










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Psychosocial problems, such as anxiety and depression 1 , emotional distress 2 , 3 , past alcohol and substance abuse 4 as well as social isolation 5 are common in transplant candidates and contribute to post-transplant management complexity. 6 , 7 These factors impact health-related quality of life (HRQOL) and biomedical outcomes. 7 , 8 , 9 Methods to proactively identify transplant candidates who are at particular risk of needing complex post-transplant care have to be developed. However, the effectiveness of instruments such as the Psychological Assessment of Candidates for Transplantation (PACT) 10 , the Transplant Evaluation Rating Scale (TERS) 11 or the INTERMED 12 , 13 in identifying patients at risk for unfavourable biomedical outcomes after transplantation has not been shown. Only the Stanford Integrated Psychosocial Assessment for Transplantation (SIPAT) 14 , 15 has found a significant association between psychosocial pre-transplant assessment, rejection episodes and medical hospitalizations. The specific question whether there is an association between pre-transplant assessment and medication adherence was also investigated in this study. The relationship between high SIPAT scores and nonadherence suggested a trend, but was not statistically significant. 14
We have previously reported the utility of the INTERMED for describing liver transplant candidates from a biopsychosocial perspective and identifying complex patients with mood disturbances and reduced HRQOL 16 ; liver transplant patients were the sole common organ group investigated in all participating centres of the study and were therefore chosen as studied population. Among these liver transplant candidates, 38% were detected as complex according to the INTERMED criteria. The INTERMED 17 , 18 is a screening instrument to identify patients with multiple care needs. It is based on the concept of case complexity, which is determined by diagnosis as well as by a variety of other parameters that influence patient management and prognosis, such as chronicity and severity of illness, limitations in daily life, psychiatric comorbidity and social vulnerability.
According to a review, prevalence of reported medication nonadherence is around 28% in kidney transplantation. 19 Early medication adherence 3-months post renal transplantation varies between 93.5% and 84% depending on the complexity of the immunosuppressant treatment (from once-daily regimen to 4 doses per day). 20 Immunosuppressant medication nonadherence, which is partly influenced by psychosocial determinants, is an important trigger of acute rejection and graft loss in solid-organ transplant (SOT) recipients. 19 , 21 , 22 Nonadherence contributes to 20% of late acute rejection episodes and 16% of graft losses in kidney transplantation. 19 In another study in kidney transplant recipients, graft loss due to nonadherence represents 48% of death-censored graft failures beyond 2 years. 21 Hazard risk of graft loss and death increases significantly with fair (HR: 1.63; 95%CI: 1.37-1.93; p<0.0001) or poor (HR: 1.80; 95%CI: 1.52-2.13; p<0.0001) adherence in comparison to good and excellent adherence as measured by pharmacy refills in kidney transplantation. 22 In the Swiss Cohort Transplant study, De Geest et al . reported that self-reported pretransplant medication nonadherence was significantly associated with post-transplant immunosuppressive medication nonadherence among kidney, liver, lung and heart transplant groups (OR: 3.10; 95%CI: 2.29-4.21). 23 Main variables associated with nonadherence were young age 19 , 21 , 22 , social isolation and poor health literacy 19 , depression 24 , non-white recipients 21 but also forgetfulness/interruption of daily routine. 25 Based on the existing evidence in the literature, we sought to determine whether a pre-transplant INTERMED evaluation can identify patients with low medication adherence post-transplantation. We therefore monitored medication adherence and its association with baseline INTERMED scores.
METHODS
The study was approved by the local Ethics Committee (Commission d’Ethique de la Recherche Clinique, Sous-Commission III, session may 22 nd , 2002, protocol: 98/02), and all the participants gave written consent.
Our study reports on a subsample of patients in the aforementioned longitudinal European INTERMED project, referred to in the introduction, which assessed the biopsychosocial profiles of transplant candidates and the prevalence of case complexity. 13 , 16 For the multicentre European INTERMED project, the Lausanne patients were recruited prospectively during the pre-transplant psychiatric evaluation. Every patient who presented to the Transplantation Centre of Lausanne University Hospital (CHUV) for SOT was considered for inclusion, except those who could not be evaluated because of severe cognitive disturbances (exclusion criteria).
For the Lausanne, one-centre substudy, the inclusion criteria applied during the post-transplant hospital stay, were as follows: to take part in the European project in Lausanne and to have benefited from a SOT. Exclusion criteria were deaths during post-SOT hospitalization, patients refusing to use the medication electronic monitor and logistic problems precluding inclusions. In this population, immunosuppressant medication adherence was measured by electronic monitors during the first 12 months post-transplant. Baseline data were collected between 2003 and 2007, and patient follow-up was completed in 2009.
The INTERMED, the first empirically based instrument to link case and care complexity 17 , 18 , is a visual, action-oriented decision-support tool for the assessment of biopsychosocial health risks and health needs. When used by trained health care professionals from different backgrounds, the validity and reliability of the tool has been demonstrated in a variety of medical populations 17 , 18 , 26 , 27 , including liver transplant recipients. 16 The utility of the INTERMED has been demonstrated for detecting complex, medically ill patients at risk for poor HRQOL and decreased response to medical treatment 28 ; it has also proven to be a case-finder for early and beneficial psychosocial interventions. 29 , 30 , 31 The INTERMED (see Table 1 ) classifies information into four domains: biological, psychological, social and health care. Each domain contains two variables related to the patient’s past and current situations and one variable about the patient’s prognosis. The variables are assessed by review of the medical chart and a subsequent 20 minute semi-structured patient interview. They are scored from 0 (no vulnerability / needs) to 3 (severe vulnerability / needs); for each variable, anchor points are defined in a glossary to facilitate scoring. The maximum score for the 20 variables is therefore 60 (range 0 – 60), and the cut-off score for qualifying as a complex patient is set >20. 28 The original English version of the INTERMED has been translated and validated in different languages 18 , 26 and is used in routine clinical practice. 31
Table 1 INTERMED domains and variables
| Domains | History | Current state | Prognoses |
|---|---|---|---|
| Biological | Chronicity | Severity of illness | Complications and life threat |
|
| |||
| Diagnostic uncertainty | Clarity of diagnostic profile | ||
|
| |||
| Psychological | Restrictions in coping | Treatment resistance | Mental health threat |
|
| |||
| Premorbid level of psychiatric dysfunctioning | Severity of psychiatric symptoms | ||
|
| |||
| Social | Family disruption | Residential instability | Social vulnerability |
|
| |||
| Impairment of social support | Impairment of social integration | ||
|
| |||
| Health care | Intensity of prior treatment | Organizational complexity at admission or referral | Care needs |
|
| |||
| Prior treatment experience | Appropriateness of admission or referral | ||
The Medication Event Monitoring System (MEMS) is a tool to measure medication adherence. It consists of an electronic device which records and stores the date and time of each opening of the pill container (MEMS TrackCapTM, MWV Switzerland Ltd.). Compared to other methods for assessing medication adherence, such as questionnaires or plasma drug concentrations, electronic monitors are the only tools which produce reliable, dynamic and “real-time” information on how medication is taken by the patient each day. 32 , 33 , 34 , 35 , 36
To increase reliability, electronic data were reconciled according to an operational manual described elsewhere. 37 , 38 Reconciliation with the pill count and the case report form allowed us to add confirmed pocket doses to the electronic adherence data (i.e., a dose, which the patient takes out of the pillbox to take it later).
Procedure
The face-to-face interview based on the INTERMED was part of the European project. It was conducted by the two first authors of the study (LM, GL), who both worked in the Psychiatric Liaison Service of Lausanne University Hospital; they were familiar with the INTERMED and the standard protocol for using the instrument.
The electronic monitoring of adherence to the immunosuppressant drugs was conducted by the pharmacists (AN, VS, MPS) in the Department of Ambulatory Care & Community Medicine at the University Hospital of Lausanne; these pharmacists run a medication adherence clinic and have research experience with the use of electronic monitors.
After the patients were enrolled in the study by the physician, the patients were referred to the pharmacists who dispensed the prescribed calcineurin inhibitor-based medication (cyclosporine 25, 50 and 100 mg or tacrolimus 0.5, 1 and 5 mg) in the electronic monitors every month for 12 months post-transplantation and explained the correct use of the electronic device. Each dosage was delivered in separate MEMS according to good pharmaceutical practices; electronic data were downloaded monthly and shown as feedback to the patients without any further systematic intervention. This monthly feedback represents standard care in this centre at this time. Additional immunosuppressant medications were not electronically monitored but were delivered according to standard care.
All dosages per patient and day were compiled to obtain the quantity of each drug taken by day compared to the expected dosage (e.g., patient X took 75 mg cyclosporine (Drug taken) on day Y instead of 175 mg (Drug expected)). All changes in drug dosages were taken into account; changes occurred frequently during the 12 months post-transplantation.
Statistical analysis
Sociodemographic and medical variables and INTERMED scores were compared using two-tailed chi-squared tests for categorical data and Mann-Whitney U Tests for continuous data. A two-sided p-value of <0.05 was used to determine statistical significance. For statistical analysis, SPSS, SAS and S-Plus were used.
Immunosuppressant medication adherence and intention-to-treat analysis was performed according to two previously described definitions: persistence and implementation. 39 Persistence is defined as the time from initiation of a studied treatment until discontinuation as determined by electronic adherence monitoring. Patients who stopped cyclosporine/tacrolimus were considered to be non-persistent. Patients whose cyclosporine/tacrolimus prescriptions were changed were considered to be persistent. If patients stopped the study but kept taking their cyclosporine/tacrolimus, they were considered to be persistent.
Implementation was defined as the percentage of persistent patients who did not deviate from the prescribed medication regimen. For each patient, implementation data were summarized in a sequence of binary data indicating yes or no to the question of whether the patient had taken all the medications as prescribed by the physician on day j (1 = correct number of daily opening(s) of all electronic monitors; 0 = less daily openings than prescribed). In case of hospitalization, patients did not use the electronic monitors systematically. As they got their immunosuppressant from the hospital, these periods contained non-detected adherence data. Therefore, these periods were described as non-monitored and censored from the analysis. A logistic generalized estimating equation (GEE) model was implemented to analyse the resulting longitudinal binary data. 40 GEE is the method of choice for analysing data with repeated measures for each patient; this method accounts for the interindividual variability of the measures and can address unbalanced data due to missing values.
Persistence and implementation were described in the 2 groups according to each patient’s INTERMED score (>20 or ≤20).
RESULTS
A total of 52 SOT recipients were approached, all of whom were previously enrolled in the European project (see Figure 1). Median time between the completion of the INTERMED and the SOT was 335 days (Quartiles 25,75: 176, 573; min-max: 28-1199). From that group, 32 patients were included in this study and monitored by MEMS, 22 patients were prescribed tacrolimus twice a day and 10 cyclosporine twice a day at inclusion. Twenty-seven patients completed follow up and were followed for a mean of 332 days.
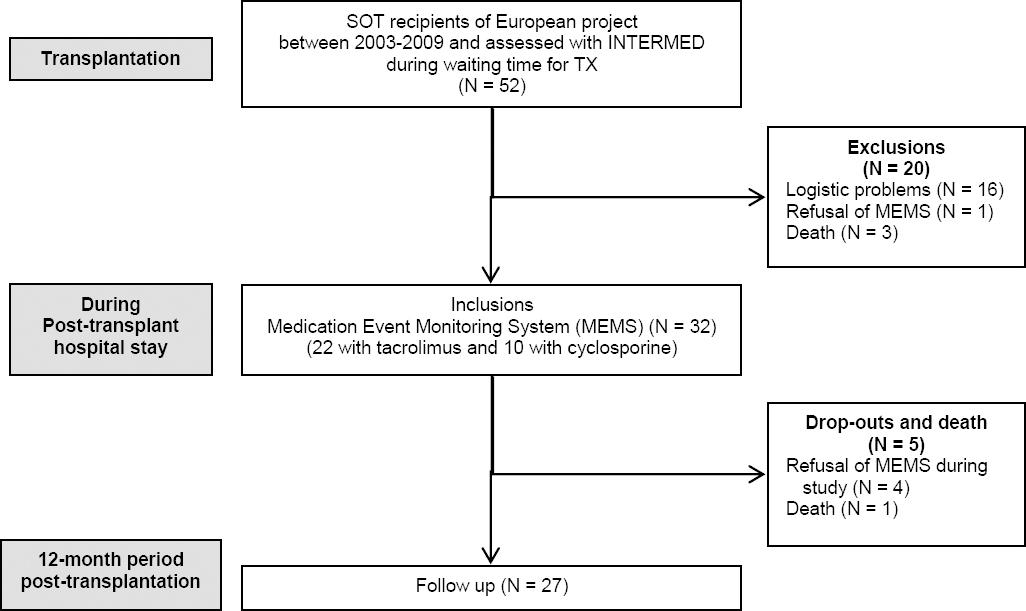
Figure 1 Flow diagram of participants of the study SOT = Solid Organ Transplantation, TX = Transplantation
The patients who were included (N=32) and excluded (N=20) did not differ with regard to age, sex, and type of organ to be transplanted ( Table 2). Because all patients completed the INTERMED baseline assessment, we were able to compare the INTERMED scores between included and excluded patients, and no differences between the two groups were found. However, excluded patients tended to show a higher, meaning worse, psychological score (p=0.069).
Table 2 Differences in sociodemographic and medical variables between included and excluded patients at baseline
| Inclusions (N=32) | Exclusions (N=20) | p | |
|---|---|---|---|
| age M (SD) | 48 years (11) | 52 years (11) | 0.160 1 |
|
| |||
| Sex ratio | 0.350 2 | ||
| % Men | 20 (62.5%) | 15 (75.5%) | |
| % Women | 12 (37.5%) | 5 (25.0%) | |
|
| |||
| Organ (%) | 0.210 2 | ||
| Lung | 7 (21.9%) | 3 (15.0%) | |
| Heart | 8 (25.0%) | 3 (15.0%) | |
| Kidney | 16 (50.0%) | 10 (50.0%) | |
| Liver | 1 (3.1%) | 4 (20.0%) | |
|
| |||
| Number of transplantations (%) | 0.818 2 | ||
| First | 28 (87.5%) | 17 (85.0%) | |
| Second | 3 (9.4%) | 1 (5.0%) | |
| Third | 1 (3.1%) | 1 (5.0%) | |
| Missing data | 0 (0.0%) | 1 (5.0%) | |
|
| |||
| Work status (%) | 0.198 2 | ||
| Employed | 18 (56.3%) | 7 (35.0%) | |
| Unemployed | 13 (40.6%) | 13 (65.0%) | |
| Missing data | 1 (3.1%) | 0 (0%) | |
|
| |||
| Social status (%) | 0.453 2 | ||
| Living alone | 7 (21.9%) | 7 (35.0%) | |
| Living with a partner | 24 (75.0%) | 13 (65.0%) | |
| Missing data | 1 (3.1%) | 0 (0%) | |
|
| |||
| Intermed M (SD) | |||
| Biological | 7.3 (1.2) | 7.3 (1.4) | 0.688 1 |
| Psychological | 3.3 (2.6) | 4.7 (2.8) | 0.062 1 |
| Social | 3.0 (2.1) | 3.1 (2.2) | 0.824 1 |
| Health Care | 4.6 (1.2) | 5.0 (1.4) | 0.232 1 |
| Sumscore | 18.3 (5.2) | 20.2 (5.1) | 0.218 1 |
1Mann – Whitney – U – Test
2Pearson’s chi square
The sociodemographic and clinical comparisons of the included complex (INTERMED>20) and non-complex (INTERMED≤20) patients based on the INTERMED are summarized in Table 3 . The only statistically significant difference was that complex patients were more likely to be unemployed (p 0.037). Regarding the mean scores in the four domains of the INTERMED, complex patients had higher scores in every domain when compared to non-complex patients. Differences were more pronounced for psychological and social domains than for health care and biological domains ( Table 3).
Table 3 Differences between complex (INTERMED>20) and non-complex patients (INTERMED≤20)
| Complex (N=11) | Non-complex (N=21) | p | |
|---|---|---|---|
| Age M (SD) | 50 years (12) | 47 years (11) | 0.366 1 |
|
| |||
| Sex ratio | 0.844 2 | ||
| % Men | 6 (54.5%) | 14 (66.6%) | |
| % Women | 5 (45.4%) | 7 (33.3%) | |
|
| |||
| Organ (%) | 0.874 2 | ||
| Lung | 2 (18.2%) | 5 (23.8%) | |
| Heart | 4 (36.4%) | 4 (19.0%) | |
| Kidney | 5 (45.5%) | 11 (52.4%) | |
| Liver | 0 (0.0%) | 1 (4.8%) | |
|
| |||
| Time on waiting list | 6 months (SD 11) | 3 months (SD 5) | 0.386 1 |
|
| |||
| Number of transplantations (%) | 0.317 2 | ||
| First | 9 (81.8%) | 19 (90.5%) | |
| Second | 2 (18.2%) | 1 (4.8%) | |
| Third | 0 (0.0%) | 1 (4.8%) | |
|
| |||
| Work status (%) | 0.037 2 | ||
| Employed | 4 (36.4%) | 15 (71.4%) | |
| Unemployed | 6 (54.5%) | 6 (28.6%) | |
| Missing data | 1 (9.0%) | 0 (0.0%) | |
|
| |||
| Social status (%) | 0.121 2 | ||
| Living alone | 4 (36.4%) | 3 (14.3%) | |
| Living with a partner | 6 (54.5%) | 18 (85.7%) | |
| Missing data | 1 (9.1%) | 0 (0.0%) | |
|
| |||
| Intermed M (SD) | |||
| Biological | 8.2 (0.8) | 6.9 (1.1) | 0.003 1 |
| Psychological | 5.7 (2.3) | 2.1 (1.8) | 0.000 1 |
| Social | 4.9 (1.7) | 2.0 (1.4) | 0.000 1 |
| Health Care | 5.4 (0.9) | 4.3 (1.2) | 0.022 1 |
| Sumscore | 24.2 (2.7) | 15.4 (3.1) | 0.000 1 |
1Mann–Whitney U Test
2Pearson’s chi squared test
Regarding medication adherence, implementation was 94.2% in non-complex patients versus 87.8% in complex patients (p 0.274) (see Figure 2 ). In terms of medication persistence, only one patient was strictly non-persistent; one member of the non-complex group discontinued after 171 days and died afterwards. Four patients withdrew; two complex patients withdrew early (at 24 and 29 days) because of noncompliance with the use of the electronic monitors, and because of global refusal of proposed care, respectively. Two non-complex patients withdrew later in the study (at 155 and 168 days), both because of noncompliance with the use of the electronic monitors.

DISCUSSION
This is the first study exploring the association between a pre-transplantation INTERMED evaluation and post-transplantation immunosuppressant therapy adherence among patients with kidney, heart, lung and liver transplants. Using an original approach, adherence to all dosages of immunosuppressive medication (cyclosporine or tacrolimus) was monitored and compiled longitudinally for 12 months post-transplant. All prescribed dosage adjustments and non-monitored periods due to frequent hospitalizations were taken into account to reflect daily adherence as accurately as possible.
As previously shown, INTERMED identifies patients at risk for an impaired HRQOL outcome following transplantation. 16 The INTERMED scores and the distribution of complex versus non-complex transplant patients observed in our study were quite comparable to those found in other populations of diabetic patients and orthopaedic trauma individuals at tertiary care centres. 41 , 42 In our population, complex patients had significantly higher scores than non-complex patients, especially regarding psychological (5.7 versus 2.1) and social domains (4.9 versus 2.0), while differences in biological (8.2 versus 6.9) and health care (5.4 versus 4.3) domains, although significant, were less pronounced and therefore less useful in discriminating complex versus non-complex patients. Furthermore, as adherence in chronic patients is known to be influenced by psychological disturbances 43 , 44 and social problems 45 , the appropriateness of using a biopsychosocial tool, such as the INTERMED, rather than a psychosocial tool as the above mentioned SIPAT 14 , 15 has to be questioned. The SIPAT study 14 showed a non-significant correlation between high SIPAT scores and medication nonadherence, therefore research on this question has to continue.
The exploratory results about medication adherence, as measured electronically, show that complex patients identified by INTERMED tend to have lower medication adherence after transplantation vs. non-complex patients. However, due to the small sample size of this study, this finding did not reach statistical significance and thus the hypothesis that complex patients have lower adherence needs to be explored further. We also noted that withdrawals seemed to occur earlier in complex patients compared to non-complex patients (within the first month versus after 5 to 6 months, respectively). Whether withdrawing is the first sign of lower adherence to medication needs to be clarified, as the literature shows that the first rejection tends to occur sooner in patients with lower adherence than in patients with stable adherence. 20 , 21
This study has several limitations. First, it had a relatively high exclusion rate; several patients had to be excluded for medical, organizational and logistic reasons because the wait time between eligibility for transplantation and actual transplant is long. The complex implementation of the protocol requires rigorous interdisciplinary collaboration between pharmacy, liaison psychiatry and the different transplantation subspecialties, and accounts for the fact that 30% of the patients were excluded for logistical reasons. Only 1 out of 5 liver SOT recipients were included because after initiating the study, the Geneva University Hospital became the sole centre for liver transplantation in the French speaking part of Switzerland, thus making follow up in Lausanne impossible. Other studies 23 , 46 , 47 assessing adherence and psychosocial factors in post-transplant patients reported similarly high exclusion rates (between 37.3% and 58.3%). Moreover, the fact that candidates for liver transplantation, who are usually complex due to a high prevalence of substance abuse and its psychosocial consequences, were underrepresented, might have decreased the case complexity of the sample and decreased the statistical power of the INTERMED with regard to medication adherence. Second, the time between the first patient enrollment and the study publication is around ten years, which could call into question the validity of our conclusions. However, because immunosuppressant treatments have not experienced major changes in the last decade 48 , this risk is mitigated. Third, we did not evaluate the association between deviations in timing and the INTERMED complexity score. We decided to do so because of two reasons: 1) more than two-thirds of the included patients were taking tacrolimus, which elimination half-life is long (43 hours), and 2) we focussed on whether or not tacrolimus or cyclosporine were taken daily with the right regimen, taking precisely into account all the different dosages patients were taking as well as all the regimen changes that happened during the 12-month post-transplant. In a further study it would be important to investigate the association between the pre-transplant INTERMED score, immunosuppressant timing and plasma immunosuppressant levels. Indeed, timing could be an interesting proxy to understand in more detail the way patients self-manage their immunosuppressant treatment at home. This might be analysed as a very early trigger for nonadherence, if indeed one can show that timing nonadherence is a predictor of taking nonadherence over time. Fourth, the pharmacists were blinded to the INTERMED score but not to the medication electronic adherence data, as they provided monthly feedback to the patients. However, this minimal intervention was the same for complex and non-complex patients, which should prevent an intervention bias between the two groups.
The study sample size was insufficient to achieve conclusive results. The fact that adherence is lower in complex patients requires to be further investigated because this information is crucial for clinical care both pre- and post-transplantation. Indeed, as in other populations, complex patients identified by means of the INTERMED might benefit from early and targeted psychosocial interventions. 29 Adherence might be increased by interventions such as patient-centred, interprofessional medication adherence programmes dedicated to complex patients.
CONCLUSIONS
This exploratory study gives insight into the complex field of interdisciplinary research in Organ Transplantation. Although the results did not reach statistical significance, they did suggest that the concept of biopsychosocial complexity and the use of the INTERMED in transplantation medicine could be a way to identify pre-transplant patients at risk for post-transplant non-adherence. If such results are confirmed by larger studies, early and targeted interventions could be designed to prevent rejection by addressing adherence before transplantation with complex patients.
Another question that could be addressed in future studies is whether the use of a nonspecific biopsychosocial instrument such as the INTERMED is the most efficient way of detecting adherence problems in the transplant population. As transplant patients generally are highly morbid and in need of complex health care, a more specific instrument that focuses on psychopathology and social issues might be more appropriate. Yet one has to be aware, that splitting psychosocial problems from medical factors increases fragmentation of care. 49
The study design points furthermore to the specific challenge of data collection for researchers working in interdisciplinary transplantation teams. Rigorous communication is a basic requirement for successful interdisciplinary research. Moreover, the fact that transplantation dates are unpredictable and therefore data collection post-transplant cannot be planned might lead to investigators who are overburdened with their dual responsibilities as clinicians and researchers. To prevent the loss of precious data in a population with a naturally high risk of exclusion and withdrawal, future studies gathering interprofessional pre- and post-transplant data should keep this aspect in mind when designing the protocol.

