute, September 1, 2004. Available at: http://www.guttmacher.org/statecenter/spibs/spib_RPHS.pdf (Accessed January 5, 2006). [ Links ]
26. Manasse HR Jr. Conscientious objection and the pharmacist. Science 2005;308:1558-9. [ Links ]
27. Rodrigues I, Grou F, Joly J. Effectiveness of emergency contraceptive pills between 72 and 120 hours after unprotected sexual intercourse. Am J Obstet Gynecol 2001;184:531-7. [ Links ]
28. Sucato GS, Gardner JS, Koepsell TD. Adolescents use of emergency contraception provided by Washington State pharmacists. J Pediatr Adolesc Gynecol 2001;14:163-9. [ Links ]
29. Jones RK, Darroch JE, Henshaw SK. Contraceptive use among U.S. women having abortions in 2000-2001. Perspect on Sex Reprod Health 2002;34:294-303. [ Links ]
30. Raine TR, Harper CC, Rocca CH, et al. Direct access to emergency contraception through pharmacies and effect on unintended pregnancy and STIs: a randomized controlled trial. JAMA 2005;293:54-62. [ Links ]
31. Iffy L. Emergency contraception: politics trumps science at the U.S. Food and Drug Administration. Obstet Gynecol 2004;104:1103-4. [ Links ]
32. Stammers T. Emergency contraception from pharmacists misses opportunity. BMJ 2001;322:1245. [ Links ]
33. Stenchever, MA, Droegemueller W, Herbst AL, Mishell, DR, Jr. Comprehensive Gynecology. 4th ed. St. Louis: Mosby; 2001. p 296. [ Links ]
34. Randomised controlled trial of levonorgestrel versus the Yuzpe regimen of combined oral contraceptives for emergency contraception. Task Force on Postovulatory Methods of Fertility Regulation. Lancet 1998;352:428-33. [ Links ]
35. Glasier A., Baird D. The effects of self-administering emergency contraception. N Engl J Med 1998;339:1-4. [ Links ]
36. Where can a woman go? Reproductive services in Texas hospitals. A Project of Access Texas and the TARAL Education Fund; 2001. [ Links ]

