










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
The scope of practice for pharmacists across the United Kingdom (UK) is widening, with pharmacists in the community now offer healthcare services that far exceed the traditional process of dispensing medicines. Community pharmacies operate under a contract with the National Health Service (NHS). In 2005, a change to the NHS Community Pharmacy Contractual Framework (CPCF) in England and Wales introduced three tiers of pharmaceutical services (essential, advanced, and enhanced).1The aim was to reward high-quality services and utilise the skills of pharmacists and pharmacy staff. All NHS pharmacies must deliver essential services (e.g., dispensing of medicines and promotion of healthy lifestyles) but can choose whether they provide advanced or enhanced services. Enhanced services are locally commissioned according to local need (e.g., palliative care support, care home support) whereas, advanced services may be offered nationally. There are currently six advanced services, two of which, the New Medicines Service (NMS) and Medicines Use Review (MUR), have a shared aim to improve and promote adherence as part of a patient-centred consultation with a pharmacist. Community pharmacies are remunerated GBP 28 per MUR conducted and have, until recently, been capped at a maximum of 400 per annual claim.1The choice of patient to approach for recruitment to MUR is at the discretion of the community pharmacist. However, to achieve payment, 70% must fall into one or more of the national target patient groups: high risk medicines; recently discharged from hospital with changes to their medicines; respiratory disease; and cardiovascular disease.2Providing advanced services, such as MUR, to young people is an ideal opportunity for pharmacists to improve health outcomes, reduce costs to the NHS, such as medicines waste at an early stage.1,2
Older adults are the established focus for pharmacy services. However, children and young people (CYP) make up more than 17% of the UK population which is similar in proportion to those aged over 65 years.3In the 11-15 year-old age group alone, approximately one in four report that they have a long-term condition (LTC).4Common conditions, several of which fall within the MUR national target groups, include asthma, diabetes, epilepsy, arthritis and mental health. Rates of medicine nonadherence in people with LTCs are commonly reported to average at about 50% whereas for children the average increases to around 60%, and for adolescents can be as high as 70%.5 6 7-8MURs may be offered free of charge to any patient, be they adult (>18 years), child (<18 years) or young person (10-24 years), prescribed one or more medicines. Prioritising the health of CYP, especially during transition to adult independence, could be beneficial to their health outcomes later in life. Also it is important that CYP have the knowledge about their medicines to ensure safe usage of medications. Despite their potential, MURs have not been evaluated for CYP specifically and data on advanced pharmacy services uptake by age is not reported.9 10-11
The aim of this study was to investigate the provision of community pharmacy services to CYP with a focus on advanced services such as MUR. Perceptions and experiences of community pharmacists, pharmacy staff, CYP and their parents or carers on the provision of advanced services to CYP were also explored.
METHODS
Four cross-sectional self- administered questionnaires were distributed to UK based pharmacists, pharmacy staff members, CYP and parents of CYP between September and December 2017 (Online appendix). Study approval was obtained from the School of Pharmacy, University of Birmingham Research Ethics Sub-Committee. Willingness to participate was confirmed; the right to withdraw at any stage and maintenance of confidentiality and anonymity was explained to all participants prior to completion of each questionnaire. Participants signed an informed consent to take part in the study.
Questionnaire development and distribution
Two different questionnaires were developed for pharmacists, one for community pharmacy staff and one for CYP and the parents of CYP. The questionnaires were developed by the research team and informed by published literature addressing pharmaceutical care to CYP and pharmacist roles in supporting CYP. Questionnaires contained a series of open, closed, multiple-choice questions and Likert scale responses. Questionnaires were subject to academic review, piloted on a subset of the target audience and revised accordingly prior to distribution.
Pharmacist questionnaires
To minimise bias, pharmacists who took part in the first questionnaire did not take part in the second questionnaire, andvice versa.
Questionnaire 1 focused on obtaining a snapshot of current service provision of pharmacists to CYP, and consisted of 21 questions to collect demographic data and information about pharmaceutical care and pharmacy services offered to CYP, the participant's role and current involvement. Pharmacists were recruited by online survey link dissemination via a UK-wide independent prescriber newsletter and hard-copy distribution by researchers visiting local community pharmacies. While no restriction was placed on the participant's area of practice, the main channels of distribution targeted primary care and community-based pharmacists.
Questionnaire 2 focussed on collection of data relating to advanced service provision to children (<18 years). It comprised 9 questions to collect pharmacy locations and annual figures (period covered 1st April 2016 to 31st March 2017) for the number of MURs conducted with children in community pharmacies and, explore pharmacist experiences and challenges with MUR service provision for children. Convenience sampling was used to target 46 community pharmacies for recruitment of one pharmacist per pharmacy to the study across the West Midlands. Hard copies of questionnaires were distributed during personal visits to community pharmacies.
Pharmacy staff questionnaires
Pharmacy staff were included in the study if they had potential involvement in the recruitment process for pharmacy services such as MURs. This questionnaire (questionnaire 3) included 9 questions to collect pharmacy locations and annual figures (period covered 1stApril 2016 to 31stMarch 2017) for the number of MURs conducted with children in community pharmacies and, explore the community pharmacy staff role, experiences and challenges of recruitment of children for MURs. Pharmacy staff were recruited at the same time as pharmacists for the second questionnaire (described above) during the same researcher visit. A maximum of one member of non-pharmacist staff per pharmacy was recruited and hard copies of the questionnaire were used to collect responses.
Children, young people and parents' questionnaire
Questionnaire 4 included a series of 20 questions and comprising two parts; one part for completion by CYP with long-term conditions and the second for completion by parents. Questions revolved around the long-term condition(s), number and frequency of medicines, and experiences of community pharmacy involvement healthcare provision.
CYP and parents were targeted for recruitment through primary and secondary schools, a university, social media and two community pharmacies. Eight primary and four secondary schools within the East and West Midlands were approached to facilitate recruitment to the study. Participating schools distributed an online link to students and parents via a weekly newsletter. Undergraduate students from the researcher's university were sent a link to the online questionnaire and asked to share. In addition, with the agreement of the community pharmacy proprietors, researchers based themselves in two community pharmacies for one day to recruit participants.
The four questionnaires were distributed by convenience sampling, therefore a sample size calculation was not conducted.
Data analysis
For this study we used the WHO criteria, amended according to UK national law, to define the age ranges of adults (>18 years), children (<18 years), adolescents (10-19 years) and young people (10-24 years). Multiple choice question and Likert scale data were analyzed using SPSS v24 (IBM Corp. in Armonk, NY, USA). Free-text responses to open-ended questions were categorized and quantified. The data gathered from questionnaire 4 from both CYP and parents/carers was combined for analysis of demographic information and prescription collection behaviour. CYP and parent feelings about their knowledge of their/their child's condition and its management was dichotomised into enough and not enough to facilitate analysis. Whether CYP forgot to take their medicines was dichotomised into yes and no in recognition that this question represented a partial indicator of adherence rather than a full validated measure.
The main study outcomes included: current pharmacy services, pharmacy services uptake by CYP, pharmacy staff recruitment into services, experience of CYP with LTCs and their parents with pharmacy services.
Inclusion criteria in this study: pharmacists working in primary care both at community pharmacies and general practice; pharmacy staff working at community pharmacies and involved in the recruitment process for pharmacy services; CYP people with LTCs and parents of CYP with LTCs.
RESULTS
A total 92 pharmacists completed questionnaire 1 investigating current pharmacist roles with CYP. A response rate could not be generated due to the nature of recruitment. Pharmacists responded from all areas of the UK, the main proportion being from the West Midlands. It is notable that most respondents were independent prescribers with the main area of practice primary care. Demographic details are shown inTable 1.
Table 1. Demographic details of pharmacist respondents to questionnaire 1
| Pharmacist respondents | N (%) |
|---|---|
| Geographical area of practice in the UK (n=92) | |
| East Midlands | 8 (8.6) |
| London | 16 (17.3) |
| North East | 6 (6.5) |
| North West | 16 (17.3) |
| West Midlands | 21 (22.8) |
| South East | 8 (8.6) |
| South West | 5 (5.4) |
| Northern Ireland | 4 (4.3) |
| Scotland | 4 (4.3) |
| Wales | 4 (4.3) |
| Prescribing qualification status (n=92) | |
| Non-prescriber | 13 (14.1) |
| Independent prescriber | 79 (85.9) |
| Main area of practice (n=92) | |
| Community pharmacy | 34 (36.9) |
| GP surgery | 58 (63.0) |
Of the 46 pharmacies approached for recruitment to questionnaire 2, 38 pharmacists and 40 non-pharmacist members of pharmacy staff responded. Most respondents were from medium chain pharmacies in high street or town center locations. Demographic details are shown inTable 2.
Table 2. Demographic details of community pharmacy staff respondents to questionnaire 2 and 3
| Pharmacist respondents | Number (%) |
|---|---|
| Location of pharmacy (n=38) | |
| High street | 11 (28.9) |
| Town or city center | 10 (26.3) |
| Within a GP practice | 2 (5.3) |
| Out of town shopping center | 9 (23.7) |
| Supermarket | 2 (5.3) |
| Village | 3 (7.9) |
| Other | 1 (2.6) |
| Type of pharmacy (n=38) | |
| Single independent | 2 (5.3) |
| Small chain (2-10 stores) | 4 (10.6) |
| Medium chain (11-99 stores) | 20 (52.6) |
| Large chain (≥100 stores) | 12 (31.6) |
| Non-pharmacist staff respondents | Number (%) |
| Location of pharmacy (n=40) | |
| High street | 11 (27.5) |
| Town or city center | 12 (30.0) |
| Within a GP practice | 2 (5.0) |
| Out of town shopping center | 8 (20.0) |
| Supermarket | 2 (5.0) |
| Village | 5 (12.5) |
| Other | 0 (0) |
| Type of pharmacy (n=39) | |
| Single independent | 1 (2.6) |
| Small chain (2-10 stores) | 3 (7.7) |
| Medium chain (11-99 stores) | 23 (59.0) |
| Large chain (>100 stores) | 12 (30.8) |
| Job title (n=39) | |
| Dispenser | 29 (74.4) |
| Healthcare assistant/counter assistant | 4 (10.3) |
| Accuracy checking technician | 3 (7.7) |
| Pharmacy technician | 2 (5.1) |
| Pre-registration pharmacist | 1 (2.6) |
One primary school of the 12 schools approached, distributed questionnaire 4 as hard-copies and online links to the parents or carers of 400 students. Due to the online nature of distribution via this and other routes, the number of participants from different recruitment sources and response rates could not be determined. There were a total of 78 responses to the online questionnaire of which 27 were excluded for nonsensical answers or for not meeting inclusion criteria. The age (mean 20.2 years, median 21 years, range 7 to 24 years) of the CYP respondents in this study suggests that most were recruited from the university student population. A total of 18 parents or carers of CYP with long-term conditions participated in this study. The age of the CYP they provided information about was broader (mean 10.2 years, median 9 years, range 2 to 22 years).Table 3shows the characteristics of CYP participants combined with the CYP information provided by parents and carers.
Table 3. Demographic details for CYP from responses to questionnaire 4 CYP
| N (%) | |
|---|---|
| Gender (n=69) | |
| Female | 46 (66.7) |
| Male | 23 (33.3) |
| CYP long-term condition (n=69) | |
| Skin | 19 (27.5) |
| Respiratory | 20 (29.0) |
| Gastrointestinal | 3 (4.3) |
| Mental Health | 20 (29.0) |
| Endocrine | 7 (10.1) |
| Cardiovascular | 1 (1.4) |
| Allergy | 5 (7.2) |
| Other | 6 (8.7) |
| No. of long term conditions per CYP (n=69) | |
| 1 | 58 (84.1) |
| 2 | 10 (14.5) |
| >2 | 1 (1.4) |
| No. of different medicines prescribed (n=69) | |
| 0 | 2 (2.9) |
| 1 | 26 (37.7) |
| 2 | 22 (31.9) |
| 3 | 10 (14.5) |
| 4 or more | 9 (13.0) |
| Frequency of medicine administration (n=69) | |
| Less than once a day | 14 (20.3) |
| Daily, once a day | 28 (40.6) |
| Daily, twice a day or more | 27 (39.1) |
The majority of pharmacists (83/92; 90.2%) reported that they often interacted with CYP with LTCs. The most common conditions that they encountered were asthma (72/92; 78.2%), mental health (47/92; 51.1%), allergies (45/92 48.9%), diabetes (40/92; 43.4%) and epilepsy (36/92; 39.1%). Regarding general promotion of healthy lifestyles specifically to CYP, most pharmacists (73/92; 79.3%), reported involvement in public health advice provision. Advice offered ranged from that demanded as an essential service by the NHS CPCF (e.g. smoking and weight management) to enhanced service provision (e.g. vaccination) and beyond, to advice on alcohol misuse, sexual health and mental health. Despite the high proportion of pharmacists offering such advice to CYP, approximately two-thirds (62/92; 67.3%) felt that they did not have enough support in its provision and more than three-quarters (71/92; 77.2%) wanted additional training. Few pharmacists (13/92; 14.1%) linked to local educational establishments (e.g. schools, colleges, universities) or social care services for CYP in their daily practice.
Participants comprised of 38 pharmacists (response rate 82.6%) and 40 pharmacy staff (response rate 87.0%) were recruited from 41 of the 46 pharmacies visited resulting in 41 annual MUR provision data sets. In the year from 1 April 2016 to 31 March 2017, a total of 40 MURs were conducted with children (<18 years) in only five of 41 community pharmacies. The children recruited for all of these MURs fell into one of two national target groups; patients taking high risk medicines or patients with respiratory disease. The mean number of all MURs conducted per pharmacy in this period was 294.9 (SD 134.2).
In the 36 pharmacies where MURs had only been conducted with adults, pharmacists and pharmacy staff were asked to select potential reasons for not recruiting children to the process.Figure 1shows the reasons selected by both pharmacists and pharmacy staff. For pharmacists, i.e., those responsible for obtaining consent and conducting MURs, consent was the most popular reason chosen (17/29; 58.6%). Lack of guideline clarity (14/29; 48.3%) and training (13/29; 44.8%) were also identified as an issue. Interestingly, a large proportion of both pharmacists (12/29; 41.4%) and pharmacy staff (14/33; 42.4%) did not realise that MURs could be conducted with children. In addition, many of the pharmacy staff who may be involved in recruitment for MURs responded that children were not the target for MURs.
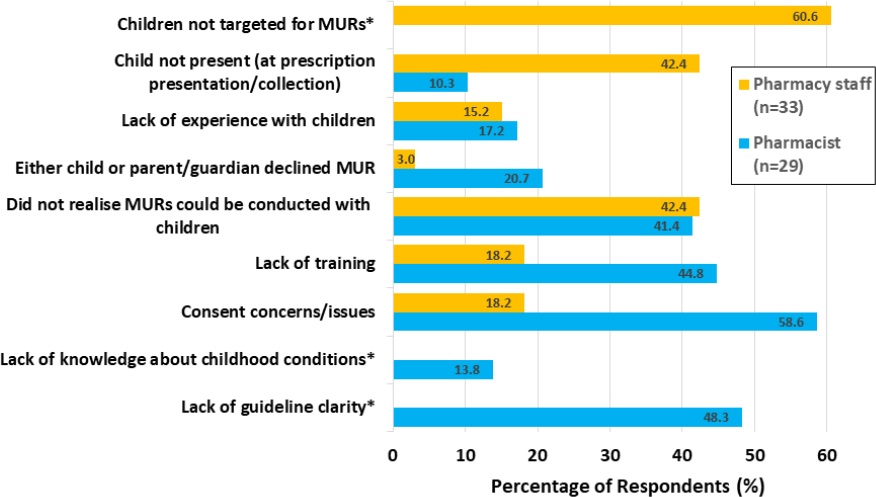
* Different reasons presented according to role in the pharmacy.
Figure 1. Reasons selected by pharmacists and pharmacy staff for not having recruited children for MURs
Despite the low numbers conducted the majority of pharmacists (35/38; 92.1%) were of the opinion that MURs could be of benefit to children. A common theme identified in additional free-text responses was the importance of improving knowledge and understanding for older children. When asked about the challenges of conducting MURs with children, three main themes emerged and had a particular focus on younger children; assessing competency and understanding; obtaining consent and absence of the child.
Although few participants reported themselves as having diabetes, other LTCs were generally as expected for CYP with respiratory (asthma) and mental health issues the most common. As anticipated for this population the majority reported only one LTC. Where more than one LTC was reported, the combinations were mainly associated conditions (e.g., asthma and eczema; depression and anxiety). All CYP reporting to have respiratory disease, named their condition as asthma. All CYP reporting a skin condition in this sample named their condition as eczema. Given the prevalence of asthma (20/69; 29.0%) and eczema (19/69; 27.5%), it is unsurprising that more than half (41/69; 59.4%) were prescribed two or more medicines and the frequency of administration for most was at least once a day (Table 3).
The conditions above were grouped and classified according to WHO ICD 11 classification of disease.12The diseases that fell under the classifications included asthma (Diseases of the respiratory system); mental health depression and anxiety (Mental, behavioural or neurodevelopmental disorders); diabetes (Endocrine, nutritional or metabolic diseases); epilepsy ( Diseases of the nervous system), skin condition (Dermatitis and Eczema) the ICD 11 specific codes are not shown here as such data was not collected.
Most CYP (53/66; 80.3%) felt they had enough knowledge about their condition and its treatment in order to manage it effectively. When asked what healthcare professionals had provided them with information about their LTC and given freedom to choose multiple options, only 29.4% (15/51) selected pharmacist. Responses were similar for parents and carers with 83.3% (15/18) feeling that they had enough knowledge about their child's condition and its management and with 27.8% (5/18) getting information from a pharmacist. One of the aims of advanced pharmacy services such as MUR is to improve adherence. More than half of CYP (31/51; 60.8%) and their parents or carers (9/18; 50.0%) recognised non-adherence, due to forgetfulness, as an issue in their situation. Yet, the majority of CYP (46/51; 90.2%) and parents/carers (17/18; 94.4%) reported they/their children had not taken part in these advanced services even though almost two-thirds (45/68; 66.2%) reported that they tended to use the same pharmacy for supply of prescription medicines.
DISCUSSION
Pharmacists encounter CYP often but the number of MURs conducted with CYP is low. Despite the prevalence of childhood LTCs and pharmacists self-identifying that their interactions are with CYP with the most common LTCs (e.g., asthma), many community pharmacists and pharmacy staff did not realise that MURs could be conducted with children. It is possible, therefore that pharmacists may not have considered the national MUR target groups to include children. Those pharmacists working in a pharmacy that had not conducted MURs with children identified consent issues as the main barrier to recruitment followed by lack of guideline clarity and training. For the few pharmacists/pharmacies that did conduct MURs with patients under 18 years, all of them fell into two of the four national target groups (i.e., taking high risk medicines or respiratory disease).
For those community pharmacists offering public heath advice and MUR to CYP, they reported a need for additional support and training. When coupled with a lack of links to CYP support networks (e.g., schools, universities), and issues of assessing competence and obtaining consent, these are all likely to contribute to the minimal pharmacy service provision and pharmacist advice reported by CYP.
Strengths and limitations
There is limited research published on community pharmacist engagement with young people through the provision of MURs to children in the UK.13,14This study adds to the minimal literature on the provision of advanced services, in particular MUR, for children and starts to provide insight into CYP experiences of adherence-focussed advanced services. All questionnaires contained closed questions with the opportunity for respondents to add extra information as free-text. The four questionnaires were distributed by three different researchers and used varying methods of delivery; hence there was uneven distribution across the UK and the majority of respondents were from a Midlands location. Due to the distribution methods used, response rates could not be obtained for two (questionnaire 1 and 2) of the four questionnaires.
Results of this study were triangulated by gathering information from different pharmacists, pharmacy staff CYP and parents. Data gathered about pharmacist's general experience of dealing with CYP and the services offered from questionnaire 1 included a high proportion of independent prescriber pharmacists. While this was useful to identify emerging roles of primary care pharmacists and the advice they offered, it has limited relation to community pharmacy services. Due to the small numbers of participants no firm conclusions could be drawn however, when questionnaire 1 is considered in combination with questionnaire 2, whose participants were all community pharmacists, and questionnaires 3 and 4 where the participants were all users of community pharmacy services, the data provides an indicative snapshot of the current interactions of pharmacists with CYP and conduct of MURs with children which adds to published literature.
Part of the aim of this study was to investigate the community pharmacist's current role with and services offered to CYP, yet the ages of this group ranges from 2 to 24 years representing a broad array of development, understanding, and competence. To what extent pharmacist and pharmacy staff participants were focussing on lower and upper extremes of this age range when responding to questionnaires cannot be determined. MUR data was collected for those of 18 years and younger (i.e., the definition of a child in the UK) whereas the majority of questionnaire 3 respondents fell within the definition of an adult (i.e., 18 years and older) but according to WHO criteria still met the definition of a young person (10-24 years). Despite the discrepancies in age ranges considered between the different aspects of this study, the experiences of the CYP involved in questionnaire 3 and 4 align with the small numbers of MURs with CYP reported in questionnaire 2. All questionnaires had small sample sizes. In addition, the respondents to questionnaire 3 were likely to be medical, and pharmacy undergraduates where prior knowledge or interest might have biased their interactions with and experience of community pharmacy and the services/advice offered.
Implications for practice
The conventional focus of much community pharmacy activity is directed at adults and the ailments that come with aging.15Pharmacy schemes targeting the young tend to revolve around public health and lifestyle rather than long-term disease and its management.16For this reason, and a general perception that young people are rarely ill, CYP are at risk of being overlooked for advanced pharmacy services. In line with previous UK-based studies, this research shows that it is uncommon for pharmacists to conduct MURs with CYP.13,14Previous research has found that pharmacists and community pharmacy staff did not feel it appropriate to offer adult focussed services to those under 16 years of age.17In contrast, a high proportion of community pharmacists and staff in this study were unaware that their advanced services could be offered to children. Interestingly, previous research has shown a lack of public awareness of pharmacy services as potentially limiting the optimal use of community pharmacies.18,19Awareness, therefore is an issue that needs to be addressed for both pharmacists, their staff and the general public. This lack of awareness could be tackled by providing training on management of LTCs for CYP in continuous development sessions for pharmacists and pharmacy staff. Furthermore, by raising awareness in public health campaigns for the public regarding available pharmacy services. Both pharmacists and pharmacy staff in this study reported the need for additional training as they did not realise that MUR services could be provided to CYP. Previous studies have highlighted the importance of developing paediatric pharmaceutical teaching at both undergraduate curricula and postgraduate education sessions and also at the pre-registration stage for pharmacists.20,21
The question of who may benefit most from advanced services such as MUR is yet to be addressed.22However, CYP, especially those starting to take responsibility for their own health, may stand to benefit more than adults with the same condition by gaining a better understanding of the importance of adherence in disease management at an earlier stage. This research showed that where MURs were conducted with children, asthma was the main reason. The high prevalence of asthma in children (i.e. one in six children between 5 and 14 years) coupled with evidence suggesting this to be one of the few conditions where there is a proven benefit from MUR suggests these patients should be targeted for advanced adherence-focussed pharmacy services.23,24The incidence of mental health issues in this study's CYP population equalled that of asthma. Given the recent recognition of the mental health support needed for CYP there is a missed opportunity in terms of MUR target groups within the CYP population which may need to be considered within national policy.25
Published literature suggests that children above the age of 7 years generally accept advice and communicate well with pharmacists during counselling.26Many children take responsibility and independently manage their medicines for long term conditions with minimal knowledge.27However, non-adherence is reported as higher for children and adolescents than in adults.7,8In addition, there is national recognition of the gaps associated with transition of care from children's to adult's health and social care services.28This makes advanced services specifically targeting adherence issues, such as NMS and MUR, potentially valuable in this group. Astonet al. identified that pharmacists perceived difficulties in taking consent as the most common reason for not conducting NMS or MURs with children.14The same was true of this study where this perception also extended to pharmacy staff. In addition, pharmacists and pharmacy staff in this study perceived that a lack of guideline clarity was also a barrier. Guidelines clearly state that children are eligible if they have the capacity to engage in the process and able to consent.2Adolescents, in particular, are likely to understand their medicines, communicate at an appropriate level and provide consent. However, the potential subjectivity associated with competence assessment and consent could, in part, account for the feelings that guidelines and training are not adequate for conducting MURs with CYP. Further guidance on assessing competence and obtaining appropriate consent may be necessary for pharmacists to give them the confidence in performing these tasks in such potentially vulnerable groups
US studies report that children either do not visit community pharmacies, or only accompany their parents to pick up their medication only 29% of the time.26,29This has also been identified as a barrier to building long-term relationships and engaging with young people with LTCs in the UK community pharmacy setting.30While many children with LTCs may not present to a community pharmacy, this study suggests that CYP and their parents/carers, tend to use the same pharmacy to collect their prescriptions. Importantly then, a community pharmacist is likely to remain a constant during a child's development and possibly during the potentially difficult transition from child to adult healthcare services. Guidance for advanced services such, as MUR and NMS, currently states that they must be conducted by a pharmacist with the patient and not in the presence of a parent or carer. Removing this requirement and allowing consultations in the presence of parents and carers is suggested as a way to facilitate the transition of care and handover of responsibility for medicines from parent/carer to child. This would, however, require some comprehensive guidance and for pharmacists about how to implement and gain consent from all parties and on how to deal with the complexities of the parent/carer and child relationship. In addition, community pharmacists would need to build the essential links to primary care, social care, and educational establishments that this study shows are currently missing in their daily practice.
From the pharmacist's perspective issues associated with non-adherence in a younger patient may appear more difficult to tackle than for older adults. Even though this group tends to take fewer medicines, without the strategies for communication and experience of dealing with younger patients pharmacists may feel unequipped to interact. This study and others focussing on adolescents found that pharmacists feel inadequately trained when it comes to dealing with young people.31,32This suggests that pharmacists may need further experience and training in dealing with children, child health issues, and consent as part of the accreditation process for such advanced services. Incorporating these topics into training for accreditation would in turn, raise awareness that children may be eligible for advanced services.
Over the next few years MURs conducted by community pharmacists are being phased out in the UK to be replaced by enhanced structured medication reviews.33It is intended that these will be carried out by clinical pharmacists working within primary care networks under new GP contractual arrangements. Despite a new route to delivery by a different group of pharmacists, the findings of this study remain relevant. CYP with LTC require medicines review and, due to potentially higher non-adherence rates than for adults, their conduct may have a greater impact on longer term clinical outcomes than for adults with the same condition.
CONCLUSIONS
Research is needed to provide evidence for the efficacy of all medicine reviews which would ideally be stratified by age and LTC. The pharmacists conducting reviews need training, not only in communicating with CYP across all age ranges but importantly in the process of assessing competence and consent.

